Download as pdf or txt
You might also like
- (Book 1) : Career Paths: Physiotherapy - GlossaryDocument15 pages(Book 1) : Career Paths: Physiotherapy - Glossarygab77No ratings yet
- 1.3.8.8. Action-Reflection-Action-Session-ARAS (BSN2H)Document1 page1.3.8.8. Action-Reflection-Action-Session-ARAS (BSN2H)Kristil ChavezNo ratings yet
- Learn The Anatomy of The HeartDocument3 pagesLearn The Anatomy of The Heartash vldnbr100% (1)
- Transferring, Logrolling and PositioningDocument89 pagesTransferring, Logrolling and PositioningJay Vincent MedranoNo ratings yet
- Providing Range of Motion ExercisesDocument5 pagesProviding Range of Motion ExercisesKristine Faith AzcuetaNo ratings yet
- Active and Passive Exercise 1Document52 pagesActive and Passive Exercise 1Khairul Hanan100% (5)
- Range of Motion Procedure Checklist-1Document2 pagesRange of Motion Procedure Checklist-1api-288919673100% (2)
- Body Mechanics and Transferring PatientDocument57 pagesBody Mechanics and Transferring PatientRhenier S. Ilado100% (2)
- Assist With Client or Patient MovementDocument88 pagesAssist With Client or Patient Movementmihret gashayeNo ratings yet
- Range of MotionDocument5 pagesRange of MotionLevy DuranNo ratings yet
- 15 Providing Passive Range of Motion ExerciseDocument7 pages15 Providing Passive Range of Motion ExerciseFreisan ChenNo ratings yet
- Range of MotionDocument17 pagesRange of MotionJim Cariaga100% (2)
- Principles of Body Mechanics:: Rom& Isometric ExercisesDocument5 pagesPrinciples of Body Mechanics:: Rom& Isometric ExercisesRose Antonette BenitoNo ratings yet
- Shoulder Range of Motion Exercises PDFDocument4 pagesShoulder Range of Motion Exercises PDFGade JyNo ratings yet
- Techniques of Body MechanicsDocument11 pagesTechniques of Body MechanicsJazelyn Mae UyNo ratings yet
- Body MechanicsDocument41 pagesBody MechanicsPaul ReynaldoNo ratings yet
- Body Mechanics and Transfer TechniquesDocument90 pagesBody Mechanics and Transfer TechniquesTina Talmadge100% (1)
- Performance Checklist - ROMDocument3 pagesPerformance Checklist - ROMCrishaGarraNo ratings yet
- Rom Exercise 2Document7 pagesRom Exercise 2KBDNo ratings yet
- Activities of Daily Living Assignment Hcap 1000Document5 pagesActivities of Daily Living Assignment Hcap 1000184448No ratings yet
- Passive Mobilization Exercises Upper LimbDocument3 pagesPassive Mobilization Exercises Upper LimbAnujGuptaNo ratings yet
- Range of MotionDocument23 pagesRange of MotionSulton IlhamNo ratings yet
- Proc RangeOfMotionDocument4 pagesProc RangeOfMotionSri KuspartianingsihNo ratings yet
- Muscular - Active Assistive Range of Motion (AAROM)Document4 pagesMuscular - Active Assistive Range of Motion (AAROM)mksayshiNo ratings yet
- Skills 116 Finals ROM Assistive Devices PDFDocument64 pagesSkills 116 Finals ROM Assistive Devices PDFMae Arra Gilbao Lecobu-anNo ratings yet
- Week 4 Prelab Homework - AnswersDocument12 pagesWeek 4 Prelab Homework - AnswerswilliamsdevanelNo ratings yet
- Screenshot 2023-04-12 at 8.31.24 PM PDFDocument6 pagesScreenshot 2023-04-12 at 8.31.24 PM PDFAkku AkkuNo ratings yet
- Ballistic StretchingDocument17 pagesBallistic StretchingDayana AriqaNo ratings yet
- Lesson Notes - Body MechanicsDocument9 pagesLesson Notes - Body MechanicsNicole Marin-ChingNo ratings yet
- Principles of Body Mechanics: By: Angeluz Fernandez-GarciaDocument34 pagesPrinciples of Body Mechanics: By: Angeluz Fernandez-Garciadear_angel2003No ratings yet
- Body MechanicsDocument27 pagesBody MechanicsJURY LEIGH SALUQUENNo ratings yet
- Total Hip Replacement Home ProgramDocument5 pagesTotal Hip Replacement Home ProgramBhargav DaveNo ratings yet
- ROM1Document4 pagesROM1Nishan DuwalNo ratings yet
- Body Mec and Bed MakingDocument95 pagesBody Mec and Bed Makingloise100% (1)
- Transfer and AmbulationDocument108 pagesTransfer and AmbulationGladys YaresNo ratings yet
- Nightingale PledgeDocument7 pagesNightingale PledgeRacquel RomanoNo ratings yet
- Revised Moving Lifting ProcedureDocument8 pagesRevised Moving Lifting ProcedureBritthaney BuladacoNo ratings yet
- Bahasa Inggris Kelompok 4Document11 pagesBahasa Inggris Kelompok 4Elsya FaradimaNo ratings yet
- Pe 2Document21 pagesPe 2Glaiza RontasNo ratings yet
- Nursing Funda Manual NewDocument420 pagesNursing Funda Manual Newharold smithNo ratings yet
- Body Mechanics: Ms. Francisca Achaliwie AND Ms. Mabel Apaanye AvaneDocument22 pagesBody Mechanics: Ms. Francisca Achaliwie AND Ms. Mabel Apaanye AvaneAmfo Baffoe FrederickNo ratings yet
- A R-ExerciseDocument7 pagesA R-ExerciseElisha RamsayNo ratings yet
- Total-Shoulder ExercicesDocument9 pagesTotal-Shoulder ExercicesAmalia MihaiNo ratings yet
- Body MechanicsDocument24 pagesBody MechanicsKevin Matthew O. Velasco50% (2)
- Moving & TurningDocument15 pagesMoving & TurningNoel AyalaNo ratings yet
- Body MechanicsDocument5 pagesBody MechanicsAnnapurna Dangeti100% (1)
- THR RestrictedDocument25 pagesTHR RestrictedYadareli DothéNo ratings yet
- TKR ProtocolDocument8 pagesTKR ProtocolSandeep SoniNo ratings yet
- Self StretchDocument4 pagesSelf StretchHiba RiazNo ratings yet
- P.E 2 MidtermDocument36 pagesP.E 2 Midtermlazarozijan04No ratings yet
- Proper Body MechanicsDocument3 pagesProper Body MechanicsAbriann Vince ImpenioNo ratings yet
- Range of Motion Exercises: in HealthDocument8 pagesRange of Motion Exercises: in HealthCagabcab Canibel Melany100% (1)
- Functional Foundations by SET FOR SETDocument36 pagesFunctional Foundations by SET FOR SETdinos99hotmail.comNo ratings yet
- Stretching Fundamentals11Document29 pagesStretching Fundamentals11April Ann HortilanoNo ratings yet
- Chapter 1 Body Mechanics: DefinitionDocument25 pagesChapter 1 Body Mechanics: DefinitionCyeonjNo ratings yet
- Cervical Arthrodesis: PT Preoperative and Postoperative ManagementDocument3 pagesCervical Arthrodesis: PT Preoperative and Postoperative ManagementJoanna EdenNo ratings yet
- 7-BobathDocument9 pages7-BobathAmany SaifNo ratings yet
- Mobility - RIOSDocument122 pagesMobility - RIOSangemcpo08No ratings yet
- Body Conditioning: Physical ActivityDocument18 pagesBody Conditioning: Physical ActivityArdiene Shallouvette Gamoso100% (1)
- Range of MotionDocument5 pagesRange of MotionUmmu NafilaNo ratings yet
- Body MechanicsDocument87 pagesBody MechanicsShazneiy KhanNo ratings yet
- Active Assisted ExerciseDocument25 pagesActive Assisted ExerciseMuhammad Gustrin SyahNo ratings yet
- Presenting Complaints (As Applicable)Document2 pagesPresenting Complaints (As Applicable)Kristil ChavezNo ratings yet
- Case PresDocument2 pagesCase PresKristil ChavezNo ratings yet
- Gerd HTP Bn3aDocument4 pagesGerd HTP Bn3aKristil ChavezNo ratings yet
- Calendula (Pot Marigolds) : Kristil Marie E. Chavez BN3ADocument1 pageCalendula (Pot Marigolds) : Kristil Marie E. Chavez BN3AKristil ChavezNo ratings yet
- Addison DiseaseDocument22 pagesAddison DiseaseKristil ChavezNo ratings yet
- Assessment Cues Nursing Diagnosis Desired Outcome Nursing Intervention Justification EvaluationDocument3 pagesAssessment Cues Nursing Diagnosis Desired Outcome Nursing Intervention Justification EvaluationKristil ChavezNo ratings yet
- ReflectionDocument3 pagesReflectionKristil ChavezNo ratings yet
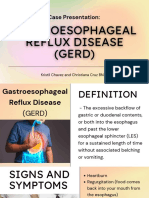
- Case Presentation:: Kristil Chavez and Christiana Cruz BN3ADocument21 pagesCase Presentation:: Kristil Chavez and Christiana Cruz BN3AKristil ChavezNo ratings yet
- UntitledDocument2 pagesUntitledKristil ChavezNo ratings yet
- Intravenous/Parenteral Fluid Sheet: 01/31/2023 4:00pm 2 Pnss KMCDocument1 pageIntravenous/Parenteral Fluid Sheet: 01/31/2023 4:00pm 2 Pnss KMCKristil ChavezNo ratings yet
- Medication Sheet: Complete Name and Initials of Medication NurseDocument1 pageMedication Sheet: Complete Name and Initials of Medication NurseKristil ChavezNo ratings yet
- ARNISDocument16 pagesARNISKristil ChavezNo ratings yet
- Draftt News ArticleeeeDocument1 pageDraftt News ArticleeeeKristil ChavezNo ratings yet
- Barangay Health Center Services and DOH ProgramsDocument7 pagesBarangay Health Center Services and DOH ProgramsKristil Chavez100% (1)
- TPR-Sheet-MW2-Case 1Document2 pagesTPR-Sheet-MW2-Case 1Kristil ChavezNo ratings yet
- Drug Study-MW2-Case 1Document4 pagesDrug Study-MW2-Case 1Kristil ChavezNo ratings yet
- Nurse's Notes-MW2-Case 1Document1 pageNurse's Notes-MW2-Case 1Kristil ChavezNo ratings yet
- PCOM Reaction Paper (Chavez BSN1a)Document1 pagePCOM Reaction Paper (Chavez BSN1a)Kristil ChavezNo ratings yet
- Health EducationDocument17 pagesHealth EducationKristil ChavezNo ratings yet
- Otorhinolaryngology: Inferior Turbinectomy: What Is The Best Technique?Document2 pagesOtorhinolaryngology: Inferior Turbinectomy: What Is The Best Technique?Ramya KamathNo ratings yet
- 6 Exercises For Diastasis Recti Say Goodbye To The Mommy TummyDocument9 pages6 Exercises For Diastasis Recti Say Goodbye To The Mommy TummyLinda Pride100% (3)
- Second Summative TestDocument3 pagesSecond Summative TestHoney Laluna Cimeni100% (1)
- Accessory LigamentsDocument10 pagesAccessory LigamentsWidy AnniNo ratings yet
- Workbook ActivityDocument2 pagesWorkbook ActivityRisciella 18No ratings yet
- Airway ManagementDocument129 pagesAirway ManagementSyabie YassinNo ratings yet
- Shoulder Marma Point PDFDocument3 pagesShoulder Marma Point PDFSatyam PatelNo ratings yet
- INTOEINGDocument1 pageINTOEINGJoanne AngelicaNo ratings yet
- Tounge Thrust SwallowingDocument2 pagesTounge Thrust SwallowinglexerdowsalternativeNo ratings yet
- Rehabilitation of Tibial Plateau FractureDocument29 pagesRehabilitation of Tibial Plateau FractureJansen LeeNo ratings yet
- Equine Veterinary - Circulatory System - Horse First AiDocument1 pageEquine Veterinary - Circulatory System - Horse First AiRenan RodriguesNo ratings yet
- Interpreting The Chest Radio Graph Friendly)Document9 pagesInterpreting The Chest Radio Graph Friendly)Vagner BorgesNo ratings yet
- SHS The HUMAN BODY An OrientationDocument81 pagesSHS The HUMAN BODY An OrientationRhena TogoresNo ratings yet
- Sistem Saraf OtonomDocument55 pagesSistem Saraf OtonomElizar JarNo ratings yet
- Thoracic Segment KpsDocument77 pagesThoracic Segment Kpskrishna bptNo ratings yet
- Marieb pg446Document1 pageMarieb pg446Kai Joseph JaradatNo ratings yet
- ASDA Packet I-K (Part 1)Document48 pagesASDA Packet I-K (Part 1)Kelly KouchNo ratings yet
- The Miracle Seven: Tiger Move ExercisesDocument9 pagesThe Miracle Seven: Tiger Move ExercisesPete PuzaNo ratings yet
- CBSE Class 11 Biology Chapter 21 Neural Control and Coordination NotesDocument7 pagesCBSE Class 11 Biology Chapter 21 Neural Control and Coordination NotesShivalgiri Goswami0% (1)
- Angiology: Sanqiang Pan Department of Anatomy Medical College of Jinan UniversityDocument34 pagesAngiology: Sanqiang Pan Department of Anatomy Medical College of Jinan UniversityKw ChanNo ratings yet
- Dr. Mike Israetel Training Volume Landmarks Hypertrophy RoutineDocument25 pagesDr. Mike Israetel Training Volume Landmarks Hypertrophy RoutineBen ChadneyNo ratings yet
- Pilates and The Powerhouse II PDFDocument9 pagesPilates and The Powerhouse II PDFviboramorNo ratings yet
- Chapter 7 Muscles Power PointDocument102 pagesChapter 7 Muscles Power PointNurseReyesNo ratings yet
- Ankle X-Ray InterpretationDocument9 pagesAnkle X-Ray InterpretationBeeNo ratings yet
- Fitness Block PlanDocument10 pagesFitness Block PlanSteven GallagherNo ratings yet
- Jimed, Vol. 3, No. 2 Issn 2356-301XDocument5 pagesJimed, Vol. 3, No. 2 Issn 2356-301XDewi YulyantiNo ratings yet
- Hyperemia and Congestion Pathology NotesDocument4 pagesHyperemia and Congestion Pathology NotesMinto George100% (1)
- Sistem Urinarius, Pelvis & Perineum: DR - Tri Suciati, M.KesDocument96 pagesSistem Urinarius, Pelvis & Perineum: DR - Tri Suciati, M.KeslianaalviahNo ratings yet