Download as pdf or txt
You might also like
- 2dennis - M - Marchiori Clinical ImagingDocument1,481 pages2dennis - M - Marchiori Clinical Imagingsimona mariana dutuNo ratings yet
- Honda PresentationDocument39 pagesHonda PresentationAkkhi_D_Chaser_6797100% (1)
- WiFi Function Manual of Charge Point-181030 PDFDocument16 pagesWiFi Function Manual of Charge Point-181030 PDFfreesonNo ratings yet
- SITXFSA001 - Student AssessmentDocument31 pagesSITXFSA001 - Student AssessmentNiroj Adhikari100% (3)
- 31.05.23 AdrenalDocument46 pages31.05.23 AdrenallilydariniNo ratings yet
- Cushing Disease (By Syukri)Document3 pagesCushing Disease (By Syukri)Ebrahim Adel Ali AhmedNo ratings yet
- Adrenal MassDocument38 pagesAdrenal Massshaza ewisNo ratings yet
- Adrenal Gland 3: Dr. Hani Rjoob Dr. Rami AlayasaDocument34 pagesAdrenal Gland 3: Dr. Hani Rjoob Dr. Rami AlayasaMahmoud Abu MayalehNo ratings yet
- Addison+conn+cush+feo+adr IncidentalomaDocument65 pagesAddison+conn+cush+feo+adr IncidentalomaMjn BausatNo ratings yet
- Hipotalamus-Pituitari-Sumbu Adrenal (Axis) Regulasi Sirkadian Korteks Adrenal CRH ACTHDocument9 pagesHipotalamus-Pituitari-Sumbu Adrenal (Axis) Regulasi Sirkadian Korteks Adrenal CRH ACTHAnastasia PinkyNo ratings yet
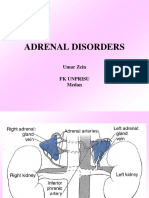
- Adrenal Disorders: Umar Zein FK Unprisu MedanDocument48 pagesAdrenal Disorders: Umar Zein FK Unprisu Medanyukmin rotamaNo ratings yet
- Cushing Syndrome in Children: Dr. Mahbuba Jahan Sharmin Dr. Ismat Jahan ShimiDocument57 pagesCushing Syndrome in Children: Dr. Mahbuba Jahan Sharmin Dr. Ismat Jahan Shimisheme1711No ratings yet
- Diseases of The Adrenal GlandsDocument27 pagesDiseases of The Adrenal GlandsPurnima ChoudhuryNo ratings yet
- Adrenal Disorders: Divisi Endokrin Dan Metabolik Bagian Penyakit Dalam FK USU RSUP H. Adam Malik MedanDocument45 pagesAdrenal Disorders: Divisi Endokrin Dan Metabolik Bagian Penyakit Dalam FK USU RSUP H. Adam Malik MedanSiddiq Blackhell CakepNo ratings yet
- Adrenal Disorders: Dr. Anil Dhakal Lecturer, Internal MedicineDocument53 pagesAdrenal Disorders: Dr. Anil Dhakal Lecturer, Internal MedicineBi PinNo ratings yet
- Adrenal ColorDocument35 pagesAdrenal ColorAnonymous oOofKbmPTiNo ratings yet
- AdrenalpathologyDocument81 pagesAdrenalpathologyjoavchNo ratings yet
- Adrenal Disease VTCDocument50 pagesAdrenal Disease VTCElena Borş Morari100% (1)
- Lec#17+18 Adrenal DisordersDocument101 pagesLec#17+18 Adrenal DisordersKhaldoun AlmomaniNo ratings yet
- Cushing's SyndromeDocument25 pagesCushing's SyndromeRose Ann Del MundoNo ratings yet
- Cushing's - Syndrome - Nov 2010Document35 pagesCushing's - Syndrome - Nov 2010Jim Jose AntonyNo ratings yet
- AdrenalDocument9 pagesAdrenalNada MuchNo ratings yet
- Adrenal Gland PathologyDocument6 pagesAdrenal Gland PathologyRami ShishanNo ratings yet
- EBM - 5. Adrenal DisordersDocument101 pagesEBM - 5. Adrenal DisordersBRI KUNo ratings yet
- Pathology of Adrenal Glands.Document41 pagesPathology of Adrenal Glands.Sukma Eka PratiwiNo ratings yet
- Endocrinology Part 1Document131 pagesEndocrinology Part 1LucjaNo ratings yet
- Adrenal Disorders in ChildrenDocument39 pagesAdrenal Disorders in ChildrenCorina OngNo ratings yet
- Adrenal Disorders in ChildrenDocument50 pagesAdrenal Disorders in ChildrenadinayNo ratings yet
- Adrenal Cortex and Medulla - The Clinical ContextDocument10 pagesAdrenal Cortex and Medulla - The Clinical ContextbluesaltNo ratings yet
- 5) Adrenal GlandDocument74 pages5) Adrenal GlandABUBEKER BESHIRNo ratings yet
- Anatomy & Physiology: CRH ActhDocument6 pagesAnatomy & Physiology: CRH ActhAmoroso, Marian Corneth D.No ratings yet
- Cushing SyndromeDocument12 pagesCushing SyndromeAmoroso, Marian Corneth D.No ratings yet
- Adrenal Glands: Dr. Wien Wiratmoko SppaDocument27 pagesAdrenal Glands: Dr. Wien Wiratmoko SppaYusha NugrahaNo ratings yet
- 6.23.08 Dancel Endocrine BD RevDocument32 pages6.23.08 Dancel Endocrine BD Revkhaled_71111No ratings yet
- Cushing 2020Document74 pagesCushing 2020FloreaAndreiNo ratings yet
- Cushing Syndrom - NisaDocument17 pagesCushing Syndrom - NisaSilvanaPutriNo ratings yet
- The Hypothalamo-Pituitary-Adrenocortical Axis: Dr. Noelle Orata Mount Kenya UniversityDocument49 pagesThe Hypothalamo-Pituitary-Adrenocortical Axis: Dr. Noelle Orata Mount Kenya UniversityvivianNo ratings yet
- Kuliah AdrenalDocument32 pagesKuliah AdrenalNindhyana Diwaratri R100% (1)
- Cushing's SyndromeDocument2 pagesCushing's SyndromeKuan NgNo ratings yet
- Cushing's SyndromeDocument2 pagesCushing's SyndromeKuan NgNo ratings yet
- Cushing's SyndromeDocument2 pagesCushing's SyndromeKuan NgNo ratings yet
- Cushing's SyndromeDocument2 pagesCushing's SyndromeKuan NgNo ratings yet
- Adrenocortical HyperfunctionDocument132 pagesAdrenocortical Hyperfunctionshobharamkrishna100% (2)
- Cushing Syndrome: M.Sc. (N) 1 YearDocument30 pagesCushing Syndrome: M.Sc. (N) 1 YearRanjana SharmaNo ratings yet
- 20) Dr. Dr. Himawan Sanusi, Sp. PD, KEMD - Cushing+conn+addsosnianDocument27 pages20) Dr. Dr. Himawan Sanusi, Sp. PD, KEMD - Cushing+conn+addsosnianAsridewi DewiNo ratings yet
- Adrenal DiseasesDocument35 pagesAdrenal Diseasesmy Lord JesusNo ratings yet
- Endo-2 Hyperprolactinemia DIDocument40 pagesEndo-2 Hyperprolactinemia DIalhusien.abd2000No ratings yet
- Adrenal DiseaseDocument77 pagesAdrenal DiseaseNzau Muange100% (1)
- EndocrinologyDocument10 pagesEndocrinology96k7z7khz7No ratings yet
- Adrenal Disease 1Document77 pagesAdrenal Disease 1Nzau MuangeNo ratings yet
- Disease of Adrenal GlandDocument47 pagesDisease of Adrenal GlandgibreilNo ratings yet
- Adrenal Glands Cushing's SyndromeDocument7 pagesAdrenal Glands Cushing's SyndromeSue SongNo ratings yet
- Adrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing SyndromeDocument46 pagesAdrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing Syndromeyuyu tuptupNo ratings yet
- 2.06.08 Cushing's Syndrome McClune - 2Document24 pages2.06.08 Cushing's Syndrome McClune - 2IkbarardianNo ratings yet
- Adrenal PathologyDocument63 pagesAdrenal PathologyHafizur RashidNo ratings yet
- Adrenal DisordersDocument48 pagesAdrenal DisordersMubeenUrRehmanNo ratings yet
- 005 - Cushing SyndromeDocument51 pages005 - Cushing SyndromeLucas Victor AlmeidaNo ratings yet
- Dr. Harsinen SubjectDocument222 pagesDr. Harsinen SubjectFaridah LailiNo ratings yet
- Adrenal Cortex: - Divided Into Three Zones - Zona Glomerulosa (Outer Layer) ProducesDocument25 pagesAdrenal Cortex: - Divided Into Three Zones - Zona Glomerulosa (Outer Layer) ProducesSaddamix AL OmariNo ratings yet
- Master The Wards - Internal Medicine - 1Document16 pagesMaster The Wards - Internal Medicine - 1rayousufNo ratings yet
- Chusing SyndromeDocument30 pagesChusing Syndromebagusputrabali13No ratings yet
- Addison's Disease-Dr. AM IyagbaDocument34 pagesAddison's Disease-Dr. AM IyagbaDr. Amb. Monday ZaccheausNo ratings yet
- Jacquier - CMR and MDCT in Cardiac MassesDocument162 pagesJacquier - CMR and MDCT in Cardiac Massessimona mariana dutuNo ratings yet
- Laboratory Procedures in HaematologyDocument104 pagesLaboratory Procedures in Haematologysimona mariana dutuNo ratings yet
- Diagnostic Imaging Pediatrics by Lane F. Donnelly, Blaise v. Jones, Sara M. OHara, Christopher G. Anton, Corning Benton, Sjirk J. Westra, Steven J. Kraus, Janet L. Strife, Bernadette L. Koch, Karin L.Document1,148 pagesDiagnostic Imaging Pediatrics by Lane F. Donnelly, Blaise v. Jones, Sara M. OHara, Christopher G. Anton, Corning Benton, Sjirk J. Westra, Steven J. Kraus, Janet L. Strife, Bernadette L. Koch, Karin L.simona mariana dutu100% (1)
- AKTOLUN - Nuclear OncologyDocument730 pagesAKTOLUN - Nuclear Oncologysimona mariana dutuNo ratings yet
- Bombardieri - Breast Cancer - Nuclear Medicine in Diagnosis and Therapeutic OptionsDocument309 pagesBombardieri - Breast Cancer - Nuclear Medicine in Diagnosis and Therapeutic Optionssimona mariana dutuNo ratings yet
- Pain Spine Disorders - MainDocument10 pagesPain Spine Disorders - Mainsimona mariana dutuNo ratings yet
- Spinal Stenosis-Lumbar: Douglas S. Fenton, M.DDocument10 pagesSpinal Stenosis-Lumbar: Douglas S. Fenton, M.Dsimona mariana dutuNo ratings yet
- Pain in The Spine DisorderDocument8 pagesPain in The Spine Disordersimona mariana dutuNo ratings yet
- Synovial Cyst: Leo F. Czervionke, M.DDocument8 pagesSynovial Cyst: Leo F. Czervionke, M.Dsimona mariana dutuNo ratings yet
- Comprehensive Manuals in Radiology: Harold G. Jacobson, EditorDocument140 pagesComprehensive Manuals in Radiology: Harold G. Jacobson, Editorsimona mariana dutuNo ratings yet
- Presentation 9Document1 pagePresentation 9simona mariana dutuNo ratings yet
- Ami 02Document39 pagesAmi 02simona mariana dutuNo ratings yet
- Basic Radiology PDFDocument104 pagesBasic Radiology PDFsimona mariana dutu100% (1)
- Nipple DischargeDocument16 pagesNipple Dischargesimona mariana dutuNo ratings yet
- The Foot: Obvious Look ForDocument13 pagesThe Foot: Obvious Look Forsimona mariana dutu100% (1)
- Hip FractureDocument14 pagesHip Fracturesimona mariana dutuNo ratings yet
- Module 3Document10 pagesModule 3Joseph JohnNo ratings yet
- ThesisDocument69 pagesThesisSyed Zaeem RizviNo ratings yet
- An LSTM Approach To Forecast Migration Using Google TrendsDocument8 pagesAn LSTM Approach To Forecast Migration Using Google TrendsSavantNo ratings yet
- GS 2646Document108 pagesGS 2646Wagner BernardinaNo ratings yet
- Translating Humor in Dubbing and SubtitlingDocument8 pagesTranslating Humor in Dubbing and SubtitlingJane Hartnett0% (1)
- Statement DEC PDFDocument14 pagesStatement DEC PDFUmay Delisha0% (1)
- China's Foreign Exchange Market AnalysisDocument27 pagesChina's Foreign Exchange Market AnalysisMilanNo ratings yet
- LPI - Company Profile - 2022Document4 pagesLPI - Company Profile - 2022Chrisneil DelosreyesNo ratings yet
- Grammaire - L1 G1+3+4+7 - M. Benkider - Corrigé Et CommentairesDocument3 pagesGrammaire - L1 G1+3+4+7 - M. Benkider - Corrigé Et CommentairesYssoufFahSNo ratings yet
- Textile Trade in BangladeshDocument5 pagesTextile Trade in BangladeshSanghamitra DasNo ratings yet
- Guided Exercise - Mendel's Peas: NameDocument9 pagesGuided Exercise - Mendel's Peas: NameStephanie Jane AndoyNo ratings yet
- KIK614441 IC Part1Document49 pagesKIK614441 IC Part1Hafid FajriNo ratings yet
- Blind Taste Test of Soft-Drinks - A Comparison Study On Coke and PepsiDocument4 pagesBlind Taste Test of Soft-Drinks - A Comparison Study On Coke and PepsiInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Gantry SystemDocument4 pagesGantry SystemTh NattapongNo ratings yet
- Cosmology GitaDocument122 pagesCosmology GitabaijumohanNo ratings yet
- DM Plan Golachipa Upazila Patuakhali District - English Version-2014Document110 pagesDM Plan Golachipa Upazila Patuakhali District - English Version-2014CDMP BangladeshNo ratings yet
- 0606 Additional Mathematics: MARK SCHEME For The October/November 2014 SeriesDocument6 pages0606 Additional Mathematics: MARK SCHEME For The October/November 2014 SeriesKennedy Absalom ModiseNo ratings yet
- Philosophies and Theories of EducationDocument26 pagesPhilosophies and Theories of Educationcynthiaaa sNo ratings yet
- 25 Common Surgical ConditionsDocument3 pages25 Common Surgical ConditionsMu AbNo ratings yet
- Summative Assessment RubricDocument2 pagesSummative Assessment Rubricapi-426187508No ratings yet
- Building Services Branch Testing and Commissioning ProcedureDocument211 pagesBuilding Services Branch Testing and Commissioning ProcedurePHYRAK100% (1)
- Product Data Sheet: Substation - S40 - Sepam Series 40Document2 pagesProduct Data Sheet: Substation - S40 - Sepam Series 40Arcvil AlzNo ratings yet
- Introduction To The Catering IndustryDocument33 pagesIntroduction To The Catering IndustrySandeep SinghNo ratings yet
- HSM 541 Week 7 Course ProjectDocument5 pagesHSM 541 Week 7 Course ProjecttheresajonesasNo ratings yet
- Unit IV IO NotesDocument15 pagesUnit IV IO NotesVarun VanaparthyNo ratings yet
- An Introduction To Eh AntennasDocument36 pagesAn Introduction To Eh AntennasYayok S. Anggoro100% (1)
- Chapter2 PDFDocument18 pagesChapter2 PDFshaik jaheerNo ratings yet