
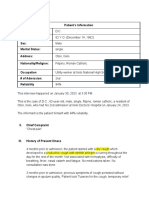
Case
Case
You might also like
- Mona Hernandez Care PlanDocument11 pagesMona Hernandez Care PlanKarina Rodriguez80% (5)
- Carl Rogers Counsels An Individual On Anger - TranscriptDocument18 pagesCarl Rogers Counsels An Individual On Anger - TranscriptAndrew Williams100% (1)
- DeVry HIT 111 All Discussions - LatestDocument11 pagesDeVry HIT 111 All Discussions - Latestshonwilllen0% (1)
- Tina Jones Heent Soap Note Episodic VisitDocument5 pagesTina Jones Heent Soap Note Episodic VisitMallory ZaborNo ratings yet
- Case Study - Chronic BronchitisDocument5 pagesCase Study - Chronic BronchitisPatrick PrepotenteNo ratings yet
- Nbme 1 Block 1-4Document75 pagesNbme 1 Block 1-4Eimad Atif100% (1)
- Care of The Patient With COVID-19 COVID Case Study 2Document3 pagesCare of The Patient With COVID-19 COVID Case Study 2Ashley HernandezNo ratings yet
- Pediatric Respiratory Cases: DR Hodan S. Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUDocument24 pagesPediatric Respiratory Cases: DR Hodan S. Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUmukhtar abddiNo ratings yet
- Bronchiolitis - Discharge SummaryDocument2 pagesBronchiolitis - Discharge SummaryIndranil SinhaNo ratings yet
- CroupDocument19 pagesCroupEmily EresumaNo ratings yet
- Influenza: The Hundred-Year Hunt to Cure the 1918 Spanish Flu PandemicFrom EverandInfluenza: The Hundred-Year Hunt to Cure the 1918 Spanish Flu PandemicRating: 4 out of 5 stars4/5 (39)
- Rutherford: Vascular Surgery, 6th EdDocument6 pagesRutherford: Vascular Surgery, 6th EdanitaromeroNo ratings yet
- Writing Case Notes (Analysis) - Gem AlbertsDocument6 pagesWriting Case Notes (Analysis) - Gem AlbertsJunwehNo ratings yet
- Chapter 10Document4 pagesChapter 10Srinu WestNo ratings yet
- Cases Resp - SystemDocument12 pagesCases Resp - SystemJerin XavierNo ratings yet
- MicroDocument12 pagesMicroSuman MahmoodNo ratings yet
- SITUATIONDocument2 pagesSITUATIONJulius Earl MarquezNo ratings yet
- Anaphylaxis - Berry2019 PDFDocument3 pagesAnaphylaxis - Berry2019 PDFRendi Saputra YogaNo ratings yet
- Kasus 1 Deskripsi:: Evaluate Identify InterveneDocument2 pagesKasus 1 Deskripsi:: Evaluate Identify InterveneAisha Putri SNo ratings yet
- G1 3F Case1 PnuemoniaDocument25 pagesG1 3F Case1 PnuemoniaEduard GarchitorenaNo ratings yet
- Case Scenario For Different Groups PDFDocument8 pagesCase Scenario For Different Groups PDFWallen Jey VelascoNo ratings yet
- Case StudyDocument10 pagesCase StudyShaNaya ZarinNo ratings yet
- Case Scenarios: Scenario 1Document2 pagesCase Scenarios: Scenario 1Kym RonquilloNo ratings yet
- A Case Study of A 1-Year-Old Child Diagnosed With Bronchial Asthma in Acute ExacerbationDocument36 pagesA Case Study of A 1-Year-Old Child Diagnosed With Bronchial Asthma in Acute ExacerbationKyra Bianca R. FamacionNo ratings yet
- Quiz 2 Alternative ToxicologyDocument8 pagesQuiz 2 Alternative Toxicologyfarhanyasser34No ratings yet
- CASE 1 Patient DCDocument6 pagesCASE 1 Patient DCDonnaLyssaReyesReunirNo ratings yet
- G 3 NCM 122 Lab BSN 4 2 FinalDocument67 pagesG 3 NCM 122 Lab BSN 4 2 FinalPam RomeroNo ratings yet
- Ards Case StudyDocument1 pageArds Case StudyLyons MacNo ratings yet
- Cases - CoughDocument5 pagesCases - CoughSarthak DubeyNo ratings yet
- Case Write-Up Influenza ADocument17 pagesCase Write-Up Influenza AA MNo ratings yet
- QCM Ped PulmoDocument8 pagesQCM Ped PulmoWahbi KhalidNo ratings yet
- PneumoniaDocument102 pagesPneumoniaJay Kumar100% (1)
- 57-Year-Old Woman With Covid-19 and DelusionsDocument9 pages57-Year-Old Woman With Covid-19 and DelusionsNazly ÁlvarezNo ratings yet
- Espiritu, Charles Anthony C.Document8 pagesEspiritu, Charles Anthony C.Charles AnthonyNo ratings yet
- Hypoxia and DyspneaDocument30 pagesHypoxia and DyspneaNgurah Arya PradnyantaraNo ratings yet
- ScenarioDocument5 pagesScenarioMei Marie MangubatNo ratings yet
- Dengue Case PresentationDocument4 pagesDengue Case PresentationLovelle LopezNo ratings yet
- Mentalt Health 6-116Document16 pagesMentalt Health 6-116Osama NasrNo ratings yet
- Case Study Week 1 Community Acquired Pneumonia 1Document6 pagesCase Study Week 1 Community Acquired Pneumonia 1Yuuki Chitose (tai-kun)No ratings yet
- Activity-5 - Branadj. DocumentationDocument3 pagesActivity-5 - Branadj. DocumentationbalabacrizleNo ratings yet
- Asthma CWUDocument8 pagesAsthma CWUNabilah ZulkiflyNo ratings yet
- Underlying Cause of Death and ICD 10 CompliantDocument17 pagesUnderlying Cause of Death and ICD 10 CompliantAhnaf MustaviNo ratings yet
- Clinical CaseDocument6 pagesClinical Casedani_zurita_1No ratings yet
- Cardio-Pulmo Discharge SummaryDocument2 pagesCardio-Pulmo Discharge SummaryIndranil Sinha100% (1)
- DANNY - RIVERA - MODIFIED VERSION - Episodic Visit TemplateDocument5 pagesDANNY - RIVERA - MODIFIED VERSION - Episodic Visit TemplateMallory ZaborNo ratings yet
- CLS 400 - Test 4 (Extra Credit)Document8 pagesCLS 400 - Test 4 (Extra Credit)McNeeseInsiderNo ratings yet
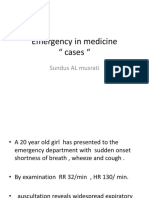
- Emergency in Medicine " Cases ": Sundus AL MusratiDocument38 pagesEmergency in Medicine " Cases ": Sundus AL MusratiHdzzNo ratings yet
- Case Presentation IM DDHDocument12 pagesCase Presentation IM DDHAishwarya BharathNo ratings yet
- 3 End of Life Gipsy GenesDocument2 pages3 End of Life Gipsy GenesADRIAN ISAAC GARZON PEREZNo ratings yet
- Cardio Case Scenario 3Document1 pageCardio Case Scenario 3Francis Josh DagohoyNo ratings yet
- The Flu: A Guide for Prevention and TreatmentFrom EverandThe Flu: A Guide for Prevention and TreatmentRating: 5 out of 5 stars5/5 (1)
- At the Edge of Mysteries: The Discovery of the Immune SystemFrom EverandAt the Edge of Mysteries: The Discovery of the Immune SystemNo ratings yet
- Strength, Resilience and Triumph: Living with Hydrocephalus: My StoryFrom EverandStrength, Resilience and Triumph: Living with Hydrocephalus: My StoryNo ratings yet
- Legionnaire's Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandLegionnaire's Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Natural Antibiotics and Antivirals: Homemade Herbal Remedies that Kill Pathogens and Cure Bacterial Infections and Allergies. Prevent Illness, Cold and FluFrom EverandNatural Antibiotics and Antivirals: Homemade Herbal Remedies that Kill Pathogens and Cure Bacterial Infections and Allergies. Prevent Illness, Cold and FluNo ratings yet
- Exam ObjectivesDocument232 pagesExam ObjectivesmustafaNo ratings yet
- Visual Impairment ScriptDocument3 pagesVisual Impairment Scriptapi-285548719No ratings yet
- History of Medicne: Body SystemsDocument27 pagesHistory of Medicne: Body SystemsLavendra KunwarNo ratings yet
- Internal Regulation Multiple Choice QuizDocument3 pagesInternal Regulation Multiple Choice Quizsbjon984924100% (1)
- Dental CariesDocument6 pagesDental Cariesyusuf230287No ratings yet
- Lesson Plan On Eating DisorderDocument17 pagesLesson Plan On Eating DisorderAnkush Kulat PatilNo ratings yet
- ACLF Guidelines 2023Document31 pagesACLF Guidelines 2023ctsakalakisNo ratings yet
- ImplementationDocument7 pagesImplementationAnonymous syRbQm6No ratings yet
- Cirrhosis Hepatic Group 5Document7 pagesCirrhosis Hepatic Group 5Nur Fadhillah Qurratul AinNo ratings yet
- Fast Track Diagnostics Assays Brochure 0917 FINAL 1800000004342593Document6 pagesFast Track Diagnostics Assays Brochure 0917 FINAL 1800000004342593Svasthya ManagerNo ratings yet
- SE - Henry-The Last LeafDocument6 pagesSE - Henry-The Last LeafCeren ManasNo ratings yet
- Benign SGD - PPTX Version 1Document32 pagesBenign SGD - PPTX Version 1Qazi ShahmeerNo ratings yet
- Infection Control IcuDocument37 pagesInfection Control IcuVidit JoshiNo ratings yet
- PremierUltra PA-BrochureDocument2 pagesPremierUltra PA-BrochureMay NgNo ratings yet
- BMI Classification WhoDocument1 pageBMI Classification WhoMuhammad Akrim100% (1)
- Anemia 1Document104 pagesAnemia 1maryam ijazNo ratings yet
- Poster Presentation CCRA Malang 2014Document3 pagesPoster Presentation CCRA Malang 2014alfarobi yogiNo ratings yet
- 06 Uncomplicated MalariaDocument16 pages06 Uncomplicated MalariaMwanja MosesNo ratings yet
- Six Arguments For A Greener DietDocument257 pagesSix Arguments For A Greener DietHuy PhạmNo ratings yet
- Anti-Microbial USMLE Review: Active RecallDocument32 pagesAnti-Microbial USMLE Review: Active Recallmehrzi kamelNo ratings yet
- Kumpulan Osce Ukmppd - BimaDocument2 pagesKumpulan Osce Ukmppd - BimaEddie Wyatt0% (1)
- Pleullar EffusionDocument20 pagesPleullar EffusionGopi GNo ratings yet
- What Is A Transjugular Intrahepatic Portosystemic Shunt (TIPS) ?Document7 pagesWhat Is A Transjugular Intrahepatic Portosystemic Shunt (TIPS) ?Tata Tamara Tam TamNo ratings yet
- Eating DisorderDocument5 pagesEating DisorderColesio Dianne Joyce AmisNo ratings yet
- TVP 2016 0102 OO AnisocoriaDocument7 pagesTVP 2016 0102 OO AnisocoriaRocioNo ratings yet
- PneumoconiosisDocument10 pagesPneumoconiosisDhruv patelNo ratings yet
- Case of OsteosarcomaDocument16 pagesCase of OsteosarcomaRanisha ArulrajahNo ratings yet
- Hikikomori: The Anti-Social Life That Many Japanese Youths AffectDocument3 pagesHikikomori: The Anti-Social Life That Many Japanese Youths AffectAgifa gumelarNo ratings yet




















































































Download as docx, pdf, or txt
You might also like
- Mona Hernandez Care PlanDocument11 pagesMona Hernandez Care PlanKarina Rodriguez80% (5)
- Carl Rogers Counsels An Individual On Anger - TranscriptDocument18 pagesCarl Rogers Counsels An Individual On Anger - TranscriptAndrew Williams100% (1)
- DeVry HIT 111 All Discussions - LatestDocument11 pagesDeVry HIT 111 All Discussions - Latestshonwilllen0% (1)
- Tina Jones Heent Soap Note Episodic VisitDocument5 pagesTina Jones Heent Soap Note Episodic VisitMallory ZaborNo ratings yet
- Case Study - Chronic BronchitisDocument5 pagesCase Study - Chronic BronchitisPatrick PrepotenteNo ratings yet
- Nbme 1 Block 1-4Document75 pagesNbme 1 Block 1-4Eimad Atif100% (1)
- Care of The Patient With COVID-19 COVID Case Study 2Document3 pagesCare of The Patient With COVID-19 COVID Case Study 2Ashley HernandezNo ratings yet
- Pediatric Respiratory Cases: DR Hodan S. Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUDocument24 pagesPediatric Respiratory Cases: DR Hodan S. Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUmukhtar abddiNo ratings yet
- Bronchiolitis - Discharge SummaryDocument2 pagesBronchiolitis - Discharge SummaryIndranil SinhaNo ratings yet
- CroupDocument19 pagesCroupEmily EresumaNo ratings yet
- Influenza: The Hundred-Year Hunt to Cure the 1918 Spanish Flu PandemicFrom EverandInfluenza: The Hundred-Year Hunt to Cure the 1918 Spanish Flu PandemicRating: 4 out of 5 stars4/5 (39)
- Rutherford: Vascular Surgery, 6th EdDocument6 pagesRutherford: Vascular Surgery, 6th EdanitaromeroNo ratings yet
- Writing Case Notes (Analysis) - Gem AlbertsDocument6 pagesWriting Case Notes (Analysis) - Gem AlbertsJunwehNo ratings yet
- Chapter 10Document4 pagesChapter 10Srinu WestNo ratings yet
- Cases Resp - SystemDocument12 pagesCases Resp - SystemJerin XavierNo ratings yet
- MicroDocument12 pagesMicroSuman MahmoodNo ratings yet
- SITUATIONDocument2 pagesSITUATIONJulius Earl MarquezNo ratings yet
- Anaphylaxis - Berry2019 PDFDocument3 pagesAnaphylaxis - Berry2019 PDFRendi Saputra YogaNo ratings yet
- Kasus 1 Deskripsi:: Evaluate Identify InterveneDocument2 pagesKasus 1 Deskripsi:: Evaluate Identify InterveneAisha Putri SNo ratings yet
- G1 3F Case1 PnuemoniaDocument25 pagesG1 3F Case1 PnuemoniaEduard GarchitorenaNo ratings yet
- Case Scenario For Different Groups PDFDocument8 pagesCase Scenario For Different Groups PDFWallen Jey VelascoNo ratings yet
- Case StudyDocument10 pagesCase StudyShaNaya ZarinNo ratings yet
- Case Scenarios: Scenario 1Document2 pagesCase Scenarios: Scenario 1Kym RonquilloNo ratings yet
- A Case Study of A 1-Year-Old Child Diagnosed With Bronchial Asthma in Acute ExacerbationDocument36 pagesA Case Study of A 1-Year-Old Child Diagnosed With Bronchial Asthma in Acute ExacerbationKyra Bianca R. FamacionNo ratings yet
- Quiz 2 Alternative ToxicologyDocument8 pagesQuiz 2 Alternative Toxicologyfarhanyasser34No ratings yet
- CASE 1 Patient DCDocument6 pagesCASE 1 Patient DCDonnaLyssaReyesReunirNo ratings yet
- G 3 NCM 122 Lab BSN 4 2 FinalDocument67 pagesG 3 NCM 122 Lab BSN 4 2 FinalPam RomeroNo ratings yet
- Ards Case StudyDocument1 pageArds Case StudyLyons MacNo ratings yet
- Cases - CoughDocument5 pagesCases - CoughSarthak DubeyNo ratings yet
- Case Write-Up Influenza ADocument17 pagesCase Write-Up Influenza AA MNo ratings yet
- QCM Ped PulmoDocument8 pagesQCM Ped PulmoWahbi KhalidNo ratings yet
- PneumoniaDocument102 pagesPneumoniaJay Kumar100% (1)
- 57-Year-Old Woman With Covid-19 and DelusionsDocument9 pages57-Year-Old Woman With Covid-19 and DelusionsNazly ÁlvarezNo ratings yet
- Espiritu, Charles Anthony C.Document8 pagesEspiritu, Charles Anthony C.Charles AnthonyNo ratings yet
- Hypoxia and DyspneaDocument30 pagesHypoxia and DyspneaNgurah Arya PradnyantaraNo ratings yet
- ScenarioDocument5 pagesScenarioMei Marie MangubatNo ratings yet
- Dengue Case PresentationDocument4 pagesDengue Case PresentationLovelle LopezNo ratings yet
- Mentalt Health 6-116Document16 pagesMentalt Health 6-116Osama NasrNo ratings yet
- Case Study Week 1 Community Acquired Pneumonia 1Document6 pagesCase Study Week 1 Community Acquired Pneumonia 1Yuuki Chitose (tai-kun)No ratings yet
- Activity-5 - Branadj. DocumentationDocument3 pagesActivity-5 - Branadj. DocumentationbalabacrizleNo ratings yet
- Asthma CWUDocument8 pagesAsthma CWUNabilah ZulkiflyNo ratings yet
- Underlying Cause of Death and ICD 10 CompliantDocument17 pagesUnderlying Cause of Death and ICD 10 CompliantAhnaf MustaviNo ratings yet
- Clinical CaseDocument6 pagesClinical Casedani_zurita_1No ratings yet
- Cardio-Pulmo Discharge SummaryDocument2 pagesCardio-Pulmo Discharge SummaryIndranil Sinha100% (1)
- DANNY - RIVERA - MODIFIED VERSION - Episodic Visit TemplateDocument5 pagesDANNY - RIVERA - MODIFIED VERSION - Episodic Visit TemplateMallory ZaborNo ratings yet
- CLS 400 - Test 4 (Extra Credit)Document8 pagesCLS 400 - Test 4 (Extra Credit)McNeeseInsiderNo ratings yet
- Emergency in Medicine " Cases ": Sundus AL MusratiDocument38 pagesEmergency in Medicine " Cases ": Sundus AL MusratiHdzzNo ratings yet
- Case Presentation IM DDHDocument12 pagesCase Presentation IM DDHAishwarya BharathNo ratings yet
- 3 End of Life Gipsy GenesDocument2 pages3 End of Life Gipsy GenesADRIAN ISAAC GARZON PEREZNo ratings yet
- Cardio Case Scenario 3Document1 pageCardio Case Scenario 3Francis Josh DagohoyNo ratings yet
- The Flu: A Guide for Prevention and TreatmentFrom EverandThe Flu: A Guide for Prevention and TreatmentRating: 5 out of 5 stars5/5 (1)
- At the Edge of Mysteries: The Discovery of the Immune SystemFrom EverandAt the Edge of Mysteries: The Discovery of the Immune SystemNo ratings yet
- Strength, Resilience and Triumph: Living with Hydrocephalus: My StoryFrom EverandStrength, Resilience and Triumph: Living with Hydrocephalus: My StoryNo ratings yet
- Legionnaire's Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandLegionnaire's Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Natural Antibiotics and Antivirals: Homemade Herbal Remedies that Kill Pathogens and Cure Bacterial Infections and Allergies. Prevent Illness, Cold and FluFrom EverandNatural Antibiotics and Antivirals: Homemade Herbal Remedies that Kill Pathogens and Cure Bacterial Infections and Allergies. Prevent Illness, Cold and FluNo ratings yet
- Exam ObjectivesDocument232 pagesExam ObjectivesmustafaNo ratings yet
- Visual Impairment ScriptDocument3 pagesVisual Impairment Scriptapi-285548719No ratings yet
- History of Medicne: Body SystemsDocument27 pagesHistory of Medicne: Body SystemsLavendra KunwarNo ratings yet
- Internal Regulation Multiple Choice QuizDocument3 pagesInternal Regulation Multiple Choice Quizsbjon984924100% (1)
- Dental CariesDocument6 pagesDental Cariesyusuf230287No ratings yet
- Lesson Plan On Eating DisorderDocument17 pagesLesson Plan On Eating DisorderAnkush Kulat PatilNo ratings yet
- ACLF Guidelines 2023Document31 pagesACLF Guidelines 2023ctsakalakisNo ratings yet
- ImplementationDocument7 pagesImplementationAnonymous syRbQm6No ratings yet
- Cirrhosis Hepatic Group 5Document7 pagesCirrhosis Hepatic Group 5Nur Fadhillah Qurratul AinNo ratings yet
- Fast Track Diagnostics Assays Brochure 0917 FINAL 1800000004342593Document6 pagesFast Track Diagnostics Assays Brochure 0917 FINAL 1800000004342593Svasthya ManagerNo ratings yet
- SE - Henry-The Last LeafDocument6 pagesSE - Henry-The Last LeafCeren ManasNo ratings yet
- Benign SGD - PPTX Version 1Document32 pagesBenign SGD - PPTX Version 1Qazi ShahmeerNo ratings yet
- Infection Control IcuDocument37 pagesInfection Control IcuVidit JoshiNo ratings yet
- PremierUltra PA-BrochureDocument2 pagesPremierUltra PA-BrochureMay NgNo ratings yet
- BMI Classification WhoDocument1 pageBMI Classification WhoMuhammad Akrim100% (1)
- Anemia 1Document104 pagesAnemia 1maryam ijazNo ratings yet
- Poster Presentation CCRA Malang 2014Document3 pagesPoster Presentation CCRA Malang 2014alfarobi yogiNo ratings yet
- 06 Uncomplicated MalariaDocument16 pages06 Uncomplicated MalariaMwanja MosesNo ratings yet
- Six Arguments For A Greener DietDocument257 pagesSix Arguments For A Greener DietHuy PhạmNo ratings yet
- Anti-Microbial USMLE Review: Active RecallDocument32 pagesAnti-Microbial USMLE Review: Active Recallmehrzi kamelNo ratings yet
- Kumpulan Osce Ukmppd - BimaDocument2 pagesKumpulan Osce Ukmppd - BimaEddie Wyatt0% (1)
- Pleullar EffusionDocument20 pagesPleullar EffusionGopi GNo ratings yet
- What Is A Transjugular Intrahepatic Portosystemic Shunt (TIPS) ?Document7 pagesWhat Is A Transjugular Intrahepatic Portosystemic Shunt (TIPS) ?Tata Tamara Tam TamNo ratings yet
- Eating DisorderDocument5 pagesEating DisorderColesio Dianne Joyce AmisNo ratings yet
- TVP 2016 0102 OO AnisocoriaDocument7 pagesTVP 2016 0102 OO AnisocoriaRocioNo ratings yet
- PneumoconiosisDocument10 pagesPneumoconiosisDhruv patelNo ratings yet
- Case of OsteosarcomaDocument16 pagesCase of OsteosarcomaRanisha ArulrajahNo ratings yet
- Hikikomori: The Anti-Social Life That Many Japanese Youths AffectDocument3 pagesHikikomori: The Anti-Social Life That Many Japanese Youths AffectAgifa gumelarNo ratings yet