
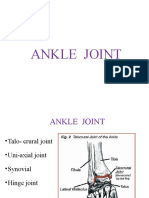
Ankle Anatomy
Ankle Anatomy
You might also like
- Grandpas Farm (Possible Worlds Games) - UV6yOlDocument28 pagesGrandpas Farm (Possible Worlds Games) - UV6yOlhjorhrafnNo ratings yet
- Volo's Guide To Monsters - 1Document7 pagesVolo's Guide To Monsters - 1Saz100% (1)
- Reading Exercise 1Document5 pagesReading Exercise 1Ghazy Muammar Fawwaz Fawwaz67% (3)
- Ankle Joint: Types, Capsule, Kigaments, Synovial Mmebrane - Blood Suply, Nerve Supply, Movements and Important RelationsDocument16 pagesAnkle Joint: Types, Capsule, Kigaments, Synovial Mmebrane - Blood Suply, Nerve Supply, Movements and Important RelationsaminaNo ratings yet
- Ankle Anatomy and Blood Supply of TalusDocument66 pagesAnkle Anatomy and Blood Supply of TalusShashank29 LakkalaNo ratings yet
- L12Document45 pagesL12Ahmed El goharyNo ratings yet
- Ankle Foot BiomechanicsDocument38 pagesAnkle Foot BiomechanicsAnish BishwakarmaNo ratings yet
- Bones of The Lower Limbs2 3 FINALLYDocument26 pagesBones of The Lower Limbs2 3 FINALLYolamidealapa2608No ratings yet
- Session12 - Foot and Ankle BiomechanicsDocument33 pagesSession12 - Foot and Ankle Biomechanicsbirijik7979No ratings yet
- Ankle & Foot MechanicsDocument47 pagesAnkle & Foot MechanicsAhmed El goharyNo ratings yet
- Ankle ComplexDocument95 pagesAnkle ComplexMangala Prema MohanarangamNo ratings yet
- Ankle Power PointDocument36 pagesAnkle Power PointjermaineNo ratings yet
- Arthrologi Blok 7 Tahun 2016 Edit IdaDocument59 pagesArthrologi Blok 7 Tahun 2016 Edit IdaNURHAYATUNISAHNo ratings yet
- Ankle JointDocument31 pagesAnkle JointdanielnawethiNo ratings yet
- Articular System DyahDocument59 pagesArticular System DyahWhydia Wedha SutedjaNo ratings yet
- The Knee Joint and Popliteal FossaDocument18 pagesThe Knee Joint and Popliteal Fossaolamidealapa2608No ratings yet
- Ankle JointDocument29 pagesAnkle JointRamakrishnanNo ratings yet
- Anatomy of FeetDocument22 pagesAnatomy of FeetsherysheryyNo ratings yet
- Arches of The FootDocument17 pagesArches of The FootchibuyeNo ratings yet
- Anatomy Biomechanics of AnkleDocument82 pagesAnatomy Biomechanics of AnklelypiheNo ratings yet
- Arches of Foot: DR M Idris SiddiquiDocument22 pagesArches of Foot: DR M Idris SiddiquiSivabharathi SivanandamNo ratings yet
- Hip Joint 2Document25 pagesHip Joint 2justin sundayNo ratings yet
- Anatomy of Hip and Knee Joint and Popliteal Fossa: Prof. Dr. Nabil KhourDocument49 pagesAnatomy of Hip and Knee Joint and Popliteal Fossa: Prof. Dr. Nabil KhourBadria Al-najiNo ratings yet
- Ankle JointDocument39 pagesAnkle Jointheena solankiNo ratings yet
- Lower Limb BONESDocument79 pagesLower Limb BONESDr.Kumar Satish Ravi100% (1)
- Skeletal System: Cebu Doctors' University - CAMS Department of Medical TechnologyDocument46 pagesSkeletal System: Cebu Doctors' University - CAMS Department of Medical TechnologyJoshua CodillaNo ratings yet
- Foot and Ankle Bones and JointsDocument43 pagesFoot and Ankle Bones and Jointshannah murphyNo ratings yet
- Joints of The Lower Limbs and Joint Classification FinalmDocument27 pagesJoints of The Lower Limbs and Joint Classification Finalmolamidealapa2608No ratings yet
- Arches of FootDocument75 pagesArches of Footvaibhav gowdaNo ratings yet
- Biomechanics Thefoot and Ankle UnitDocument19 pagesBiomechanics Thefoot and Ankle Unitshannithushan43No ratings yet
- Hip JointDocument25 pagesHip JointHashim OmarNo ratings yet
- Hip JointDocument25 pagesHip JointHashim OmarNo ratings yet
- Physical Examination of The Ankle and Foot. JohanesDocument58 pagesPhysical Examination of The Ankle and Foot. JohanesSaaldy ReivanNo ratings yet
- Lower ExtremityDocument75 pagesLower ExtremityRiri Sandra ZannawaNo ratings yet
- Anatomy of The Lower Limb: by Dr. G. TowoDocument146 pagesAnatomy of The Lower Limb: by Dr. G. TowoVuluwa GeorgeNo ratings yet
- Anatomy of Knee JointDocument17 pagesAnatomy of Knee JointSiti AisyahNo ratings yet
- Back of LegDocument21 pagesBack of LegDr MohammedNo ratings yet
- 13 Anatomy Lower Limb BonesDocument50 pages13 Anatomy Lower Limb BonesAzizat MajolagbeNo ratings yet
- Hip DislocationDocument67 pagesHip DislocationKJ Iza (KJ Nurshariza HPSF)No ratings yet
- Anatomy and PhysiologyDocument4 pagesAnatomy and PhysiologySarah CabalquintoNo ratings yet
- Kinesiology Ankle and Foot WULDocument46 pagesKinesiology Ankle and Foot WULwulandari pramanaNo ratings yet
- Archs of The Foot - May 023Document33 pagesArchs of The Foot - May 023mrizvi334No ratings yet
- AnkleDocument6 pagesAnkleitoolNo ratings yet
- The Tibiofibular JointsDocument7 pagesThe Tibiofibular JointsVictor Espinosa BuendiaNo ratings yet
- Sole of The Foot and Arches of TheDocument24 pagesSole of The Foot and Arches of TheDrakeNo ratings yet
- Arches of FootDocument21 pagesArches of Footfilza farheenNo ratings yet
- Lecture 8Document99 pagesLecture 8bolivarsefNo ratings yet
- Bio-Mechanics of Ankle-Foot JointDocument70 pagesBio-Mechanics of Ankle-Foot JointIipo ChennaiNo ratings yet
- 1 Lower Limb BONESDocument79 pages1 Lower Limb BONESZaid AbdulqadirNo ratings yet
- Human Skeletal System PPTDocument73 pagesHuman Skeletal System PPTInsatiable CleeNo ratings yet
- Joints of The Lower LimbDocument63 pagesJoints of The Lower LimbEliud MbuteNo ratings yet
- Anatomy of Foot: Javaid Iqbal PGR-Paediatric SurgeryDocument36 pagesAnatomy of Foot: Javaid Iqbal PGR-Paediatric SurgeryJavaid KhanNo ratings yet
- Lower LimbDocument53 pagesLower LimbRupesh M DasNo ratings yet
- Soleus) Which Insert Onto Its Posterior Surface Via The Achilles TendonDocument7 pagesSoleus) Which Insert Onto Its Posterior Surface Via The Achilles TendonmanandndnNo ratings yet
- Lecture 12 Skeletal System Lower Limb (Structure Function)Document23 pagesLecture 12 Skeletal System Lower Limb (Structure Function)hafiz patahNo ratings yet
- EXSC 322 - Ankle & Foot Part 1Document52 pagesEXSC 322 - Ankle & Foot Part 1ChelseyNo ratings yet
- Week 2 Lecture Osteology, FootDocument85 pagesWeek 2 Lecture Osteology, Footolle3870No ratings yet
- Ankle JointDocument84 pagesAnkle JointPoojitha reddy MunnangiNo ratings yet
- Bio Mechanics of Ankle and FootDocument84 pagesBio Mechanics of Ankle and FootOnwaree Ing100% (6)
- Arthrology of The FootDocument55 pagesArthrology of The Footolle3870No ratings yet
- Skeletal System Shoulder and Arm PPTDocument23 pagesSkeletal System Shoulder and Arm PPTInsatiable CleeNo ratings yet
- Healthy Hips Handbook: Exercises for Treating and Preventing Common Hip Joint InjuriesFrom EverandHealthy Hips Handbook: Exercises for Treating and Preventing Common Hip Joint InjuriesNo ratings yet
- Units Or: 1 Which IsDocument5 pagesUnits Or: 1 Which IsTanvi PriyaNo ratings yet
- A User-Friendly Classification: The Irregular Verbs in EnglishDocument10 pagesA User-Friendly Classification: The Irregular Verbs in EnglishPabloNo ratings yet
- MYCOBIT Control Objective Assessment FormsDocument5 pagesMYCOBIT Control Objective Assessment FormsRafasaxNo ratings yet
- Rekayasa IdeDocument21 pagesRekayasa IdelilyNo ratings yet
- Aluminium Phosphide, A Highly Hazardous Pesticide, and A Suicide Poison in Southern Province of ZambiaDocument2 pagesAluminium Phosphide, A Highly Hazardous Pesticide, and A Suicide Poison in Southern Province of ZambiaSimon TemboNo ratings yet
- Opera Omnia Desiderii Erasmi 1.1Document704 pagesOpera Omnia Desiderii Erasmi 1.1Professore2100% (1)
- MR Robert Sheaffer - Bad UFOs - Critical Thinking About UFO Claims-CreateSpace Independent Publishing Platform (2015)Document331 pagesMR Robert Sheaffer - Bad UFOs - Critical Thinking About UFO Claims-CreateSpace Independent Publishing Platform (2015)María Eugenia LivaNo ratings yet
- Rephrasing Exercises Second TermDocument6 pagesRephrasing Exercises Second TermLulu SancNo ratings yet
- Hardrock Fabrication (P) Limited: SL - NO. Part No. Description TA66096Document5 pagesHardrock Fabrication (P) Limited: SL - NO. Part No. Description TA66096AMSONIC ROCKSNo ratings yet
- Film - The GuardianDocument1 pageFilm - The GuardianfisoxenekNo ratings yet
- High Court of Judicature at Allahabad: Case Status - CRIMINAL MISC. BAIL APPLICATION (BAIL) - (23700/2022)Document2 pagesHigh Court of Judicature at Allahabad: Case Status - CRIMINAL MISC. BAIL APPLICATION (BAIL) - (23700/2022)Ritesh SinghNo ratings yet
- Oh The Tooth That One Ths Was A Story About Place ValueDocument9 pagesOh The Tooth That One Ths Was A Story About Place Valuecagena7907No ratings yet
- 10 Female Superheroes Who Depict Women EmpowermentDocument3 pages10 Female Superheroes Who Depict Women EmpowermentSharjeel ZamanNo ratings yet
- Dont Be Fuuld by JuuLDocument3 pagesDont Be Fuuld by JuuLGabriel ParksNo ratings yet
- (With Script) June 2021 Saturday WSF Teaching GuideDocument3 pages(With Script) June 2021 Saturday WSF Teaching GuideMichael T. BelloNo ratings yet
- Top 10 Best Fighter JetsDocument14 pagesTop 10 Best Fighter JetsArooj fatimaNo ratings yet
- Ancient IndiaDocument9 pagesAncient IndiaAchanger AcherNo ratings yet
- Welcome To Fourtower Bridge: A Paths Peculiar Module For Fantasy Roleplaying GamesDocument7 pagesWelcome To Fourtower Bridge: A Paths Peculiar Module For Fantasy Roleplaying GamesTapanco BarerraNo ratings yet
- Uoc Annual Report 2018Document112 pagesUoc Annual Report 2018GitanjaliNo ratings yet
- Fuji ManualDocument166 pagesFuji Manualasbel gamNo ratings yet
- DeputationDocument8 pagesDeputationAnand MauryaNo ratings yet
- 1.publications All BranchesDocument25 pages1.publications All BranchesNaresh GollapalliNo ratings yet
- Lesson 1-SSP 113Document10 pagesLesson 1-SSP 113Jan Lester DemaalaNo ratings yet
- Answer Module 1Document3 pagesAnswer Module 1endroNo ratings yet
- Spare Parts CatalogueDocument45 pagesSpare Parts CatalogueАлексей ДомнинNo ratings yet
- Introduction To Business ResearchDocument23 pagesIntroduction To Business ResearchKhalid ElGhazouliNo ratings yet
- Mirantis CKA ExamDocument10 pagesMirantis CKA ExamvNo ratings yet























































































Download as pdf or txt
You might also like
- Grandpas Farm (Possible Worlds Games) - UV6yOlDocument28 pagesGrandpas Farm (Possible Worlds Games) - UV6yOlhjorhrafnNo ratings yet
- Volo's Guide To Monsters - 1Document7 pagesVolo's Guide To Monsters - 1Saz100% (1)
- Reading Exercise 1Document5 pagesReading Exercise 1Ghazy Muammar Fawwaz Fawwaz67% (3)
- Ankle Joint: Types, Capsule, Kigaments, Synovial Mmebrane - Blood Suply, Nerve Supply, Movements and Important RelationsDocument16 pagesAnkle Joint: Types, Capsule, Kigaments, Synovial Mmebrane - Blood Suply, Nerve Supply, Movements and Important RelationsaminaNo ratings yet
- Ankle Anatomy and Blood Supply of TalusDocument66 pagesAnkle Anatomy and Blood Supply of TalusShashank29 LakkalaNo ratings yet
- L12Document45 pagesL12Ahmed El goharyNo ratings yet
- Ankle Foot BiomechanicsDocument38 pagesAnkle Foot BiomechanicsAnish BishwakarmaNo ratings yet
- Bones of The Lower Limbs2 3 FINALLYDocument26 pagesBones of The Lower Limbs2 3 FINALLYolamidealapa2608No ratings yet
- Session12 - Foot and Ankle BiomechanicsDocument33 pagesSession12 - Foot and Ankle Biomechanicsbirijik7979No ratings yet
- Ankle & Foot MechanicsDocument47 pagesAnkle & Foot MechanicsAhmed El goharyNo ratings yet
- Ankle ComplexDocument95 pagesAnkle ComplexMangala Prema MohanarangamNo ratings yet
- Ankle Power PointDocument36 pagesAnkle Power PointjermaineNo ratings yet
- Arthrologi Blok 7 Tahun 2016 Edit IdaDocument59 pagesArthrologi Blok 7 Tahun 2016 Edit IdaNURHAYATUNISAHNo ratings yet
- Ankle JointDocument31 pagesAnkle JointdanielnawethiNo ratings yet
- Articular System DyahDocument59 pagesArticular System DyahWhydia Wedha SutedjaNo ratings yet
- The Knee Joint and Popliteal FossaDocument18 pagesThe Knee Joint and Popliteal Fossaolamidealapa2608No ratings yet
- Ankle JointDocument29 pagesAnkle JointRamakrishnanNo ratings yet
- Anatomy of FeetDocument22 pagesAnatomy of FeetsherysheryyNo ratings yet
- Arches of The FootDocument17 pagesArches of The FootchibuyeNo ratings yet
- Anatomy Biomechanics of AnkleDocument82 pagesAnatomy Biomechanics of AnklelypiheNo ratings yet
- Arches of Foot: DR M Idris SiddiquiDocument22 pagesArches of Foot: DR M Idris SiddiquiSivabharathi SivanandamNo ratings yet
- Hip Joint 2Document25 pagesHip Joint 2justin sundayNo ratings yet
- Anatomy of Hip and Knee Joint and Popliteal Fossa: Prof. Dr. Nabil KhourDocument49 pagesAnatomy of Hip and Knee Joint and Popliteal Fossa: Prof. Dr. Nabil KhourBadria Al-najiNo ratings yet
- Ankle JointDocument39 pagesAnkle Jointheena solankiNo ratings yet
- Lower Limb BONESDocument79 pagesLower Limb BONESDr.Kumar Satish Ravi100% (1)
- Skeletal System: Cebu Doctors' University - CAMS Department of Medical TechnologyDocument46 pagesSkeletal System: Cebu Doctors' University - CAMS Department of Medical TechnologyJoshua CodillaNo ratings yet
- Foot and Ankle Bones and JointsDocument43 pagesFoot and Ankle Bones and Jointshannah murphyNo ratings yet
- Joints of The Lower Limbs and Joint Classification FinalmDocument27 pagesJoints of The Lower Limbs and Joint Classification Finalmolamidealapa2608No ratings yet
- Arches of FootDocument75 pagesArches of Footvaibhav gowdaNo ratings yet
- Biomechanics Thefoot and Ankle UnitDocument19 pagesBiomechanics Thefoot and Ankle Unitshannithushan43No ratings yet
- Hip JointDocument25 pagesHip JointHashim OmarNo ratings yet
- Hip JointDocument25 pagesHip JointHashim OmarNo ratings yet
- Physical Examination of The Ankle and Foot. JohanesDocument58 pagesPhysical Examination of The Ankle and Foot. JohanesSaaldy ReivanNo ratings yet
- Lower ExtremityDocument75 pagesLower ExtremityRiri Sandra ZannawaNo ratings yet
- Anatomy of The Lower Limb: by Dr. G. TowoDocument146 pagesAnatomy of The Lower Limb: by Dr. G. TowoVuluwa GeorgeNo ratings yet
- Anatomy of Knee JointDocument17 pagesAnatomy of Knee JointSiti AisyahNo ratings yet
- Back of LegDocument21 pagesBack of LegDr MohammedNo ratings yet
- 13 Anatomy Lower Limb BonesDocument50 pages13 Anatomy Lower Limb BonesAzizat MajolagbeNo ratings yet
- Hip DislocationDocument67 pagesHip DislocationKJ Iza (KJ Nurshariza HPSF)No ratings yet
- Anatomy and PhysiologyDocument4 pagesAnatomy and PhysiologySarah CabalquintoNo ratings yet
- Kinesiology Ankle and Foot WULDocument46 pagesKinesiology Ankle and Foot WULwulandari pramanaNo ratings yet
- Archs of The Foot - May 023Document33 pagesArchs of The Foot - May 023mrizvi334No ratings yet
- AnkleDocument6 pagesAnkleitoolNo ratings yet
- The Tibiofibular JointsDocument7 pagesThe Tibiofibular JointsVictor Espinosa BuendiaNo ratings yet
- Sole of The Foot and Arches of TheDocument24 pagesSole of The Foot and Arches of TheDrakeNo ratings yet
- Arches of FootDocument21 pagesArches of Footfilza farheenNo ratings yet
- Lecture 8Document99 pagesLecture 8bolivarsefNo ratings yet
- Bio-Mechanics of Ankle-Foot JointDocument70 pagesBio-Mechanics of Ankle-Foot JointIipo ChennaiNo ratings yet
- 1 Lower Limb BONESDocument79 pages1 Lower Limb BONESZaid AbdulqadirNo ratings yet
- Human Skeletal System PPTDocument73 pagesHuman Skeletal System PPTInsatiable CleeNo ratings yet
- Joints of The Lower LimbDocument63 pagesJoints of The Lower LimbEliud MbuteNo ratings yet
- Anatomy of Foot: Javaid Iqbal PGR-Paediatric SurgeryDocument36 pagesAnatomy of Foot: Javaid Iqbal PGR-Paediatric SurgeryJavaid KhanNo ratings yet
- Lower LimbDocument53 pagesLower LimbRupesh M DasNo ratings yet
- Soleus) Which Insert Onto Its Posterior Surface Via The Achilles TendonDocument7 pagesSoleus) Which Insert Onto Its Posterior Surface Via The Achilles TendonmanandndnNo ratings yet
- Lecture 12 Skeletal System Lower Limb (Structure Function)Document23 pagesLecture 12 Skeletal System Lower Limb (Structure Function)hafiz patahNo ratings yet
- EXSC 322 - Ankle & Foot Part 1Document52 pagesEXSC 322 - Ankle & Foot Part 1ChelseyNo ratings yet
- Week 2 Lecture Osteology, FootDocument85 pagesWeek 2 Lecture Osteology, Footolle3870No ratings yet
- Ankle JointDocument84 pagesAnkle JointPoojitha reddy MunnangiNo ratings yet
- Bio Mechanics of Ankle and FootDocument84 pagesBio Mechanics of Ankle and FootOnwaree Ing100% (6)
- Arthrology of The FootDocument55 pagesArthrology of The Footolle3870No ratings yet
- Skeletal System Shoulder and Arm PPTDocument23 pagesSkeletal System Shoulder and Arm PPTInsatiable CleeNo ratings yet
- Healthy Hips Handbook: Exercises for Treating and Preventing Common Hip Joint InjuriesFrom EverandHealthy Hips Handbook: Exercises for Treating and Preventing Common Hip Joint InjuriesNo ratings yet
- Units Or: 1 Which IsDocument5 pagesUnits Or: 1 Which IsTanvi PriyaNo ratings yet
- A User-Friendly Classification: The Irregular Verbs in EnglishDocument10 pagesA User-Friendly Classification: The Irregular Verbs in EnglishPabloNo ratings yet
- MYCOBIT Control Objective Assessment FormsDocument5 pagesMYCOBIT Control Objective Assessment FormsRafasaxNo ratings yet
- Rekayasa IdeDocument21 pagesRekayasa IdelilyNo ratings yet
- Aluminium Phosphide, A Highly Hazardous Pesticide, and A Suicide Poison in Southern Province of ZambiaDocument2 pagesAluminium Phosphide, A Highly Hazardous Pesticide, and A Suicide Poison in Southern Province of ZambiaSimon TemboNo ratings yet
- Opera Omnia Desiderii Erasmi 1.1Document704 pagesOpera Omnia Desiderii Erasmi 1.1Professore2100% (1)
- MR Robert Sheaffer - Bad UFOs - Critical Thinking About UFO Claims-CreateSpace Independent Publishing Platform (2015)Document331 pagesMR Robert Sheaffer - Bad UFOs - Critical Thinking About UFO Claims-CreateSpace Independent Publishing Platform (2015)María Eugenia LivaNo ratings yet
- Rephrasing Exercises Second TermDocument6 pagesRephrasing Exercises Second TermLulu SancNo ratings yet
- Hardrock Fabrication (P) Limited: SL - NO. Part No. Description TA66096Document5 pagesHardrock Fabrication (P) Limited: SL - NO. Part No. Description TA66096AMSONIC ROCKSNo ratings yet
- Film - The GuardianDocument1 pageFilm - The GuardianfisoxenekNo ratings yet
- High Court of Judicature at Allahabad: Case Status - CRIMINAL MISC. BAIL APPLICATION (BAIL) - (23700/2022)Document2 pagesHigh Court of Judicature at Allahabad: Case Status - CRIMINAL MISC. BAIL APPLICATION (BAIL) - (23700/2022)Ritesh SinghNo ratings yet
- Oh The Tooth That One Ths Was A Story About Place ValueDocument9 pagesOh The Tooth That One Ths Was A Story About Place Valuecagena7907No ratings yet
- 10 Female Superheroes Who Depict Women EmpowermentDocument3 pages10 Female Superheroes Who Depict Women EmpowermentSharjeel ZamanNo ratings yet
- Dont Be Fuuld by JuuLDocument3 pagesDont Be Fuuld by JuuLGabriel ParksNo ratings yet
- (With Script) June 2021 Saturday WSF Teaching GuideDocument3 pages(With Script) June 2021 Saturday WSF Teaching GuideMichael T. BelloNo ratings yet
- Top 10 Best Fighter JetsDocument14 pagesTop 10 Best Fighter JetsArooj fatimaNo ratings yet
- Ancient IndiaDocument9 pagesAncient IndiaAchanger AcherNo ratings yet
- Welcome To Fourtower Bridge: A Paths Peculiar Module For Fantasy Roleplaying GamesDocument7 pagesWelcome To Fourtower Bridge: A Paths Peculiar Module For Fantasy Roleplaying GamesTapanco BarerraNo ratings yet
- Uoc Annual Report 2018Document112 pagesUoc Annual Report 2018GitanjaliNo ratings yet
- Fuji ManualDocument166 pagesFuji Manualasbel gamNo ratings yet
- DeputationDocument8 pagesDeputationAnand MauryaNo ratings yet
- 1.publications All BranchesDocument25 pages1.publications All BranchesNaresh GollapalliNo ratings yet
- Lesson 1-SSP 113Document10 pagesLesson 1-SSP 113Jan Lester DemaalaNo ratings yet
- Answer Module 1Document3 pagesAnswer Module 1endroNo ratings yet
- Spare Parts CatalogueDocument45 pagesSpare Parts CatalogueАлексей ДомнинNo ratings yet
- Introduction To Business ResearchDocument23 pagesIntroduction To Business ResearchKhalid ElGhazouliNo ratings yet
- Mirantis CKA ExamDocument10 pagesMirantis CKA ExamvNo ratings yet