Download as pdf or txt
You might also like
- Chapter 35 Health PhysicsDocument10 pagesChapter 35 Health PhysicsMegNo ratings yet
- Marine Fouling and Its Prevention Woods Hole Oceanagraphic 1952Document391 pagesMarine Fouling and Its Prevention Woods Hole Oceanagraphic 1952Lucy JonesNo ratings yet
- Rapid Pathogen Detection by Metagenomic Next-Generation Sequencing of Infected Body FluidsDocument26 pagesRapid Pathogen Detection by Metagenomic Next-Generation Sequencing of Infected Body FluidsLuisNo ratings yet
- CARIOLOGYDocument77 pagesCARIOLOGYteklay100% (3)
- 1 s2.0 S0167701206000224 MainDocument9 pages1 s2.0 S0167701206000224 MainGirish Kishor PaiNo ratings yet
- ASMNGS 2018 AbstractsDocument187 pagesASMNGS 2018 AbstractsturnersdNo ratings yet
- Utility of Mycobacterium Tuberculosis PCR in Rul - 2020 - Journal of Clinical TuDocument5 pagesUtility of Mycobacterium Tuberculosis PCR in Rul - 2020 - Journal of Clinical TuKarina ChristantoNo ratings yet
- Influenzae, and Streptococcus Pneumoniae in Suspected CasesDocument6 pagesInfluenzae, and Streptococcus Pneumoniae in Suspected CasesMatiasNo ratings yet
- Clinchem 2017 273698 FullDocument10 pagesClinchem 2017 273698 FullMaisyaroh SaragihNo ratings yet
- Lembar Jawaban SoalDocument5 pagesLembar Jawaban SoalWahyuNo ratings yet
- Biosensors and BioelectronicsDocument8 pagesBiosensors and BioelectronicsochaNo ratings yet
- Liquid Biopsy For Infectious Diseases - A Focus On Microbial Cell-Free DNA SequencingDocument13 pagesLiquid Biopsy For Infectious Diseases - A Focus On Microbial Cell-Free DNA Sequencingmicrobehunter007No ratings yet
- UntitledDocument10 pagesUntitledLalainasoa Odile RivoarilalaNo ratings yet
- Wa0011.Document11 pagesWa0011.umayamajidNo ratings yet
- A New Point-Of-Care Test For The Rapid Detection of Urinary Tract InfectionsDocument8 pagesA New Point-Of-Care Test For The Rapid Detection of Urinary Tract InfectionsAntika CahyatiNo ratings yet
- Penelitian AbstraktifDocument9 pagesPenelitian AbstraktifYondi Piter PapulungNo ratings yet
- Jamal 2014Document7 pagesJamal 2014Andi EsSeNo ratings yet
- Park Et Al 2023 A Two Step Real Time PCR Method To Identify Mycobacterium Tuberculosis Infections and Six DominantDocument9 pagesPark Et Al 2023 A Two Step Real Time PCR Method To Identify Mycobacterium Tuberculosis Infections and Six DominantANS TOKANNo ratings yet
- 1 s2.0 S0732889323001359 MainDocument7 pages1 s2.0 S0732889323001359 MaindesaklaksmiNo ratings yet
- Mgen 000087Document10 pagesMgen 000087Bozner Sanchez EscobarNo ratings yet
- Genotypic Characterization of Mycobacterium Tuberculosis Strains Resistant To Rifampicin Isoniazid and Second Line Antibiotics in ChadDocument14 pagesGenotypic Characterization of Mycobacterium Tuberculosis Strains Resistant To Rifampicin Isoniazid and Second Line Antibiotics in ChadAthenaeum Scientific PublishersNo ratings yet
- Comparative Performance of Microbiological Methods For The Detection of Tuberculous Meningitis Pathogens in Cerebrospinal FluidDocument7 pagesComparative Performance of Microbiological Methods For The Detection of Tuberculous Meningitis Pathogens in Cerebrospinal FluiddesaklaksmiNo ratings yet
- Recent Advances in Tuberculosis Diagnostic Techniques: Review ArticleDocument6 pagesRecent Advances in Tuberculosis Diagnostic Techniques: Review ArticleMustaqeem DawarNo ratings yet
- Comparison of Gene-Xpert and Line Probe Assay For Detection of Mycobacterium Tuberculosis and Rifampicin-Mono ResistanceDocument8 pagesComparison of Gene-Xpert and Line Probe Assay For Detection of Mycobacterium Tuberculosis and Rifampicin-Mono ResistanceFaradilla FirdausaNo ratings yet
- Civ 609Document17 pagesCiv 609Descargar scribdNo ratings yet
- Kenneth V.I. Rolston, Davood Yadegarynia, Dimitrios P. Kontoyiannis, Issam I. Raad, Dah H. HoDocument8 pagesKenneth V.I. Rolston, Davood Yadegarynia, Dimitrios P. Kontoyiannis, Issam I. Raad, Dah H. HoAnggy de RinconNo ratings yet
- Contamination Des PouletsDocument18 pagesContamination Des PouletsSomda K MariusNo ratings yet
- Molecular Analysis of Bacterial Contamination On Stethoscopes in An Intensive Care UnitDocument7 pagesMolecular Analysis of Bacterial Contamination On Stethoscopes in An Intensive Care UnitletuslearnNo ratings yet
- Device Independent, Real TimeidentificationofbacterialDocument6 pagesDevice Independent, Real TimeidentificationofbacterialHenny_OordNo ratings yet
- Ciaa 1611Document8 pagesCiaa 1611Silvia Rodriguez PitreNo ratings yet
- Application of Molecular Biology-Based MethodsDocument6 pagesApplication of Molecular Biology-Based MethodsSophie KimNo ratings yet
- MycoDocument10 pagesMycorajaniNo ratings yet
- Miotto. Interpreting Mutations and Phenotypic DR. ERJ 2019Document13 pagesMiotto. Interpreting Mutations and Phenotypic DR. ERJ 2019Vigilancia EpidemiologicaNo ratings yet
- Sensors and Actuators B 193 (2014) 715 - 722Document8 pagesSensors and Actuators B 193 (2014) 715 - 722wardaninurindahNo ratings yet
- Biologicals: Chantal Fournier-Wirth, Joliette CosteDocument5 pagesBiologicals: Chantal Fournier-Wirth, Joliette CostevictoriaNo ratings yet
- IrfanDocument1 pageIrfanIrfan SonuNo ratings yet
- BMC Veterinary Research: Rapid Detection of Mycobacterium Bovis DNA in Cattle Lymph Nodes With Visible Lesions Using PCRDocument11 pagesBMC Veterinary Research: Rapid Detection of Mycobacterium Bovis DNA in Cattle Lymph Nodes With Visible Lesions Using PCRMayra FazNo ratings yet
- 2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)Document6 pages2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)SERGIO LOBATO FRANÇANo ratings yet
- Xpert MTB RIF Ultra For The Diagnosis of HIV-associated Tuberculous Meningitis - A Prospective Validation StudyDocument10 pagesXpert MTB RIF Ultra For The Diagnosis of HIV-associated Tuberculous Meningitis - A Prospective Validation StudyJorge AlvarezNo ratings yet
- Bacterial Meningitis in Children Under 15 Years of Age in NepalDocument7 pagesBacterial Meningitis in Children Under 15 Years of Age in NepalPrima YosiNo ratings yet
- Walter Et Al 2024 Performance Evaluation of Machine Assisted Interpretation of Gram Stains From Positive Blood CulturesDocument14 pagesWalter Et Al 2024 Performance Evaluation of Machine Assisted Interpretation of Gram Stains From Positive Blood Culturessazzad suvroNo ratings yet
- Klebsiella Pneumoniae Isolated From Urine ofDocument9 pagesKlebsiella Pneumoniae Isolated From Urine ofInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Thannesberger 2017Document15 pagesThannesberger 2017Денис КрахоткинNo ratings yet
- Schell 2012Document9 pagesSchell 2012PUPUT PUJIANTINo ratings yet
- Perspectives On Advances in Tuberculosis Diagnostics, Drugs, and VaccinesDocument17 pagesPerspectives On Advances in Tuberculosis Diagnostics, Drugs, and Vaccinesyenny handayani sihiteNo ratings yet
- Diagnosis of Lymph Node Tuberculosis Using The GeneXpert MTB:RIF in BangladeshDocument5 pagesDiagnosis of Lymph Node Tuberculosis Using The GeneXpert MTB:RIF in BangladeshReal CaaNo ratings yet
- Genexpert - On Body Fluid SpecimensDocument4 pagesGenexpert - On Body Fluid Specimensramo G.No ratings yet
- 2021 Genome-Wide Association Study of Resistance To MTBDocument18 pages2021 Genome-Wide Association Study of Resistance To MTBAntonio Jafar GarciaNo ratings yet
- Extrapulmonary Tuberculosis Comparative Analysis of Diagnostic Modalities Used in A Tertiary Healthcare SettingDocument2 pagesExtrapulmonary Tuberculosis Comparative Analysis of Diagnostic Modalities Used in A Tertiary Healthcare SettingBIOMEDSCIDIRECT PUBLICATIONSNo ratings yet
- Journal Homepage: - : IntroductionDocument7 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Microfluidics for Rapid Detection of Live PathogensDocument17 pagesMicrofluidics for Rapid Detection of Live Pathogensmicrobehunter007No ratings yet
- VERMA, Detection of M. Tuberculosis in The EnvironmentDocument9 pagesVERMA, Detection of M. Tuberculosis in The EnvironmentRafaele Carla Pivetta De AraujoNo ratings yet
- Whole Genome Sequencing Reveals High-Resolution Epidemiological Links Between Clinical and Environmental Klebsiella PneumoniaeDocument10 pagesWhole Genome Sequencing Reveals High-Resolution Epidemiological Links Between Clinical and Environmental Klebsiella PneumoniaeNora LeeNo ratings yet
- A Novel DNA Microarray For Rapid Diagnosis of Enteropathogenic Bacteria in Stool Specimens of Patients With DiarrheaDocument6 pagesA Novel DNA Microarray For Rapid Diagnosis of Enteropathogenic Bacteria in Stool Specimens of Patients With DiarrheaPritha BhuwapaksophonNo ratings yet
- Diagnosing Sepsis: Where We're at and Where We're Going: EditorialDocument3 pagesDiagnosing Sepsis: Where We're at and Where We're Going: EditorialCristina LopezNo ratings yet
- mgNGS_clinmicrob_watts2020Document7 pagesmgNGS_clinmicrob_watts2020Krisztián TóthNo ratings yet
- International Journal of Infectious DiseasesDocument7 pagesInternational Journal of Infectious DiseasesWINY LESLI ALFONSO BAUTISTANo ratings yet
- Antibiogram of Gram Negative Uropathogens in A TerDocument5 pagesAntibiogram of Gram Negative Uropathogens in A TerDumitraNo ratings yet
- Research On Pathogenic Bacteria and Antibiotic Resistance of Enterobacteriaceae in Hospitalized Elderly PatientsDocument5 pagesResearch On Pathogenic Bacteria and Antibiotic Resistance of Enterobacteriaceae in Hospitalized Elderly PatientsVishwas gargNo ratings yet
- 1 s2.0 S1472979217300252 MainDocument7 pages1 s2.0 S1472979217300252 MainpelleNo ratings yet
- Gut Microbiome Dynamics Over A Course of Kidney.273Document1 pageGut Microbiome Dynamics Over A Course of Kidney.273Liliana SiriteanuNo ratings yet
- Detection of Second-Line Drug Resistance in Mycobacterium Tuberculosis Using Oligonucleotide MicroarraysDocument8 pagesDetection of Second-Line Drug Resistance in Mycobacterium Tuberculosis Using Oligonucleotide MicroarrayscyclonzNo ratings yet
- Minimal Residual Disease Testing: Current Innovations and Future DirectionsFrom EverandMinimal Residual Disease Testing: Current Innovations and Future DirectionsTodd E. DruleyNo ratings yet
- 1 s2.0 S1658361222001251 MainDocument11 pages1 s2.0 S1658361222001251 MainaminNo ratings yet
- Relevance of Menarche, Menopause, and Other Bioevent To FertilityDocument3 pagesRelevance of Menarche, Menopause, and Other Bioevent To FertilitydattaniranjanNo ratings yet
- Pex 08 01Document4 pagesPex 08 01Rafi SalimNo ratings yet
- Community and Environmental HealthDocument26 pagesCommunity and Environmental HealthMary Grace AgueteNo ratings yet
- Zoology Sem-III & IV (New) 2019Document30 pagesZoology Sem-III & IV (New) 2019Ajay MeghanathiNo ratings yet
- Insectopia CompendiumDocument53 pagesInsectopia Compendiumnaruto hyuga67% (3)
- Instruction Manual: Direct-Zol - 96 Magbead RnaDocument8 pagesInstruction Manual: Direct-Zol - 96 Magbead RnaVIRAL WORLD IDNo ratings yet
- Blank2021 Article MarkerAllergensInHymenopteraVeDocument13 pagesBlank2021 Article MarkerAllergensInHymenopteraVeAna-Maria DuMiNo ratings yet
- PMR Examination 2004-2008Document9 pagesPMR Examination 2004-2008chlkhgNo ratings yet
- Human Development and LearningDocument36 pagesHuman Development and LearningBahasa KuNo ratings yet
- MLS3174 Clinical Haematology FEB 18 PDFDocument9 pagesMLS3174 Clinical Haematology FEB 18 PDFVisaNathanNo ratings yet
- Model Project Proposal (ITTO)Document22 pagesModel Project Proposal (ITTO)Bhaskar PaulNo ratings yet
- H3C - Abstract Book 12302014-V2Document204 pagesH3C - Abstract Book 12302014-V2AAPI ConventionNo ratings yet
- A Self-Assembled Nanoscale Robotic Arm Controlled by Electric FieldsDocument6 pagesA Self-Assembled Nanoscale Robotic Arm Controlled by Electric FieldsRegiane FerreiraNo ratings yet
- P5P6Sci - Respiratory SystemDocument8 pagesP5P6Sci - Respiratory SystemLevyNo ratings yet
- HomeostasisDocument3 pagesHomeostasisAffie SaikolNo ratings yet
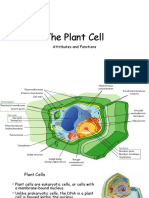
- The Plant CellDocument30 pagesThe Plant CellMichael GentilesNo ratings yet
- B 10 VRV 2042Document36 pagesB 10 VRV 2042api-283593849No ratings yet
- 1647-Article Text-3369-1-10-20220320Document5 pages1647-Article Text-3369-1-10-20220320Eshan BhaleraoNo ratings yet
- ID Identifikasi Jenis Alga Koralin Di PulauDocument4 pagesID Identifikasi Jenis Alga Koralin Di PulauEndoIeNo ratings yet
- Food Chemistry: SciencedirectDocument11 pagesFood Chemistry: Sciencedirectratri nurNo ratings yet
- Types of Leukocytes and The PlateletsDocument25 pagesTypes of Leukocytes and The PlateletscarcuevajailamarieNo ratings yet
- Ecozone Dichotomous KeyDocument3 pagesEcozone Dichotomous Keyqmtkqz72vhNo ratings yet
- Free Download Human Aging Calogero Caruso Full Chapter PDFDocument51 pagesFree Download Human Aging Calogero Caruso Full Chapter PDFnola.rodriguez670100% (20)
- Preprints202304 1223 v1Document23 pagesPreprints202304 1223 v1SrinivasaYadavNo ratings yet
- 2014 MBAA Chris White Yeast ManagementDocument30 pages2014 MBAA Chris White Yeast ManagementAdrián LampazziNo ratings yet
- Stainning 2019Document29 pagesStainning 2019Almoatazbellah AbdallahNo ratings yet