Download as pdf or txt
You might also like
- The ACM v2.0 International PDFDocument76 pagesThe ACM v2.0 International PDFTiago SilvaNo ratings yet
- Coronary Artery Bypass Graph Concept MapDocument5 pagesCoronary Artery Bypass Graph Concept Mapnursing concept maps100% (1)
- Pubs HPE OmniStack 4 1 3 For Vsphere Upgrade GuideDocument63 pagesPubs HPE OmniStack 4 1 3 For Vsphere Upgrade GuideYeraldo MarinNo ratings yet
- Guideline Title: Intra-Aortic Balloon Pump ManagementDocument16 pagesGuideline Title: Intra-Aortic Balloon Pump ManagementJansen ChNo ratings yet
- RFH COVID-19 ICU Resource Pack FULL PDFDocument15 pagesRFH COVID-19 ICU Resource Pack FULL PDFQuique GarciaNo ratings yet
- Hemorrhage ShockDocument17 pagesHemorrhage ShockgrizzlovNo ratings yet
- Handbook Conical MountingsDocument28 pagesHandbook Conical MountingsVito DigeoNo ratings yet
- The Occult Origins of The Bank of EnglandDocument7 pagesThe Occult Origins of The Bank of EnglandMarbleManNo ratings yet
- Ib Unit - The Arrival-Immigration-Visual ExperienceDocument6 pagesIb Unit - The Arrival-Immigration-Visual Experienceapi-284054906No ratings yet
- Cardiff Council Planning Committee Agenda For Wednesday February 13, 2013.Document222 pagesCardiff Council Planning Committee Agenda For Wednesday February 13, 2013.jessica_best2820No ratings yet
- Card ACLSDocument2 pagesCard ACLSSaman FirdousNo ratings yet
- Post Resuscitation Care: 15 SEPTEMBER 2014Document27 pagesPost Resuscitation Care: 15 SEPTEMBER 2014Arnold Daniel100% (1)
- Post Arrest CareDocument23 pagesPost Arrest CareMohamed RasoolNo ratings yet
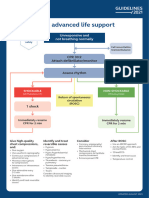
- Adult Advanced Life Support Algorithm 2021 Aug 2023Document1 pageAdult Advanced Life Support Algorithm 2021 Aug 2023cknihilnewNo ratings yet
- Post-Cardiac Arrest Care Algorithm: Return of Spontaneous Circulation (ROSC)Document1 pagePost-Cardiac Arrest Care Algorithm: Return of Spontaneous Circulation (ROSC)johndoe1995No ratings yet
- Pasca ResusitasiDocument2 pagesPasca Resusitasiolga adhityaNo ratings yet
- Adult Immediate Post Cardiac Arrest Care Algorithm 2015 UpdateDocument1 pageAdult Immediate Post Cardiac Arrest Care Algorithm 2015 UpdateRyggie Comelon0% (1)
- Critical Event Checklists PDFDocument27 pagesCritical Event Checklists PDFMateas ZsoltNo ratings yet
- 8-Adult Advanced Life Support Algorithm 2021Document1 page8-Adult Advanced Life Support Algorithm 2021khaledNo ratings yet
- Patient MonitoringDocument32 pagesPatient MonitoringhendranatjNo ratings yet
- Cardiac Arrest Circular Algorithm: Start CPR 2 M IN UT ESDocument1 pageCardiac Arrest Circular Algorithm: Start CPR 2 M IN UT ESjohndoe1995No ratings yet
- Weaning From Cardiopulmonary Bypass: Routine Cardiac SurgeryDocument5 pagesWeaning From Cardiopulmonary Bypass: Routine Cardiac SurgeryredaNo ratings yet
- 9 - Role of Non InvasiveDocument46 pages9 - Role of Non InvasiveHavara Kausar AkbarNo ratings yet
- PiCCO Technology Brochure PDFDocument32 pagesPiCCO Technology Brochure PDFHue PhamNo ratings yet
- ICU ManagementDocument26 pagesICU Managementvamshidh100% (2)
- Acute Medicine: Shock: Inadequate Tissue and Organ PerfusionDocument3 pagesAcute Medicine: Shock: Inadequate Tissue and Organ Perfusionmyat252No ratings yet
- Syok MurniDocument13 pagesSyok Murniolga adhityaNo ratings yet
- Society For Pediatric Anesthesia Emergency Checklist ManualDocument28 pagesSociety For Pediatric Anesthesia Emergency Checklist ManualJill SweetNo ratings yet
- Ischemic PreconditioningDocument36 pagesIschemic PreconditioninghirschmedNo ratings yet
- ACLS 2020 Algorithms: American Heart Association 2020 GuidelinesDocument8 pagesACLS 2020 Algorithms: American Heart Association 2020 GuidelinesNofi Nurina100% (4)
- Syok KardiogenikDocument31 pagesSyok KardiogenikcantikarevieraNo ratings yet
- 2009 PiCCO Advanced Hemodynamic Monitoring PDFDocument15 pages2009 PiCCO Advanced Hemodynamic Monitoring PDFYannis ZoldenbergNo ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityChris LeeNo ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityAlexis HospitalNo ratings yet
- Critical Event ChecklistsDocument25 pagesCritical Event ChecklistsarisyiNo ratings yet
- NCP CardioDocument10 pagesNCP CardioCharles LigonNo ratings yet
- Analisis Gas DarahDocument33 pagesAnalisis Gas DarahMerryNo ratings yet
- 8 - DR. Khaled - Cardiac SurgeryDocument26 pages8 - DR. Khaled - Cardiac SurgeryMuhand.No ratings yet
- RRT Care Plan Protocol GuideDocument4 pagesRRT Care Plan Protocol GuideTahani KhalilNo ratings yet
- Monitor Bedside BSM-3000 SeriesDocument8 pagesMonitor Bedside BSM-3000 SeriesDouglas Gaitan PotosmeNo ratings yet
- Bls and Acls: Deepika SelvaDocument82 pagesBls and Acls: Deepika SelvaPriyanka TNo ratings yet
- Cases in Surgical Critical CareDocument36 pagesCases in Surgical Critical CareHasan ShanawaniNo ratings yet
- Acls Notes 7-2012Document13 pagesAcls Notes 7-2012sarahbearcoupsNo ratings yet
- Algorithms - Paediatric Advanced Life Support PDFDocument1 pageAlgorithms - Paediatric Advanced Life Support PDFLenox BlackNo ratings yet
- Overview of Respiratory Failure & Use of Mechanical VentilationDocument89 pagesOverview of Respiratory Failure & Use of Mechanical VentilationsheharyarNo ratings yet
- Ventilator Management in Head Injury PatientssDocument28 pagesVentilator Management in Head Injury PatientssSivasubramanian BalasubramanianNo ratings yet
- AlgorithmACLS PCAC 200622Document1 pageAlgorithmACLS PCAC 200622Sandy XNo ratings yet
- ACLS Healthcare Provider Post-Cardiac Arrest Care Algorithm: o Co Io o CoDocument1 pageACLS Healthcare Provider Post-Cardiac Arrest Care Algorithm: o Co Io o CoAlexis HospitalNo ratings yet
- Note On Cardiopulmonary Physiotherapy PDFDocument16 pagesNote On Cardiopulmonary Physiotherapy PDFTsz Kwan CheungNo ratings yet
- CAA ECG Reporting SystemDocument16 pagesCAA ECG Reporting SystemLynne MannNo ratings yet
- Screenshot 2565-05-03 at 10.34.19Document39 pagesScreenshot 2565-05-03 at 10.34.19Sugus PichayaNo ratings yet
- Post Cardiac ArrestDocument2 pagesPost Cardiac ArrestAlthea AlcalaNo ratings yet
- Bedside Monitor: BSM-3000 SeriesDocument8 pagesBedside Monitor: BSM-3000 Seriesfarouk beNo ratings yet
- AnnCardAnaesth9144-7552051 020552Document5 pagesAnnCardAnaesth9144-7552051 020552Imanuel Far-FarNo ratings yet
- Adult Post-Cardiac Arrest Care Algorithm: o Co Io o CoDocument1 pageAdult Post-Cardiac Arrest Care Algorithm: o Co Io o CoKavya ShreeNo ratings yet
- Clinical Review - Update On Hemodynamic Monitoring - A Consensus of 16 - PMCDocument15 pagesClinical Review - Update On Hemodynamic Monitoring - A Consensus of 16 - PMCV ANo ratings yet
- C19 SPACE ToolKit ChecklistsDocument8 pagesC19 SPACE ToolKit ChecklistsAdrian BălanNo ratings yet
- Mindanao State University College of Health Sciences Marawi CityDocument17 pagesMindanao State University College of Health Sciences Marawi CityBella DonnaNo ratings yet
- ACLS Prof THDocument2 pagesACLS Prof THjwq6jxwy6tNo ratings yet
- Disturbances in AcidDocument11 pagesDisturbances in AcidShannen Alija M. LaoNo ratings yet
- Guidelines For The Management of Intracerebral HaemorrhageDocument18 pagesGuidelines For The Management of Intracerebral Haemorrhagerebeca marityNo ratings yet
- Chapter3Shock CirculationDocument13 pagesChapter3Shock CirculationSri AgustinaNo ratings yet
- Post Resus CareDocument35 pagesPost Resus Caredrjaikrish100% (1)
- Perfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationFrom EverandPerfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationRating: 5 out of 5 stars5/5 (2)
- Questions and Answers in Small Animal AnesthesiaFrom EverandQuestions and Answers in Small Animal AnesthesiaLesley J. SmithNo ratings yet
- Comparison of The Ferno Scoop Stretcher With The Long Backboard For Spinal ImmobilizationDocument7 pagesComparison of The Ferno Scoop Stretcher With The Long Backboard For Spinal ImmobilizationLeandro NogueiraNo ratings yet
- Schroeder 2018Document10 pagesSchroeder 2018Leandro NogueiraNo ratings yet
- Injury Patterns and Causes of Death in 953 Patients With Penetrating Abdominal War Wounds in A Civilian Independent Non-Governmental Organization Hospital in Lashkargah, AfghanistanDocument8 pagesInjury Patterns and Causes of Death in 953 Patients With Penetrating Abdominal War Wounds in A Civilian Independent Non-Governmental Organization Hospital in Lashkargah, AfghanistanLeandro NogueiraNo ratings yet
- Current Thinking Cervical Collar Use in SMR May 2019Document5 pagesCurrent Thinking Cervical Collar Use in SMR May 2019Leandro NogueiraNo ratings yet
- Olaus Sen 2017Document7 pagesOlaus Sen 2017Leandro NogueiraNo ratings yet
- Jones 2014Document8 pagesJones 2014Leandro NogueiraNo ratings yet
- 10 1016@j Amj 2020 07 009Document6 pages10 1016@j Amj 2020 07 009Leandro NogueiraNo ratings yet
- Self-Extrication and Selective Spinal Immobilisation in A Polytrauma Patient With Spinal InjuriesDocument4 pagesSelf-Extrication and Selective Spinal Immobilisation in A Polytrauma Patient With Spinal InjuriesLeandro NogueiraNo ratings yet
- Ventilator Management of Adult Patients in The Emergency DepartmentDocument20 pagesVentilator Management of Adult Patients in The Emergency DepartmentLeandro NogueiraNo ratings yet
- START Versus SALT Triage: Which Is Preferred by The 21 Century Health Care Student?Document6 pagesSTART Versus SALT Triage: Which Is Preferred by The 21 Century Health Care Student?Leandro NogueiraNo ratings yet
- Monro-Kellie 2.0: The Dynamic Vascular and Venous Pathophysiological Components of Intracranial PressureDocument13 pagesMonro-Kellie 2.0: The Dynamic Vascular and Venous Pathophysiological Components of Intracranial PressureLeandro NogueiraNo ratings yet
- E230 FullDocument10 pagesE230 FullLeandro NogueiraNo ratings yet
- Chapter 2 Static EquilibriumDocument19 pagesChapter 2 Static Equilibriumshahrul100% (1)
- Kunci-Jawaban Howard AntonDocument41 pagesKunci-Jawaban Howard AntonAlyagariniNo ratings yet
- Experiment # 15: LABORATORY MANUAL For ENGR2860U-Fluid MechanicsDocument10 pagesExperiment # 15: LABORATORY MANUAL For ENGR2860U-Fluid MechanicsAbdullah Alshihri100% (1)
- UAV - NPTEL - IIT RoorkeeDocument14 pagesUAV - NPTEL - IIT Roorkeesankalp chopkarNo ratings yet
- Navodaya Vidyalaya Samiti Navodaya Vidyalaya Samiti Navodaya Vidyalaya SamitiDocument31 pagesNavodaya Vidyalaya Samiti Navodaya Vidyalaya Samiti Navodaya Vidyalaya Samiticat manNo ratings yet
- GC - Interview QuestionsDocument7 pagesGC - Interview QuestionsSasiNo ratings yet
- Manual Usuario NSX-AV800Document80 pagesManual Usuario NSX-AV800observador1980No ratings yet
- Garden Seed Handbook Part 31Document5 pagesGarden Seed Handbook Part 31gezarolNo ratings yet
- Experiment 1 Safety Measures: Use and Preparation of Chemical Substance 1.1 ObjectivesDocument8 pagesExperiment 1 Safety Measures: Use and Preparation of Chemical Substance 1.1 ObjectivesMaldini JosnonNo ratings yet
- Mendoza EAPP Q1 Module 2 Week 2 Structure of An Academic TextDocument10 pagesMendoza EAPP Q1 Module 2 Week 2 Structure of An Academic TextEllie Pasion67% (3)
- GU 0009. Leisegang Colposcope Directions ForUseDocument44 pagesGU 0009. Leisegang Colposcope Directions ForUseGabriela Ponce GuerrerpNo ratings yet
- ISO 22301 Lead Implementer - Two Page BrochureDocument2 pagesISO 22301 Lead Implementer - Two Page BrochurePECBCERTIFICATIONNo ratings yet
- Chapter 12: Personality Assessment - An Overview What Is Personality?Document4 pagesChapter 12: Personality Assessment - An Overview What Is Personality?John ArthurNo ratings yet
- 5.2 Extreme Value Theorem, Global Versus Local Extrema, and CriticalDocument26 pages5.2 Extreme Value Theorem, Global Versus Local Extrema, and Criticalazzamomar2018No ratings yet
- Overview of Extended RealityDocument7 pagesOverview of Extended RealityAkul DevtaNo ratings yet
- Saim NotesDocument120 pagesSaim NotesJagmohan Bisht0% (1)
- Government Polytechnic, Nanded: Title of The ProjectDocument24 pagesGovernment Polytechnic, Nanded: Title of The ProjectPradip GaikwadNo ratings yet
- Service Recovery - Making It RightDocument25 pagesService Recovery - Making It RightRavan RajanNo ratings yet
- FunctionDocument3 pagesFunctionGeraldo RochaNo ratings yet
- Playbook Overcoming Cloud Security ConcernsDocument8 pagesPlaybook Overcoming Cloud Security Concernsshekhar785424No ratings yet
- Irp Test-1 (07!12!17) (Solution) (Jee Mains) Code-AbDocument20 pagesIrp Test-1 (07!12!17) (Solution) (Jee Mains) Code-Abvejoshi21699No ratings yet
- Ce Booklet Fall 14Document28 pagesCe Booklet Fall 14api-279863771No ratings yet
- QC DissertationDocument85 pagesQC DissertationAhmed MahmoudNo ratings yet
- Detailed Lesson PlanDocument12 pagesDetailed Lesson PlanIrishNo ratings yet
- Ashok Mali ReportDocument1 pageAshok Mali ReportAshok MaliNo ratings yet