Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5824)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Mom Plan - Postpartum Fitness PlanDocument71 pagesMom Plan - Postpartum Fitness Plananon_809193911100% (2)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Employee Benefits Manual - Air India Express GMC 2023-24Document29 pagesEmployee Benefits Manual - Air India Express GMC 2023-24tanyaqthomasNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- MLHP LogBook PDFDocument471 pagesMLHP LogBook PDFMRS CHAKRAPANI92% (13)
- Stages of Labor FlowchartDocument1 pageStages of Labor FlowchartXyrelle GambalozaNo ratings yet
- Learning Objectives of MidwiferyDocument2 pagesLearning Objectives of Midwiferyangel panchal100% (2)
- Clinical InstructorDocument6 pagesClinical InstructorRae Dominick Aquino SalvaNo ratings yet
- INTRODUCTIONDocument3 pagesINTRODUCTIONRae Dominick Aquino SalvaNo ratings yet
- CDX Oral RevalidaDocument9 pagesCDX Oral RevalidaRae Dominick Aquino SalvaNo ratings yet
- Salva, Rae Dominick A. NSTP ActivityDocument3 pagesSalva, Rae Dominick A. NSTP ActivityRae Dominick Aquino SalvaNo ratings yet
- Total Population Number of Households A. Family Members and CharacteristicsDocument19 pagesTotal Population Number of Households A. Family Members and CharacteristicsRae Dominick Aquino SalvaNo ratings yet
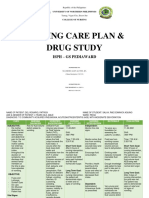
- Salva, R.D NCP & Drug Study (Isph - Gs Pediaward)Document7 pagesSalva, R.D NCP & Drug Study (Isph - Gs Pediaward)Rae Dominick Aquino SalvaNo ratings yet
- The Child Health Programs Newborns InfantsDocument78 pagesThe Child Health Programs Newborns InfantsRae Dominick Aquino SalvaNo ratings yet
- Overall TallyDocument12 pagesOverall TallyRae Dominick Aquino SalvaNo ratings yet
- What Does It Mean To Be A Citizen of The World?: Reflection PaperDocument1 pageWhat Does It Mean To Be A Citizen of The World?: Reflection PaperRae Dominick Aquino SalvaNo ratings yet
- Chapter 9 Global CitizenshipDocument2 pagesChapter 9 Global CitizenshipRae Dominick Aquino SalvaNo ratings yet
- Kwashiorkor-Is A Form of Severe ProteinDocument20 pagesKwashiorkor-Is A Form of Severe ProteinRae Dominick Aquino SalvaNo ratings yet
- By Julie May MolinaDocument12 pagesBy Julie May MolinaRae Dominick Aquino SalvaNo ratings yet
- University of Northern PhilippinesDocument11 pagesUniversity of Northern PhilippinesRae Dominick Aquino SalvaNo ratings yet
- Daily Checklist: University of Northern PhilippinesDocument2 pagesDaily Checklist: University of Northern PhilippinesRae Dominick Aquino SalvaNo ratings yet
- Final Exam MMWDocument6 pagesFinal Exam MMWRae Dominick Aquino SalvaNo ratings yet
- Daily Checklist: Did You... Mo N Tu e We D TH U FR I Sa T Su NDocument4 pagesDaily Checklist: Did You... Mo N Tu e We D TH U FR I Sa T Su NRae Dominick Aquino SalvaNo ratings yet
- Care Plan Group 4Document5 pagesCare Plan Group 4Rae Dominick Aquino SalvaNo ratings yet
- .O ....... OU :2l2 - : Office of The SecretaryDocument7 pages.O ....... OU :2l2 - : Office of The SecretarysabrinajavellanaNo ratings yet
- MCN LEC Quizzes - (2mid) (A-Prelims)Document43 pagesMCN LEC Quizzes - (2mid) (A-Prelims)Aaron Jane GalangNo ratings yet
- 7 Postpartum CareDocument20 pages7 Postpartum CareVirgie GigiNo ratings yet
- Postpartum NCPDocument20 pagesPostpartum NCPapi-370148988% (34)
- Joy Wanjiru Midwifery Case StudyDocument34 pagesJoy Wanjiru Midwifery Case StudyJimmy Maina100% (1)
- BPT3 RD YearDocument17 pagesBPT3 RD YearKhushNo ratings yet
- NCP No. 1 (Postpartum Duty)Document2 pagesNCP No. 1 (Postpartum Duty)Chrizley Shawn DeroniaNo ratings yet
- Rooming in ActDocument5 pagesRooming in ActShaira EddingNo ratings yet
- Evaluation of Factors That Contributes To Post-Partum Haemorrhage in Pregnant Women at KIU-THDocument14 pagesEvaluation of Factors That Contributes To Post-Partum Haemorrhage in Pregnant Women at KIU-THKIU PUBLICATION AND EXTENSIONNo ratings yet
- Postnatal ExaminationDocument19 pagesPostnatal ExaminationAlpha100% (1)
- 03 A025 5123Document13 pages03 A025 5123Sri HariNo ratings yet
- Postnatal Care PlanDocument20 pagesPostnatal Care Planjinsi georgeNo ratings yet
- SCRIPT For SOCLEGDocument7 pagesSCRIPT For SOCLEGKaren Ryl Lozada BritoNo ratings yet
- Factors That Can Influence The Counselling Session - Counselling For Maternal and Newborn Health Care - Ncbi BookshelfDocument15 pagesFactors That Can Influence The Counselling Session - Counselling For Maternal and Newborn Health Care - Ncbi BookshelfNur Ain KhadirNo ratings yet
- Lesson 6 11midtermDocument28 pagesLesson 6 11midtermREIMOND VINCE MENDOZANo ratings yet
- Mizoram Nursing Council: Part I: Objectives Answer All QuestionsDocument3 pagesMizoram Nursing Council: Part I: Objectives Answer All QuestionsAmy LalringhluaniNo ratings yet
- 0nursing Culture Chapter 05 1 1Document24 pages0nursing Culture Chapter 05 1 1Earlou MagbanuaNo ratings yet
- Breast Feeding Problems in Primipara Mothers in Early Postnatal Period Bushra Najem Lamia Dhia Al-DeenDocument4 pagesBreast Feeding Problems in Primipara Mothers in Early Postnatal Period Bushra Najem Lamia Dhia Al-DeenEstellaNo ratings yet
- Kehamilan Persalinan NifasDocument29 pagesKehamilan Persalinan NifaschoiimmaNo ratings yet
- Beliefs and Practises Surrounding Postpartum Period Among Malay WomenDocument9 pagesBeliefs and Practises Surrounding Postpartum Period Among Malay WomenBrillo Virla DawnNo ratings yet
- Group 3 and 4 MCN UpdatesDocument11 pagesGroup 3 and 4 MCN UpdatesDance TagleNo ratings yet
- NCM 107 Maternal and Child Nursing Related Learning Experience BSN 2 AY 2020-2021Document18 pagesNCM 107 Maternal and Child Nursing Related Learning Experience BSN 2 AY 2020-2021janina myka100% (1)
- Lochia Patterns Among Normal Women: A Systematic ReviewDocument5 pagesLochia Patterns Among Normal Women: A Systematic Reviewasm obginNo ratings yet
- Primigravida Mothers Knowledge-2128Document15 pagesPrimigravida Mothers Knowledge-2128Mariecor EnriquezNo ratings yet
- Virtual Field Work ReportDocument29 pagesVirtual Field Work ReportFarah FaadhilaNo ratings yet