
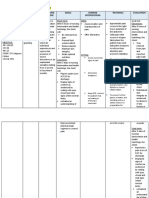
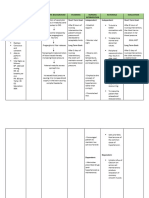
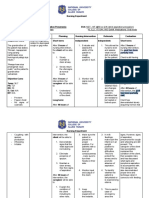
Case #4 Nursing Care Plan
Case #4 Nursing Care Plan
You might also like
- Nursing Care Plan For CholecystitisDocument4 pagesNursing Care Plan For CholecystitisEemyaj Jaymee88% (8)
- Nursing Care Plan PDFDocument6 pagesNursing Care Plan PDFEngely MercaderNo ratings yet
- NCP AnginaDocument3 pagesNCP AnginaShie LA100% (1)
- HeliotherapyDocument26 pagesHeliotherapyalmont1759No ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanMariel GamaloNo ratings yet
- Nursing Care Plan Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationDocument4 pagesNursing Care Plan Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationAngelica Charisse BuliganNo ratings yet
- Nursing Care Plan For Myocardial InfarctionDocument7 pagesNursing Care Plan For Myocardial InfarctionRocelyn CristobalNo ratings yet
- Nursing Care Plan For Myocardial InfarctionDocument7 pagesNursing Care Plan For Myocardial InfarctionjamieboyRN88% (8)
- NCP TahbsoDocument18 pagesNCP TahbsoUzziah Dharambai GurbuxaniNo ratings yet
- Perioperative Nursing Care Plan TAHBSODocument4 pagesPerioperative Nursing Care Plan TAHBSOPatricia OrtegaNo ratings yet
- Long Term: PT Will Demonstrate Increased Tolerance To Activity by DischargeDocument18 pagesLong Term: PT Will Demonstrate Increased Tolerance To Activity by DischargeMary Ann Ebol0% (1)
- Erica Marie L. Escanda BSN 3-A Group 2: Hyperthermia Related ToDocument3 pagesErica Marie L. Escanda BSN 3-A Group 2: Hyperthermia Related ToErica Marie EscandaNo ratings yet
- Nursing Care Plan Age: 60 Years OldDocument4 pagesNursing Care Plan Age: 60 Years OldLouise GudmalinNo ratings yet
- ACUTE PAIN BSN III KOLCABA NCP 8th ROTATIONDocument4 pagesACUTE PAIN BSN III KOLCABA NCP 8th ROTATIONKrisheille Amano MirandaNo ratings yet
- NCP FinalDocument10 pagesNCP FinalAlessandro MadrigalNo ratings yet
- NCP Estoesta HemorrhageDocument5 pagesNCP Estoesta HemorrhageKyle Albert EstoestaNo ratings yet
- Case Study Myocardial InfarctionDocument23 pagesCase Study Myocardial InfarctionJester GalayNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Rationale Planning Intervention S Rationale EvaluationDocument7 pagesNursing Care Plan: Assessment Nursing Diagnosis Rationale Planning Intervention S Rationale EvaluationNo EulNo ratings yet
- Nursing Care PlansDocument16 pagesNursing Care PlansJobelle AcenaNo ratings yet
- Nursing Care Plan TemplateDocument5 pagesNursing Care Plan TemplateKyle Albert EstoestaNo ratings yet
- Nursing Care Plan 1Document4 pagesNursing Care Plan 1Kiko BernardinoNo ratings yet
- NCP - BSN12F - Pumbaya (Module 4)Document3 pagesNCP - BSN12F - Pumbaya (Module 4)Ellah PumbayaNo ratings yet
- Scientific Analysis Goal: Goal:: Subjective CuesDocument3 pagesScientific Analysis Goal: Goal:: Subjective CuesChloie Marie RosalejosNo ratings yet
- Nursing Care Plan2Document3 pagesNursing Care Plan2Fc CrisostomoNo ratings yet
- NCP JourrnallldsdDocument17 pagesNCP JourrnallldsdCHRISTINE JOY. MOLINANo ratings yet
- Principles of Pathophysiology - Bullock, ShaneDocument2 pagesPrinciples of Pathophysiology - Bullock, ShaneMel Izhra N. MargateNo ratings yet
- NCP Rheumatoid FeverDocument6 pagesNCP Rheumatoid FeverJustine CagatanNo ratings yet
- Ccu Cad NCPDocument5 pagesCcu Cad NCPheyyymeeeNo ratings yet
- NCPDocument5 pagesNCPtwinks cabadingNo ratings yet
- Preop Appendectomy NCPDocument3 pagesPreop Appendectomy NCPMyra AtuleNo ratings yet
- Drug Study and NCP (Craniotomy)Document2 pagesDrug Study and NCP (Craniotomy)Deinielle Magdangal Romero100% (1)
- HydrocephalusDocument3 pagesHydrocephalusMae Arra Lecobu-anNo ratings yet
- Adrian G. Mallar BSN 2 Focus: Chest Pain Nursing Care Plan - Rheumatic Heart DiseaseDocument3 pagesAdrian G. Mallar BSN 2 Focus: Chest Pain Nursing Care Plan - Rheumatic Heart DiseaseFarzana AfrinNo ratings yet
- College of Nursing and Allied Medical Sciences: WesleyanDocument3 pagesCollege of Nursing and Allied Medical Sciences: WesleyanPrince Juzzel Banag100% (1)
- NCP SGHDocument2 pagesNCP SGHdaniloabautista44No ratings yet
- NCP SGH DianaDocument2 pagesNCP SGH Dianadaniloabautista44No ratings yet
- Joanne Tomas Skills NCP Pre EclampticDocument3 pagesJoanne Tomas Skills NCP Pre EclampticBSN 3-2 RUIZ, Jewel Anne F.No ratings yet
- Marquez, C. BSN 2B Case Study 104Document5 pagesMarquez, C. BSN 2B Case Study 104Caren MarquezNo ratings yet
- NCP Post Op (Impaired and Risk For Infection)Document4 pagesNCP Post Op (Impaired and Risk For Infection)Carl J.No ratings yet
- NCP BeeaDocument3 pagesNCP BeeaKiko BernardinoNo ratings yet
- Acute Pain!!!!!!!!!!!!!!!Document3 pagesAcute Pain!!!!!!!!!!!!!!!ahz_kerian2No ratings yet
- NCP PostpartumDocument6 pagesNCP PostpartumLovely Anne ArqueroNo ratings yet
- Ii. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Document4 pagesIi. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Lecery Sophia Wong75% (4)
- Nursing Care PlanDocument4 pagesNursing Care PlanChrizelle FlorentinoNo ratings yet
- Fernandez 1b NCPDocument7 pagesFernandez 1b NCPToni Marie FernandezNo ratings yet
- Nursing Care Plan - ProdigalidadDocument5 pagesNursing Care Plan - ProdigalidadZxiayieee JeonNo ratings yet
- Breast Mass Bilateral To Consider FibroadenomaDocument5 pagesBreast Mass Bilateral To Consider FibroadenomaYum CNo ratings yet
- NCP & DSDocument4 pagesNCP & DSKyla Marie TejadaNo ratings yet
- To Decrease Temperature by Means Through Evaporation and ConductionDocument11 pagesTo Decrease Temperature by Means Through Evaporation and Conductioniaekawa100% (6)
- Acute Pain - NCPDocument3 pagesAcute Pain - NCPNovelyn PuaNo ratings yet
- Group-5 - NCP - Ges HypDocument2 pagesGroup-5 - NCP - Ges HypWallen Jey VelascoNo ratings yet
- Medina, Joanna BN3C - NCP FormatDocument7 pagesMedina, Joanna BN3C - NCP FormatJOANNA MARIE MEDINANo ratings yet
- Risk NCP - PESCADERO 4CDocument1 pageRisk NCP - PESCADERO 4COrlando VillanuevaNo ratings yet
- Subjective: " " Sto: Diagnostics: Sto:Goal MET: VitalDocument3 pagesSubjective: " " Sto: Diagnostics: Sto:Goal MET: VitalKarl KiwisNo ratings yet
- NCP UTI (Artillo)Document3 pagesNCP UTI (Artillo)Al TheóNo ratings yet
- NCM 109-NCP - PeregrinoDocument2 pagesNCM 109-NCP - PeregrinoJOYCE ANN PEREGRINONo ratings yet
- NCP Knowledge DeficitDocument2 pagesNCP Knowledge DeficitRainier IbarretaNo ratings yet
- Nursing Care Plan For Myocardial Infarction NCPDocument8 pagesNursing Care Plan For Myocardial Infarction NCPRhomyrose CampanaNo ratings yet
- Fast Facts: Perioperative Pain: Effective management has numerous benefitsFrom EverandFast Facts: Perioperative Pain: Effective management has numerous benefitsNo ratings yet
- Medsurg FinalDocument22 pagesMedsurg FinalPauline AñesNo ratings yet
- Newly Approved Laws (Duterte)Document35 pagesNewly Approved Laws (Duterte)Pauline AñesNo ratings yet
- Finals MS RLEDocument6 pagesFinals MS RLEPauline AñesNo ratings yet
- Drug Study (Hydrocortisone)Document1 pageDrug Study (Hydrocortisone)Pauline AñesNo ratings yet
- Drug StudyDocument3 pagesDrug StudyPauline AñesNo ratings yet
- Skills FCPDocument3 pagesSkills FCPPauline AñesNo ratings yet
- NCM 108 Bioethics - Finals NotesDocument7 pagesNCM 108 Bioethics - Finals NotesPauline AñesNo ratings yet
- Microbiology NotesDocument83 pagesMicrobiology NotesPauline Añes100% (1)
- NCM 107 RLE NotesDocument40 pagesNCM 107 RLE NotesPauline AñesNo ratings yet
- Drug StudyDocument2 pagesDrug StudyPauline AñesNo ratings yet
- Drug StudyDocument3 pagesDrug StudyPauline AñesNo ratings yet
- Case Study 7Document14 pagesCase Study 7Pauline AñesNo ratings yet
- Drug Study Obimin PlusDocument2 pagesDrug Study Obimin PlusPauline AñesNo ratings yet
- Drug Study: Injection May Result inDocument1 pageDrug Study: Injection May Result inPauline AñesNo ratings yet
- Enicillin-Like Antibiotics. Diarrhea, Nausea, Vomiting, HeadacheDocument5 pagesEnicillin-Like Antibiotics. Diarrhea, Nausea, Vomiting, HeadachePauline AñesNo ratings yet
- Man - Has Always Been A Fascinating Organism.: CharityDocument4 pagesMan - Has Always Been A Fascinating Organism.: CharityPauline AñesNo ratings yet
- Cleansing Bed Bath: General ObjectivesDocument3 pagesCleansing Bed Bath: General ObjectivesPauline AñesNo ratings yet
- Case #2 Nursing Care PlanDocument2 pagesCase #2 Nursing Care PlanPauline AñesNo ratings yet
- Marketing StrategiesDocument6 pagesMarketing StrategiesPauline AñesNo ratings yet
- Finals Funda SkillsDocument7 pagesFinals Funda SkillsPauline AñesNo ratings yet
- Health Assessment NotesDocument12 pagesHealth Assessment NotesPauline Añes0% (1)
- Health Assessment SKILLS NOTESDocument9 pagesHealth Assessment SKILLS NOTESPauline AñesNo ratings yet
- The Role of Free Radicals in Health and DiseaseDocument9 pagesThe Role of Free Radicals in Health and Diseasehumera0% (1)
- 1694 1699+Aliyah+PurwantiDocument6 pages1694 1699+Aliyah+Purwantisiti zuhri ramdaniNo ratings yet
- Relapsing Polychondritis - A 2016 Update On Clinical Features, Diagnostic Tools, Treatment and Biological Drug UseDocument18 pagesRelapsing Polychondritis - A 2016 Update On Clinical Features, Diagnostic Tools, Treatment and Biological Drug UseAldiNo ratings yet
- Biology 5090 12 Paper 1 Question Paper Mayjue 2013Document16 pagesBiology 5090 12 Paper 1 Question Paper Mayjue 2013Raja Muda Raja NgahNo ratings yet
- EnzymesDocument13 pagesEnzymesapi-290318217No ratings yet
- The Cardiovascular System: Jomar P. Ronquillo, RN, Manc Anatomy and Physiology InstructorDocument133 pagesThe Cardiovascular System: Jomar P. Ronquillo, RN, Manc Anatomy and Physiology InstructorHypothalamus1No ratings yet
- Upper Limb DopplerDocument35 pagesUpper Limb DopplerRahul Kulkarni100% (1)
- DrugDocument6 pagesDrugRose Ann MirafloresNo ratings yet
- Developing The WHOLE PersonDocument9 pagesDeveloping The WHOLE Persondianne genelzaNo ratings yet
- Cell Structure Gizmo AnswersDocument5 pagesCell Structure Gizmo Answerspaula-navas 13451No ratings yet
- Biology Diagram McqsDocument23 pagesBiology Diagram McqsFatima Obaid0% (1)
- HaematologyDocument11 pagesHaematologyIkram AzmanNo ratings yet
- Elsa Manual SabreDocument50 pagesElsa Manual SabrerijalharunNo ratings yet
- Muscles of Facial Expression: DR Kibe GKDocument32 pagesMuscles of Facial Expression: DR Kibe GKjohn mwambuNo ratings yet
- Keanekaragaman Mikroalga Divisi Cyanobacteria Di Danau Aur Kabupaten Musi RawasDocument7 pagesKeanekaragaman Mikroalga Divisi Cyanobacteria Di Danau Aur Kabupaten Musi RawasRendy Viky HaikalNo ratings yet
- Course Review KeyDocument24 pagesCourse Review KeyHermann Dejero LozanoNo ratings yet
- Psych 150 Final ReviewDocument5 pagesPsych 150 Final ReviewTim WiseNo ratings yet
- Journal-Notes On Cognitive Science (E.g., C. R. Gallistel and Adam Philip King's Important BookDocument13 pagesJournal-Notes On Cognitive Science (E.g., C. R. Gallistel and Adam Philip King's Important Bookappled.apNo ratings yet
- Drug Study On Emergency Drugs Final - )Document12 pagesDrug Study On Emergency Drugs Final - )wen_pil100% (3)
- Chemotherapy and Renal Andhepatic Insufficiency 2008Document24 pagesChemotherapy and Renal Andhepatic Insufficiency 2008Vika RatuNo ratings yet
- Mata Pelajaran: Bahasa Inggris Kelas: Xi/Semua Jurusan: Soal Ulangan Harian Ahir 2021Document11 pagesMata Pelajaran: Bahasa Inggris Kelas: Xi/Semua Jurusan: Soal Ulangan Harian Ahir 2021Ika Septiani PutriNo ratings yet
- Report On Stress - NymaDocument26 pagesReport On Stress - Nymannaima100% (1)
- Introduction To Physiology, Chemical Composition of The BodyDocument42 pagesIntroduction To Physiology, Chemical Composition of The Bodymrskhan jalalNo ratings yet
- La Limpieza HepaticaDocument186 pagesLa Limpieza HepaticaNehomar Jose Brito Guerra100% (5)
- David Berceli Webinar Notes, Trauma Releasing Exercises NotesDocument23 pagesDavid Berceli Webinar Notes, Trauma Releasing Exercises NotesAnonymous F4KmWCH100% (11)
- The Largest Organ of The Body IsDocument10 pagesThe Largest Organ of The Body IsDip Ayan MNo ratings yet
- Final Announcement Book 26th ASMIHA 2017-1Document47 pagesFinal Announcement Book 26th ASMIHA 2017-1d.ramadhanNo ratings yet
- Review and Comprehension P. 108 (Madayag, Rachel Eve G)Document2 pagesReview and Comprehension P. 108 (Madayag, Rachel Eve G)Rachel MadayagNo ratings yet
- Influence of Aerobic Exercise Training On Cardiovascular and Endocrine Inflammatory Biomarkers in Hypertensive Postmenopausal WomenDocument7 pagesInfluence of Aerobic Exercise Training On Cardiovascular and Endocrine Inflammatory Biomarkers in Hypertensive Postmenopausal WomenNemo SecretNo ratings yet











































































































Download as docx, pdf, or txt
You might also like
- Nursing Care Plan For CholecystitisDocument4 pagesNursing Care Plan For CholecystitisEemyaj Jaymee88% (8)
- Nursing Care Plan PDFDocument6 pagesNursing Care Plan PDFEngely MercaderNo ratings yet
- NCP AnginaDocument3 pagesNCP AnginaShie LA100% (1)
- HeliotherapyDocument26 pagesHeliotherapyalmont1759No ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanMariel GamaloNo ratings yet
- Nursing Care Plan Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationDocument4 pagesNursing Care Plan Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationAngelica Charisse BuliganNo ratings yet
- Nursing Care Plan For Myocardial InfarctionDocument7 pagesNursing Care Plan For Myocardial InfarctionRocelyn CristobalNo ratings yet
- Nursing Care Plan For Myocardial InfarctionDocument7 pagesNursing Care Plan For Myocardial InfarctionjamieboyRN88% (8)
- NCP TahbsoDocument18 pagesNCP TahbsoUzziah Dharambai GurbuxaniNo ratings yet
- Perioperative Nursing Care Plan TAHBSODocument4 pagesPerioperative Nursing Care Plan TAHBSOPatricia OrtegaNo ratings yet
- Long Term: PT Will Demonstrate Increased Tolerance To Activity by DischargeDocument18 pagesLong Term: PT Will Demonstrate Increased Tolerance To Activity by DischargeMary Ann Ebol0% (1)
- Erica Marie L. Escanda BSN 3-A Group 2: Hyperthermia Related ToDocument3 pagesErica Marie L. Escanda BSN 3-A Group 2: Hyperthermia Related ToErica Marie EscandaNo ratings yet
- Nursing Care Plan Age: 60 Years OldDocument4 pagesNursing Care Plan Age: 60 Years OldLouise GudmalinNo ratings yet
- ACUTE PAIN BSN III KOLCABA NCP 8th ROTATIONDocument4 pagesACUTE PAIN BSN III KOLCABA NCP 8th ROTATIONKrisheille Amano MirandaNo ratings yet
- NCP FinalDocument10 pagesNCP FinalAlessandro MadrigalNo ratings yet
- NCP Estoesta HemorrhageDocument5 pagesNCP Estoesta HemorrhageKyle Albert EstoestaNo ratings yet
- Case Study Myocardial InfarctionDocument23 pagesCase Study Myocardial InfarctionJester GalayNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Rationale Planning Intervention S Rationale EvaluationDocument7 pagesNursing Care Plan: Assessment Nursing Diagnosis Rationale Planning Intervention S Rationale EvaluationNo EulNo ratings yet
- Nursing Care PlansDocument16 pagesNursing Care PlansJobelle AcenaNo ratings yet
- Nursing Care Plan TemplateDocument5 pagesNursing Care Plan TemplateKyle Albert EstoestaNo ratings yet
- Nursing Care Plan 1Document4 pagesNursing Care Plan 1Kiko BernardinoNo ratings yet
- NCP - BSN12F - Pumbaya (Module 4)Document3 pagesNCP - BSN12F - Pumbaya (Module 4)Ellah PumbayaNo ratings yet
- Scientific Analysis Goal: Goal:: Subjective CuesDocument3 pagesScientific Analysis Goal: Goal:: Subjective CuesChloie Marie RosalejosNo ratings yet
- Nursing Care Plan2Document3 pagesNursing Care Plan2Fc CrisostomoNo ratings yet
- NCP JourrnallldsdDocument17 pagesNCP JourrnallldsdCHRISTINE JOY. MOLINANo ratings yet
- Principles of Pathophysiology - Bullock, ShaneDocument2 pagesPrinciples of Pathophysiology - Bullock, ShaneMel Izhra N. MargateNo ratings yet
- NCP Rheumatoid FeverDocument6 pagesNCP Rheumatoid FeverJustine CagatanNo ratings yet
- Ccu Cad NCPDocument5 pagesCcu Cad NCPheyyymeeeNo ratings yet
- NCPDocument5 pagesNCPtwinks cabadingNo ratings yet
- Preop Appendectomy NCPDocument3 pagesPreop Appendectomy NCPMyra AtuleNo ratings yet
- Drug Study and NCP (Craniotomy)Document2 pagesDrug Study and NCP (Craniotomy)Deinielle Magdangal Romero100% (1)
- HydrocephalusDocument3 pagesHydrocephalusMae Arra Lecobu-anNo ratings yet
- Adrian G. Mallar BSN 2 Focus: Chest Pain Nursing Care Plan - Rheumatic Heart DiseaseDocument3 pagesAdrian G. Mallar BSN 2 Focus: Chest Pain Nursing Care Plan - Rheumatic Heart DiseaseFarzana AfrinNo ratings yet
- College of Nursing and Allied Medical Sciences: WesleyanDocument3 pagesCollege of Nursing and Allied Medical Sciences: WesleyanPrince Juzzel Banag100% (1)
- NCP SGHDocument2 pagesNCP SGHdaniloabautista44No ratings yet
- NCP SGH DianaDocument2 pagesNCP SGH Dianadaniloabautista44No ratings yet
- Joanne Tomas Skills NCP Pre EclampticDocument3 pagesJoanne Tomas Skills NCP Pre EclampticBSN 3-2 RUIZ, Jewel Anne F.No ratings yet
- Marquez, C. BSN 2B Case Study 104Document5 pagesMarquez, C. BSN 2B Case Study 104Caren MarquezNo ratings yet
- NCP Post Op (Impaired and Risk For Infection)Document4 pagesNCP Post Op (Impaired and Risk For Infection)Carl J.No ratings yet
- NCP BeeaDocument3 pagesNCP BeeaKiko BernardinoNo ratings yet
- Acute Pain!!!!!!!!!!!!!!!Document3 pagesAcute Pain!!!!!!!!!!!!!!!ahz_kerian2No ratings yet
- NCP PostpartumDocument6 pagesNCP PostpartumLovely Anne ArqueroNo ratings yet
- Ii. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Document4 pagesIi. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Lecery Sophia Wong75% (4)
- Nursing Care PlanDocument4 pagesNursing Care PlanChrizelle FlorentinoNo ratings yet
- Fernandez 1b NCPDocument7 pagesFernandez 1b NCPToni Marie FernandezNo ratings yet
- Nursing Care Plan - ProdigalidadDocument5 pagesNursing Care Plan - ProdigalidadZxiayieee JeonNo ratings yet
- Breast Mass Bilateral To Consider FibroadenomaDocument5 pagesBreast Mass Bilateral To Consider FibroadenomaYum CNo ratings yet
- NCP & DSDocument4 pagesNCP & DSKyla Marie TejadaNo ratings yet
- To Decrease Temperature by Means Through Evaporation and ConductionDocument11 pagesTo Decrease Temperature by Means Through Evaporation and Conductioniaekawa100% (6)
- Acute Pain - NCPDocument3 pagesAcute Pain - NCPNovelyn PuaNo ratings yet
- Group-5 - NCP - Ges HypDocument2 pagesGroup-5 - NCP - Ges HypWallen Jey VelascoNo ratings yet
- Medina, Joanna BN3C - NCP FormatDocument7 pagesMedina, Joanna BN3C - NCP FormatJOANNA MARIE MEDINANo ratings yet
- Risk NCP - PESCADERO 4CDocument1 pageRisk NCP - PESCADERO 4COrlando VillanuevaNo ratings yet
- Subjective: " " Sto: Diagnostics: Sto:Goal MET: VitalDocument3 pagesSubjective: " " Sto: Diagnostics: Sto:Goal MET: VitalKarl KiwisNo ratings yet
- NCP UTI (Artillo)Document3 pagesNCP UTI (Artillo)Al TheóNo ratings yet
- NCM 109-NCP - PeregrinoDocument2 pagesNCM 109-NCP - PeregrinoJOYCE ANN PEREGRINONo ratings yet
- NCP Knowledge DeficitDocument2 pagesNCP Knowledge DeficitRainier IbarretaNo ratings yet
- Nursing Care Plan For Myocardial Infarction NCPDocument8 pagesNursing Care Plan For Myocardial Infarction NCPRhomyrose CampanaNo ratings yet
- Fast Facts: Perioperative Pain: Effective management has numerous benefitsFrom EverandFast Facts: Perioperative Pain: Effective management has numerous benefitsNo ratings yet
- Medsurg FinalDocument22 pagesMedsurg FinalPauline AñesNo ratings yet
- Newly Approved Laws (Duterte)Document35 pagesNewly Approved Laws (Duterte)Pauline AñesNo ratings yet
- Finals MS RLEDocument6 pagesFinals MS RLEPauline AñesNo ratings yet
- Drug Study (Hydrocortisone)Document1 pageDrug Study (Hydrocortisone)Pauline AñesNo ratings yet
- Drug StudyDocument3 pagesDrug StudyPauline AñesNo ratings yet
- Skills FCPDocument3 pagesSkills FCPPauline AñesNo ratings yet
- NCM 108 Bioethics - Finals NotesDocument7 pagesNCM 108 Bioethics - Finals NotesPauline AñesNo ratings yet
- Microbiology NotesDocument83 pagesMicrobiology NotesPauline Añes100% (1)
- NCM 107 RLE NotesDocument40 pagesNCM 107 RLE NotesPauline AñesNo ratings yet
- Drug StudyDocument2 pagesDrug StudyPauline AñesNo ratings yet
- Drug StudyDocument3 pagesDrug StudyPauline AñesNo ratings yet
- Case Study 7Document14 pagesCase Study 7Pauline AñesNo ratings yet
- Drug Study Obimin PlusDocument2 pagesDrug Study Obimin PlusPauline AñesNo ratings yet
- Drug Study: Injection May Result inDocument1 pageDrug Study: Injection May Result inPauline AñesNo ratings yet
- Enicillin-Like Antibiotics. Diarrhea, Nausea, Vomiting, HeadacheDocument5 pagesEnicillin-Like Antibiotics. Diarrhea, Nausea, Vomiting, HeadachePauline AñesNo ratings yet
- Man - Has Always Been A Fascinating Organism.: CharityDocument4 pagesMan - Has Always Been A Fascinating Organism.: CharityPauline AñesNo ratings yet
- Cleansing Bed Bath: General ObjectivesDocument3 pagesCleansing Bed Bath: General ObjectivesPauline AñesNo ratings yet
- Case #2 Nursing Care PlanDocument2 pagesCase #2 Nursing Care PlanPauline AñesNo ratings yet
- Marketing StrategiesDocument6 pagesMarketing StrategiesPauline AñesNo ratings yet
- Finals Funda SkillsDocument7 pagesFinals Funda SkillsPauline AñesNo ratings yet
- Health Assessment NotesDocument12 pagesHealth Assessment NotesPauline Añes0% (1)
- Health Assessment SKILLS NOTESDocument9 pagesHealth Assessment SKILLS NOTESPauline AñesNo ratings yet
- The Role of Free Radicals in Health and DiseaseDocument9 pagesThe Role of Free Radicals in Health and Diseasehumera0% (1)
- 1694 1699+Aliyah+PurwantiDocument6 pages1694 1699+Aliyah+Purwantisiti zuhri ramdaniNo ratings yet
- Relapsing Polychondritis - A 2016 Update On Clinical Features, Diagnostic Tools, Treatment and Biological Drug UseDocument18 pagesRelapsing Polychondritis - A 2016 Update On Clinical Features, Diagnostic Tools, Treatment and Biological Drug UseAldiNo ratings yet
- Biology 5090 12 Paper 1 Question Paper Mayjue 2013Document16 pagesBiology 5090 12 Paper 1 Question Paper Mayjue 2013Raja Muda Raja NgahNo ratings yet
- EnzymesDocument13 pagesEnzymesapi-290318217No ratings yet
- The Cardiovascular System: Jomar P. Ronquillo, RN, Manc Anatomy and Physiology InstructorDocument133 pagesThe Cardiovascular System: Jomar P. Ronquillo, RN, Manc Anatomy and Physiology InstructorHypothalamus1No ratings yet
- Upper Limb DopplerDocument35 pagesUpper Limb DopplerRahul Kulkarni100% (1)
- DrugDocument6 pagesDrugRose Ann MirafloresNo ratings yet
- Developing The WHOLE PersonDocument9 pagesDeveloping The WHOLE Persondianne genelzaNo ratings yet
- Cell Structure Gizmo AnswersDocument5 pagesCell Structure Gizmo Answerspaula-navas 13451No ratings yet
- Biology Diagram McqsDocument23 pagesBiology Diagram McqsFatima Obaid0% (1)
- HaematologyDocument11 pagesHaematologyIkram AzmanNo ratings yet
- Elsa Manual SabreDocument50 pagesElsa Manual SabrerijalharunNo ratings yet
- Muscles of Facial Expression: DR Kibe GKDocument32 pagesMuscles of Facial Expression: DR Kibe GKjohn mwambuNo ratings yet
- Keanekaragaman Mikroalga Divisi Cyanobacteria Di Danau Aur Kabupaten Musi RawasDocument7 pagesKeanekaragaman Mikroalga Divisi Cyanobacteria Di Danau Aur Kabupaten Musi RawasRendy Viky HaikalNo ratings yet
- Course Review KeyDocument24 pagesCourse Review KeyHermann Dejero LozanoNo ratings yet
- Psych 150 Final ReviewDocument5 pagesPsych 150 Final ReviewTim WiseNo ratings yet
- Journal-Notes On Cognitive Science (E.g., C. R. Gallistel and Adam Philip King's Important BookDocument13 pagesJournal-Notes On Cognitive Science (E.g., C. R. Gallistel and Adam Philip King's Important Bookappled.apNo ratings yet
- Drug Study On Emergency Drugs Final - )Document12 pagesDrug Study On Emergency Drugs Final - )wen_pil100% (3)
- Chemotherapy and Renal Andhepatic Insufficiency 2008Document24 pagesChemotherapy and Renal Andhepatic Insufficiency 2008Vika RatuNo ratings yet
- Mata Pelajaran: Bahasa Inggris Kelas: Xi/Semua Jurusan: Soal Ulangan Harian Ahir 2021Document11 pagesMata Pelajaran: Bahasa Inggris Kelas: Xi/Semua Jurusan: Soal Ulangan Harian Ahir 2021Ika Septiani PutriNo ratings yet
- Report On Stress - NymaDocument26 pagesReport On Stress - Nymannaima100% (1)
- Introduction To Physiology, Chemical Composition of The BodyDocument42 pagesIntroduction To Physiology, Chemical Composition of The Bodymrskhan jalalNo ratings yet
- La Limpieza HepaticaDocument186 pagesLa Limpieza HepaticaNehomar Jose Brito Guerra100% (5)
- David Berceli Webinar Notes, Trauma Releasing Exercises NotesDocument23 pagesDavid Berceli Webinar Notes, Trauma Releasing Exercises NotesAnonymous F4KmWCH100% (11)
- The Largest Organ of The Body IsDocument10 pagesThe Largest Organ of The Body IsDip Ayan MNo ratings yet
- Final Announcement Book 26th ASMIHA 2017-1Document47 pagesFinal Announcement Book 26th ASMIHA 2017-1d.ramadhanNo ratings yet
- Review and Comprehension P. 108 (Madayag, Rachel Eve G)Document2 pagesReview and Comprehension P. 108 (Madayag, Rachel Eve G)Rachel MadayagNo ratings yet
- Influence of Aerobic Exercise Training On Cardiovascular and Endocrine Inflammatory Biomarkers in Hypertensive Postmenopausal WomenDocument7 pagesInfluence of Aerobic Exercise Training On Cardiovascular and Endocrine Inflammatory Biomarkers in Hypertensive Postmenopausal WomenNemo SecretNo ratings yet