Download as pdf or txt
You might also like
- EMQs For Medical Students Volume 3 PDFDocument15 pagesEMQs For Medical Students Volume 3 PDFAbdulaziz Al-Araifi0% (1)
- 057608komatsu Hydraulic Oil HO 46-HMDocument5 pages057608komatsu Hydraulic Oil HO 46-HMrolex21No ratings yet
- Depathologizing Psychopathology The Neuroscience of Mental Illness and Its TreatmentDocument185 pagesDepathologizing Psychopathology The Neuroscience of Mental Illness and Its TreatmentBreno Costa100% (1)
- HypercalcemiaDocument6 pagesHypercalcemiajamil aoudeNo ratings yet
- B2 PDFDocument9 pagesB2 PDFDr. Arvind YadavNo ratings yet
- Bilezikian 2017Document11 pagesBilezikian 2017Widya Arina WinataNo ratings yet
- Calcium-Bone Metabolism Case DiscussionsDocument10 pagesCalcium-Bone Metabolism Case DiscussionswhooziesNo ratings yet
- Anorexia & Lethargy in A Dog With Presumed GiardiasisDocument4 pagesAnorexia & Lethargy in A Dog With Presumed GiardiasisMiruna ChiriacNo ratings yet
- Management of Normocalcemic Primary HyperparathyroidismDocument19 pagesManagement of Normocalcemic Primary HyperparathyroidismErika AvilaNo ratings yet
- Veterinary Internal Medicne - 2016 - Gold - Evaluation of Basal Serum or Plasma Cortisol Concentrations for the DiagnosisDocument8 pagesVeterinary Internal Medicne - 2016 - Gold - Evaluation of Basal Serum or Plasma Cortisol Concentrations for the Diagnosiskarinaramos.alunoNo ratings yet
- Pi Is 0272638618300167Document3 pagesPi Is 0272638618300167Marisa IzzaNo ratings yet
- Hypokalemic NephropathyDocument7 pagesHypokalemic NephropathyGoris HariyadiNo ratings yet
- HipercalcemiaDocument4 pagesHipercalcemiadrichard123No ratings yet
- J of Bone Mineral Res - 2022 - El Hajj Fuleihan - Classical and Nonclassical Manifestations of PrimaryDocument21 pagesJ of Bone Mineral Res - 2022 - El Hajj Fuleihan - Classical and Nonclassical Manifestations of Primarykobag87897No ratings yet
- Hipercalcemia BJMDocument4 pagesHipercalcemia BJMPedroUribeNo ratings yet
- Interpreting Laboratory Results: Key PointsDocument8 pagesInterpreting Laboratory Results: Key PointsMarjorie Joy GreciaNo ratings yet
- CA A Cancer J Clinicians - 2018 - Zagzag - Hypercalcemia and Cancer Differential Diagnosis and TreatmentDocument10 pagesCA A Cancer J Clinicians - 2018 - Zagzag - Hypercalcemia and Cancer Differential Diagnosis and TreatmentWilliam Perero RodríguezNo ratings yet
- American Journal of Emergency MedicineDocument3 pagesAmerican Journal of Emergency MedicineRina ErlinaNo ratings yet
- 10 1001@jama 2020 0538Document2 pages10 1001@jama 2020 0538Julio Alberto VásquezNo ratings yet
- Dob80024 451 458Document8 pagesDob80024 451 458Andreea StreuleaNo ratings yet
- Hypernatremia in Hospitalized Children 7380Document4 pagesHypernatremia in Hospitalized Children 7380menesesgilbertmd333No ratings yet
- Choroidal and Retinal Thickening in Severe Preeclampsia: RetinaDocument7 pagesChoroidal and Retinal Thickening in Severe Preeclampsia: RetinaAssifa RidzkiNo ratings yet
- 68-Year-Old Man With Fatigue, Fever, and Weight Loss PDFDocument4 pages68-Year-Old Man With Fatigue, Fever, and Weight Loss PDFRaghad Al-AnsariNo ratings yet
- American J Hematol - 2006 - Takahashi - Methylprednisolone Pulse Therapy For Severe Immune Thrombocytopenia Associated WithDocument5 pagesAmerican J Hematol - 2006 - Takahashi - Methylprednisolone Pulse Therapy For Severe Immune Thrombocytopenia Associated WithMohan PrasadNo ratings yet
- Hiperparatiroidismo PrimarioDocument10 pagesHiperparatiroidismo Primariopruebaprueba321765No ratings yet
- A Rare Complication of Pauci-Immune Crescentic Glomerulonephritis in A Child: QuestionsDocument2 pagesA Rare Complication of Pauci-Immune Crescentic Glomerulonephritis in A Child: QuestionsadiNo ratings yet
- Mjhid 7 1 E2015036Document3 pagesMjhid 7 1 E2015036Admin neuro-usu.idNo ratings yet
- Accepted Manuscript: Topics in Companion Animal MedicineDocument21 pagesAccepted Manuscript: Topics in Companion Animal MedicinedanielleclimacoNo ratings yet
- Systemic Amyloidosis in Primary Hyperparathyroidism. Kam Newman, Mojtaba Akhtari, Salim Shackour, Ajit KesaniDocument1 pageSystemic Amyloidosis in Primary Hyperparathyroidism. Kam Newman, Mojtaba Akhtari, Salim Shackour, Ajit KesanijingerbrunoNo ratings yet
- Carrick 2018Document7 pagesCarrick 2018Edwin AlvarezNo ratings yet
- Case Report: Grace Y. Kim, MD Helen Anaedo, MD Sahar Nozad, MD Tipu Nazeer, MD Hassan Shawa, MDDocument6 pagesCase Report: Grace Y. Kim, MD Helen Anaedo, MD Sahar Nozad, MD Tipu Nazeer, MD Hassan Shawa, MDPedro Gómez RNo ratings yet
- Renal Limited Anti Neutrophil Cytoplasmic Antibody Associated Vasculitis A Case ReportDocument5 pagesRenal Limited Anti Neutrophil Cytoplasmic Antibody Associated Vasculitis A Case ReportAthenaeum Scientific PublishersNo ratings yet
- A Case of Severe Hypertriglyceridaemia and HypercholesterolaemiaDocument1 pageA Case of Severe Hypertriglyceridaemia and Hypercholesterolaemiathys2000No ratings yet
- Recurrent Renal Colic: A Case StudyDocument2 pagesRecurrent Renal Colic: A Case StudyTheQueensafa90No ratings yet
- Rachel I Gafni Hypoparathyroidism 2019Document10 pagesRachel I Gafni Hypoparathyroidism 2019Ibrahim SabraNo ratings yet
- Validation Biochemistry MeasurementDocument35 pagesValidation Biochemistry Measurementhudan aziziNo ratings yet
- 2482 8791 1 PBDocument2 pages2482 8791 1 PBMuhammad Irvan AvandiNo ratings yet
- Best Practice Primary Care 8Document9 pagesBest Practice Primary Care 8Sisca PrimaNo ratings yet
- Parathyroid ImagingDocument6 pagesParathyroid ImagingjeffsunilNo ratings yet
- Clinical Management of Hyperkalemia: ReviewDocument19 pagesClinical Management of Hyperkalemia: ReviewRawan KhateebNo ratings yet
- Mahmud (2007) Coma With Diffuse White Matter Hemorrhages PDFDocument9 pagesMahmud (2007) Coma With Diffuse White Matter Hemorrhages PDFFelicia HarsonoNo ratings yet
- Recurrent Nephrolithiasis in A 9-Year-Old Child: (University of North Carolina, Chapel Hill, NC)Document4 pagesRecurrent Nephrolithiasis in A 9-Year-Old Child: (University of North Carolina, Chapel Hill, NC)Shaysta KhanNo ratings yet
- A Novel Missense CASR Gene Sequence Variation Resulting - 2022 - AACE Clinical CDocument5 pagesA Novel Missense CASR Gene Sequence Variation Resulting - 2022 - AACE Clinical CMohammed Shuaib AhmedNo ratings yet
- A Rare Case of Familial Neurogenic Diabetes Insipidu - 2021 - AACE Clinical CaseDocument4 pagesA Rare Case of Familial Neurogenic Diabetes Insipidu - 2021 - AACE Clinical CaseShuaib AhmedNo ratings yet
- Clinical Review: The Diagnosis and Management of HypercalcaemiaDocument9 pagesClinical Review: The Diagnosis and Management of HypercalcaemiaivanilhskyNo ratings yet
- Oxford University PressDocument9 pagesOxford University PresssarafraunaqNo ratings yet
- A Curious Case of QuadriplegiaDocument4 pagesA Curious Case of QuadriplegiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Educational Case: Anemia in A Neonate: Megan E. Kachur, MD and Benjamin J. Rosen, DODocument9 pagesEducational Case: Anemia in A Neonate: Megan E. Kachur, MD and Benjamin J. Rosen, DOL ANo ratings yet
- Paraneoplastic Limbic Encephalitis From A Carotid Body Paraganglioma Presenting As Persistent and Worsening ConfusionDocument7 pagesParaneoplastic Limbic Encephalitis From A Carotid Body Paraganglioma Presenting As Persistent and Worsening ConfusionAthenaeum Scientific PublishersNo ratings yet
- Case HipotiroidDocument3 pagesCase HipotiroidVivi DeviyanaNo ratings yet
- Case Report: Surgical Removal of A Canine Aortic Thromboembolism Secondary To PancreatitisDocument8 pagesCase Report: Surgical Removal of A Canine Aortic Thromboembolism Secondary To PancreatitisIvan RisnaNo ratings yet
- Veterinary Internal Medicne - 2013 - Behrend - Diagnosis of Spontaneous Canine Hyperadrenocorticism 2012 ACVIM ConsensusDocument13 pagesVeterinary Internal Medicne - 2013 - Behrend - Diagnosis of Spontaneous Canine Hyperadrenocorticism 2012 ACVIM ConsensusCicero HélioNo ratings yet
- Bilateral Basal Ganglia Calcification Fahrs DiseaDocument9 pagesBilateral Basal Ganglia Calcification Fahrs DiseaSonia TivadarNo ratings yet
- Glucose 6 Phosphate DefDocument3 pagesGlucose 6 Phosphate DefJoey MaravillasNo ratings yet
- Nephrolithiasis in A 9 Year OldDocument4 pagesNephrolithiasis in A 9 Year OldJasmin Kae SistosoNo ratings yet
- Hypocalcemia After Total Thyroidectomy in Graves Disease: Original Research & ContributionsDocument4 pagesHypocalcemia After Total Thyroidectomy in Graves Disease: Original Research & ContributionsInggritNo ratings yet
- Hypoparathyroidism NEJM 2019 PDFDocument10 pagesHypoparathyroidism NEJM 2019 PDFalejandro toro riveraNo ratings yet
- ICSH Guidelines For The Laboratory Diagnosis of Nonimmune Hereditary Red Cell Membrane DisordersDocument22 pagesICSH Guidelines For The Laboratory Diagnosis of Nonimmune Hereditary Red Cell Membrane DisordersSofia BujosaNo ratings yet
- DX de Las Enfermedades No Inmunologicas de La Membrana Del EritorcitoDocument22 pagesDX de Las Enfermedades No Inmunologicas de La Membrana Del EritorcitoMiguel Angel Hernandez SerratoNo ratings yet
- ICSH Guidelines For The Laboratory Diagnosis of Nonimmune Hereditary Red Cell Membrane DisordersDocument22 pagesICSH Guidelines For The Laboratory Diagnosis of Nonimmune Hereditary Red Cell Membrane DisordersSofia BujosaNo ratings yet
- Hypokalaemia Periodic Paralysis: Liam J StapletonDocument4 pagesHypokalaemia Periodic Paralysis: Liam J StapletonJL DeomampoNo ratings yet
- Labs & Imaging for Primary Eye Care: Optometry In Full ScopeFrom EverandLabs & Imaging for Primary Eye Care: Optometry In Full ScopeNo ratings yet
- Diabetic Ketoacidosis Complicating Gestational Dia - 2022 - AACE Clinical Case RDocument3 pagesDiabetic Ketoacidosis Complicating Gestational Dia - 2022 - AACE Clinical Case RMohammed Shuaib AhmedNo ratings yet
- A Novel Missense CASR Gene Sequence Variation Resulting - 2022 - AACE Clinical CDocument5 pagesA Novel Missense CASR Gene Sequence Variation Resulting - 2022 - AACE Clinical CMohammed Shuaib AhmedNo ratings yet
- Medicinal Chemistry Strategies Towards The Development - 2022 - Acta PharmaceutiDocument19 pagesMedicinal Chemistry Strategies Towards The Development - 2022 - Acta PharmaceutiMohammed Shuaib AhmedNo ratings yet
- A Case of Hypophysitis Associated With SARS CoV 2 - 2022 - AACE Clinical Case RDocument6 pagesA Case of Hypophysitis Associated With SARS CoV 2 - 2022 - AACE Clinical Case RMohammed Shuaib AhmedNo ratings yet
- A Boy With Progressive Cognitive Impairment and Da - 2022 - AACE Clinical Case RDocument2 pagesA Boy With Progressive Cognitive Impairment and Da - 2022 - AACE Clinical Case RMohammed Shuaib AhmedNo ratings yet
- Metabolic Dysregulation and Emerging Therapeutical Tar - 2022 - Acta PharmaceutiDocument23 pagesMetabolic Dysregulation and Emerging Therapeutical Tar - 2022 - Acta PharmaceutiMohammed Shuaib AhmedNo ratings yet
- Inhibition of Temperature Sensitive TRPV3 Channel by Two Na - 2022 - Acta PharmaDocument12 pagesInhibition of Temperature Sensitive TRPV3 Channel by Two Na - 2022 - Acta PharmaMohammed Shuaib AhmedNo ratings yet
- Preclinical Evaluation and Pilot Clinical Study of 18F Al - 2022 - Acta PharmacDocument9 pagesPreclinical Evaluation and Pilot Clinical Study of 18F Al - 2022 - Acta PharmacMohammed Shuaib AhmedNo ratings yet
- Inhibiting Collagen I Production and Tumor Cell Colonizatio - 2022 - Acta PharmaDocument13 pagesInhibiting Collagen I Production and Tumor Cell Colonizatio - 2022 - Acta PharmaMohammed Shuaib AhmedNo ratings yet
- Table of Contents - 2022 - Acta Pharmaceutica Sinica BDocument11 pagesTable of Contents - 2022 - Acta Pharmaceutica Sinica BMohammed Shuaib AhmedNo ratings yet
- The Cell Cycle Inhibitor P21 Promotes The Development of - 2022 - Acta PharmaceDocument12 pagesThe Cell Cycle Inhibitor P21 Promotes The Development of - 2022 - Acta PharmaceMohammed Shuaib AhmedNo ratings yet
- Targeting Whole Body Metabolism and Mitochondrial Bioener - 2022 - Acta PharmaceDocument21 pagesTargeting Whole Body Metabolism and Mitochondrial Bioener - 2022 - Acta PharmaceMohammed Shuaib AhmedNo ratings yet
- Coexistence of Cushing Disease With A Solitary Adrenocor - 2022 - AACE ClinicalDocument4 pagesCoexistence of Cushing Disease With A Solitary Adrenocor - 2022 - AACE ClinicalMohammed Shuaib AhmedNo ratings yet
- Adrenal Histoplasmosis A Therapeutic Restoration of - 2022 - AACE Clinical CaseDocument2 pagesAdrenal Histoplasmosis A Therapeutic Restoration of - 2022 - AACE Clinical CaseMohammed Shuaib AhmedNo ratings yet
- AACE Clinical Case Reports: John C. Parker, MD, Andreas G. Moraitis, MD, Joseph K. Belanoff, MDDocument5 pagesAACE Clinical Case Reports: John C. Parker, MD, Andreas G. Moraitis, MD, Joseph K. Belanoff, MDMohammed Shuaib AhmedNo ratings yet
- JSP 403 Vol 2 Chapter 2Document61 pagesJSP 403 Vol 2 Chapter 2SOOD ASSOCIATES GOANo ratings yet
- Training Tips For Hypertrophy - Renaissance Periodization - Dr. Mike IsraetelDocument7 pagesTraining Tips For Hypertrophy - Renaissance Periodization - Dr. Mike IsraetelShrenik NaharNo ratings yet
- Daftar Obat %pareto Dan Ven 15Document200 pagesDaftar Obat %pareto Dan Ven 15sofia nofiantiNo ratings yet
- Future Biotechnology: The Eurobiotech JournalDocument4 pagesFuture Biotechnology: The Eurobiotech JournalsaraNo ratings yet
- Aim Global TieupsDocument84 pagesAim Global Tieupsjhorgecruz18No ratings yet
- Individual Performance Commitment and Review (Ipcr) : Name of Employee: Approved By: Date Date FiledDocument12 pagesIndividual Performance Commitment and Review (Ipcr) : Name of Employee: Approved By: Date Date FiledTiffanny Diane Agbayani RuedasNo ratings yet
- Microbial PathogenesisDocument8 pagesMicrobial PathogenesisRachelleNo ratings yet
- Passenger Locator Form: Non-Red ListDocument4 pagesPassenger Locator Form: Non-Red ListSamadrukNo ratings yet
- Journal Medicine: The New EnglandDocument7 pagesJournal Medicine: The New EnglandTony RamirezNo ratings yet
- Behcet's Disease (Adamantiades Syndrome) : DefinitionDocument9 pagesBehcet's Disease (Adamantiades Syndrome) : DefinitionNuzairah AynoorNo ratings yet
- Rabbit KeepingDocument12 pagesRabbit KeepingMoses NdwaruNo ratings yet
- Betz Rebecca ResumeDocument2 pagesBetz Rebecca Resumeapi-316054946No ratings yet
- Vocabulary Set 28 - TAX ON FAST FOODDocument4 pagesVocabulary Set 28 - TAX ON FAST FOODchung hieuNo ratings yet
- Deep Fat FryingDocument2 pagesDeep Fat FryingalinawidagdoNo ratings yet
- Prevention & Management of Sports Injuries: Quimcy Dsouza Fybms-Sm (B) 75Document26 pagesPrevention & Management of Sports Injuries: Quimcy Dsouza Fybms-Sm (B) 75Quimcy100% (1)
- Substance AbuseDocument54 pagesSubstance AbuseCharles CastilloNo ratings yet
- Case StudiesDocument5 pagesCase StudiesPou PunzalanNo ratings yet
- Blood Bank EquipmentsDocument12 pagesBlood Bank EquipmentsJomar100% (1)
- Health ServicesDocument3 pagesHealth ServicesReizza Mae NecesitoNo ratings yet
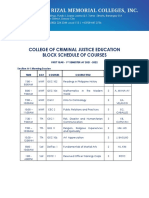
- College of Criminal Justice Education Block Schedule of CoursesDocument12 pagesCollege of Criminal Justice Education Block Schedule of CoursesKristel Ann ManlangitNo ratings yet
- Name: Rank: Date: Quiz On IMO Conventions 1. Write True or FalseDocument3 pagesName: Rank: Date: Quiz On IMO Conventions 1. Write True or FalseBisratNo ratings yet
- Green Light Surgical GuideDocument88 pagesGreen Light Surgical GuidekbrinaldiNo ratings yet
- Language Disorders - 5Document27 pagesLanguage Disorders - 5Marta Sampedro GonzalezNo ratings yet
- Diet For Patient With Parkinson's DiseaseDocument2 pagesDiet For Patient With Parkinson's DiseaseNuzulina SafiraNo ratings yet
- Purine Rich FoodDocument3 pagesPurine Rich Foodttstanescu4506No ratings yet
- WEEK 2: 12A, 12B, 12G Ôn Tập Khảo Sát Pronunciation ClosestDocument6 pagesWEEK 2: 12A, 12B, 12G Ôn Tập Khảo Sát Pronunciation ClosestHàNhậtNguyễnNo ratings yet
- Molly McDowell - Course Project Part 1Document5 pagesMolly McDowell - Course Project Part 1Adelaide DariaNo ratings yet
- Rose Doe v. The City of New York, Et. Al.Document57 pagesRose Doe v. The City of New York, Et. Al.Daily Caller News FoundationNo ratings yet