Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Words That Look Alike: Pass The TOEIC TestDocument2 pagesWords That Look Alike: Pass The TOEIC TestLành CaNo ratings yet
- Is Resilience Only Skin Deep Rural African Americans' Socioeconomic Status-Related Risk and CompetenceDocument10 pagesIs Resilience Only Skin Deep Rural African Americans' Socioeconomic Status-Related Risk and CompetenceSerap KaralarNo ratings yet
- Income As A Resilience Factor For The Impact of Discrimination and Institutional Unfairness On Minorities' Emotional Well-BeingDocument12 pagesIncome As A Resilience Factor For The Impact of Discrimination and Institutional Unfairness On Minorities' Emotional Well-BeingSerap KaralarNo ratings yet
- Age and Gender Effects On Resilience in Children and AdolescentsDocument11 pagesAge and Gender Effects On Resilience in Children and AdolescentsSerap KaralarNo ratings yet
- Harry J. Aponte, Karni Kissil - The Person of The Therapist Training Model - Mastering The Use of Self (2016, Routledge)Document165 pagesHarry J. Aponte, Karni Kissil - The Person of The Therapist Training Model - Mastering The Use of Self (2016, Routledge)Serap Karalar100% (1)
- Performance Correction Chart of Centrifugal Oil Pump For Handling Viscous LiquidsDocument7 pagesPerformance Correction Chart of Centrifugal Oil Pump For Handling Viscous LiquidsalikajbafNo ratings yet
- Advent Jesse Tree - 2013Document35 pagesAdvent Jesse Tree - 2013Chad Bragg100% (1)
- POSTMODERN, 253s '12Document270 pagesPOSTMODERN, 253s '12Raluca Gîlcă100% (1)
- High Court of Judicature at Allahabad: Case Status - CRIMINAL MISC. BAIL APPLICATION (BAIL) - (23700/2022)Document2 pagesHigh Court of Judicature at Allahabad: Case Status - CRIMINAL MISC. BAIL APPLICATION (BAIL) - (23700/2022)Ritesh SinghNo ratings yet
- DBEBEE601Document4 pagesDBEBEE601bariNo ratings yet
- Ca17 Activity 1Document2 pagesCa17 Activity 1Mark Kenneth CeballosNo ratings yet
- Open-Source Software For Automated Rodent Behavioral AnalysisDocument12 pagesOpen-Source Software For Automated Rodent Behavioral AnalysisGonzalo OrtegaNo ratings yet
- CLPWPost War Literary WorksDocument4 pagesCLPWPost War Literary WorksRohann Ban0% (1)
- Riko Technical Brochure PDFDocument29 pagesRiko Technical Brochure PDFGrigoreOzonNo ratings yet
- The Pisces Sagittarius SquareDocument3 pagesThe Pisces Sagittarius SquarejakilaNo ratings yet
- Sexy Book 121Document252 pagesSexy Book 121Irepan Ponce50% (2)
- MCQ-Environmental StudiesDocument45 pagesMCQ-Environmental StudiesShabana Yasmin67% (6)
- CGR Project Report DDGGDDDocument21 pagesCGR Project Report DDGGDDTanvi KodoliNo ratings yet
- Lista MF 01 - 05 - 2015Document11 pagesLista MF 01 - 05 - 2015CsordásCsaba-JózsefNo ratings yet
- RahmaDocument3 pagesRahmaAyyub RamadanNo ratings yet
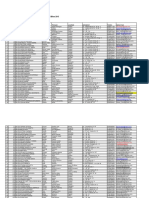
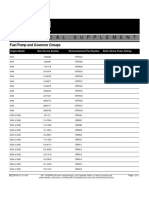
- FuelPump&GovernorGroups SELD0135 11Document11 pagesFuelPump&GovernorGroups SELD0135 11narit00007No ratings yet
- Bir Regulations MonitoringDocument87 pagesBir Regulations MonitoringErica NicolasuraNo ratings yet
- A History of Forestry in SarawakDocument9 pagesA History of Forestry in SarawakNur HaleemNo ratings yet
- (With Script) June 2021 Saturday WSF Teaching GuideDocument3 pages(With Script) June 2021 Saturday WSF Teaching GuideMichael T. BelloNo ratings yet
- 17 Artikel Analisis Komponen Produk Wisata Di Kabupaten KarawangDocument10 pages17 Artikel Analisis Komponen Produk Wisata Di Kabupaten KarawangPutri NurkarimahNo ratings yet
- ECL-ACC980 ManualDocument4 pagesECL-ACC980 ManualAneal LiverpoolNo ratings yet
- Tia HistoryDocument11 pagesTia HistoryTiara AlmeidaNo ratings yet
- Smart VOC Recovery Systems: PolarisDocument6 pagesSmart VOC Recovery Systems: PolarisDaniel SetyadiNo ratings yet
- Spare Parts CatalogueDocument45 pagesSpare Parts CatalogueАлексей ДомнинNo ratings yet
- International Business: Case Study-Report-3 18-02-2022Document5 pagesInternational Business: Case Study-Report-3 18-02-2022swapnil anandNo ratings yet
- Motor Claim Form THE ORIENTAL INSURANCE CO. LTD.Document4 pagesMotor Claim Form THE ORIENTAL INSURANCE CO. LTD.rajiv.surveyor7145No ratings yet
- Apbush DBQDocument2 pagesApbush DBQMaria Ines Carrillo100% (1)
- Celebrating The Third Place Inspiring Stories About The Great Good Places at The Heart of Our Communities (Oldenburg, Ray) (Z-Library)Document210 pagesCelebrating The Third Place Inspiring Stories About The Great Good Places at The Heart of Our Communities (Oldenburg, Ray) (Z-Library)ferialNo ratings yet
- The Colometric StructureDocument26 pagesThe Colometric StructureMerletoNo ratings yet