
Genitourinary Care Plan: Investigations
Genitourinary Care Plan: Investigations
You might also like
- Child Dental Examination FormDocument1 pageChild Dental Examination FormElok Faiqotul Umma67% (3)
- Acute Gastritis CPG FINALDocument5 pagesAcute Gastritis CPG FINALkimadlo656No ratings yet
- Discharge Plan FormatDocument2 pagesDischarge Plan FormatChristian67% (6)
- Training To See AurasDocument24 pagesTraining To See Auraskflip7593% (15)
- Vaccination Schedule For HorsesDocument3 pagesVaccination Schedule For HorsesKikiNo ratings yet
- Consent Sample For Sexual AbuseDocument8 pagesConsent Sample For Sexual Abuseamarch517No ratings yet
- Facial Clinical HistoryDocument3 pagesFacial Clinical HistoryScribdTranslationsNo ratings yet
- Consent FormsDocument2 pagesConsent FormsKristeline MedelNo ratings yet
- PONR - Comprehensive Nursing Health History and Physical ExaminationDocument21 pagesPONR - Comprehensive Nursing Health History and Physical ExaminationDRJC100% (1)
- Questionnaire Pre Natale HMEDocument8 pagesQuestionnaire Pre Natale HMEKhanza Dzikra AgyaNo ratings yet
- Chnursing NotesDocument21 pagesChnursing Notesjimmy boy canlas jrNo ratings yet
- Procedural Sedation RecordDocument2 pagesProcedural Sedation RecordRosanne AguilarNo ratings yet
- Initial and Annual Health RecordDocument2 pagesInitial and Annual Health Recordmariegold mortola fabelaNo ratings yet
- Max Life Insurance Company LimitedDocument1 pageMax Life Insurance Company LimitedRavindranathNo ratings yet
- Discharge PlanDocument3 pagesDischarge PlanDoneva Lyn MedinaNo ratings yet
- Date: - : (Last) (First) (Middle)Document5 pagesDate: - : (Last) (First) (Middle)KatieNo ratings yet
- Medical Health RecordDocument1 pageMedical Health RecordNikay SerdeñaNo ratings yet
- Consultation and Informed Consent VejDocument7 pagesConsultation and Informed Consent Vejlovrata4550No ratings yet
- Riwayat Klinis WajahDocument3 pagesRiwayat Klinis WajahScribdTranslationsNo ratings yet
- Patient Chart TemplateDocument3 pagesPatient Chart TemplateV NNo ratings yet
- Halitosis QuestionnaireDocument3 pagesHalitosis Questionnairealumera50% (2)
- Master Packing List3 - PDFDocument1 pageMaster Packing List3 - PDFPatricia HNo ratings yet
- Sedation Record: Patient Selection Criteria DateDocument2 pagesSedation Record: Patient Selection Criteria Datenona aryanNo ratings yet
- Pcca Confidential Hormone Evaluation: Medical HistoryDocument5 pagesPcca Confidential Hormone Evaluation: Medical HistoryhaindnxjNo ratings yet
- Circumcision 2-4-09Document2 pagesCircumcision 2-4-09twells417No ratings yet
- Rle Worksheet: Labor Room and Delivery RoomDocument15 pagesRle Worksheet: Labor Room and Delivery RoomLalisaM Activity100% (1)
- Gordon's FormDocument6 pagesGordon's FormHarry AglugobNo ratings yet
- PA Forms FindingsDocument30 pagesPA Forms FindingstmmrsptlnNo ratings yet
- Drug Study 3Document1 pageDrug Study 3Coleen Angelique MontenegroNo ratings yet
- Blood Transfusion Reaction FormDocument2 pagesBlood Transfusion Reaction Formbmci.bongNo ratings yet
- Dental Trauma WorksheetDocument2 pagesDental Trauma WorksheetSteliana CaramanNo ratings yet
- Phone: ( - ) - Fax: ( - ) - : (Company Name) Outpatient Physical Therapy EvaluationDocument2 pagesPhone: ( - ) - Fax: ( - ) - : (Company Name) Outpatient Physical Therapy Evaluationpt.mahmoudNo ratings yet
- Medical Form For Grade 7 12Document3 pagesMedical Form For Grade 7 12Deonna Angeline100% (1)
- Health History Assessment ToolDocument3 pagesHealth History Assessment ToolDaniela Suarez NimNo ratings yet
- Gordons Functional Health Patterns Assessment 1Document11 pagesGordons Functional Health Patterns Assessment 1Katherine Lizell Lopez100% (1)
- Cuidados Posoperatorio CirugiaDocument1 pageCuidados Posoperatorio CirugiaAna CristernaNo ratings yet
- Asessment and Evaluation FormsDocument11 pagesAsessment and Evaluation FormsJU DYNo ratings yet
- History Guide Ob GyneDocument5 pagesHistory Guide Ob Gyned99452727No ratings yet
- ISO 05 Student Health Record 1 RevDocument2 pagesISO 05 Student Health Record 1 RevHahaha HihihooNo ratings yet
- 2019-ShadowerObserver-Application 191003 195038Document9 pages2019-ShadowerObserver-Application 191003 195038omer khanNo ratings yet
- Clinical Pathway For Hypertensive Urgency (Revised)Document6 pagesClinical Pathway For Hypertensive Urgency (Revised)Heide Danica A. BaltazarNo ratings yet
- EHS-Net Foodborne Illness Complaint FormDocument4 pagesEHS-Net Foodborne Illness Complaint Formsimiprince80No ratings yet
- 8.) Health-and-Medical-Profile Template Ver.2Document4 pages8.) Health-and-Medical-Profile Template Ver.2SocialWelfare SilangNo ratings yet
- MED-F-009 Discharge Planning FormDocument1 pageMED-F-009 Discharge Planning Formdrakmalik71No ratings yet
- Obstetric FormDocument4 pagesObstetric FormKhylamarie VillalunaNo ratings yet
- MediSpa Intake FormsDocument9 pagesMediSpa Intake FormsUtopiaawaitsNo ratings yet
- 2018 WSRDocument1 page2018 WSR2ncnz6999mNo ratings yet
- Kidney and Urinary Disorder QuestionnaireDocument2 pagesKidney and Urinary Disorder Questionnairejeevan820No ratings yet
- Consent For Medications 2011Document1 pageConsent For Medications 2011maconjanice222No ratings yet
- Referral SourceDocument10 pagesReferral SourceHumberto FuentesNo ratings yet
- Documentation FormDocument2 pagesDocumentation FormAlya Al DihainiNo ratings yet
- FORMAT Pengkajian Bahasa InggrisDocument13 pagesFORMAT Pengkajian Bahasa InggrisMadiinaaftNo ratings yet
- Breast Cancer Assessment ChartDocument2 pagesBreast Cancer Assessment ChartNigel Leigh Godfrey GutierrezNo ratings yet
- ANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientDocument5 pagesANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientjackydoodsonNo ratings yet
- Gordon S Functional Health Pattern Assessment ToolDocument10 pagesGordon S Functional Health Pattern Assessment ToolMiguel VicenteNo ratings yet
- CovidreportformDocument1 pageCovidreportformapi-460314063No ratings yet
- Vaccination Record InglesDocument1 pageVaccination Record Inglescidaparecida141977No ratings yet
- Revised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)Document3 pagesRevised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)Lindo Gondales Jr.No ratings yet
- Med HX and PE Wards FormDocument8 pagesMed HX and PE Wards FormFMDCNo ratings yet
- Governmental Traumatizing Investigations: An Application to Get a New Toilet, Part IFrom EverandGovernmental Traumatizing Investigations: An Application to Get a New Toilet, Part INo ratings yet
- RMA Skill Practice: Registered Medical Assistant Practice Test QuestionsFrom EverandRMA Skill Practice: Registered Medical Assistant Practice Test QuestionsNo ratings yet
- 3 - Nursing Guide For Evidence and IndicatorsDocument18 pages3 - Nursing Guide For Evidence and IndicatorsOlaya alghareniNo ratings yet
- MHS CL Pci Form 027 Homevisit Checklist and ReportDocument3 pagesMHS CL Pci Form 027 Homevisit Checklist and ReportOlaya alghareniNo ratings yet
- Call Center Job Duties and ResponsibilitiesDocument2 pagesCall Center Job Duties and ResponsibilitiesOlaya alghareniNo ratings yet
- Key Performance Indicator Description: Nursing Care Kpis (1/2)Document4 pagesKey Performance Indicator Description: Nursing Care Kpis (1/2)Olaya alghareniNo ratings yet
- The Caregiver Training CurriculumDocument10 pagesThe Caregiver Training CurriculumOlaya alghareniNo ratings yet
- A P H B H C S H H A O C: Labama Ublic Ealth Ureau of Ome and Ommunity Ervices OME Ealth IDE Rientation HecklistDocument2 pagesA P H B H C S H H A O C: Labama Ublic Ealth Ureau of Ome and Ommunity Ervices OME Ealth IDE Rientation HecklistOlaya alghareniNo ratings yet
- Hha ExamDocument8 pagesHha ExamOlaya alghareniNo ratings yet
- Safety of Dairy Products Webinar ContentDocument24 pagesSafety of Dairy Products Webinar ContentSutha Tamil NambeNo ratings yet
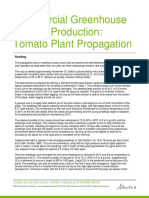
- Commercial Greenhouse Tomato Production: Tomato Plant PropagationDocument20 pagesCommercial Greenhouse Tomato Production: Tomato Plant PropagationSethNo ratings yet
- Maternal Physiology: Metabolic Changes Hematological ChangesDocument33 pagesMaternal Physiology: Metabolic Changes Hematological ChangesironNo ratings yet
- Delgado Guay (2015)Document7 pagesDelgado Guay (2015)Aprilla Ayu WulandariNo ratings yet
- CAMBRA: Best Practices in Dental Caries Management: 3 CE CreditsDocument8 pagesCAMBRA: Best Practices in Dental Caries Management: 3 CE CreditsDino MainoNo ratings yet
- Teaching Plan On Breast CancerDocument6 pagesTeaching Plan On Breast CancerSteph YapNo ratings yet
- Case Study On Wound HealingDocument5 pagesCase Study On Wound HealingINSANE LEO GAMINGNo ratings yet
- EU Fundamentals 7thed Sample ChapterDocument12 pagesEU Fundamentals 7thed Sample ChapterAndrada ArmasuNo ratings yet
- Bacillus Coagulans Probiotic of Choice Nutracos March April 2012Document3 pagesBacillus Coagulans Probiotic of Choice Nutracos March April 2012Gabriel ManriquezNo ratings yet
- Nursing Care PlanDocument10 pagesNursing Care PlanIsabelle Madrid100% (1)
- Herbs in Periodontal DiseaseDocument5 pagesHerbs in Periodontal DiseaseNadhilahNo ratings yet
- World Obesity Atlas 2023 ReportDocument232 pagesWorld Obesity Atlas 2023 ReportVozMediaNo ratings yet
- Government Policy and People Attitudes Towards Covid-19 Mitigation Strategies in Calabar Municipality, Cross River State - NigeriaDocument7 pagesGovernment Policy and People Attitudes Towards Covid-19 Mitigation Strategies in Calabar Municipality, Cross River State - NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 4 1 1 Student Response Sheet Pathblood (Revised 2 2 15)Document5 pages4 1 1 Student Response Sheet Pathblood (Revised 2 2 15)api-281824634No ratings yet
- NCM 116 Lect Visual PerceptionDocument45 pagesNCM 116 Lect Visual PerceptionMariano MarbellaNo ratings yet
- Mustard Rapeseed Profile PDFDocument70 pagesMustard Rapeseed Profile PDFVatsal GadhiaNo ratings yet
- Ascending CholangitisDocument7 pagesAscending CholangitisAmar HasanNo ratings yet
- 7) Preventive Health and EPIDocument51 pages7) Preventive Health and EPIDr. Zirwa AsimNo ratings yet
- HandbookDocument225 pagesHandbookArdoni SaharilNo ratings yet
- NCMB316: Compilation Finals in NCMB316Document23 pagesNCMB316: Compilation Finals in NCMB316Armand Bong Santiago100% (1)
- ARDSDocument26 pagesARDSDuratul FahliaNo ratings yet
- Rosalina Q. de Sagun, M.D. Maria Antonia Aurora Moral - Valencia, M.DDocument52 pagesRosalina Q. de Sagun, M.D. Maria Antonia Aurora Moral - Valencia, M.DDaphne Jo ValmonteNo ratings yet
- Varicose Veins: Dr. Yonas G. (MD)Document18 pagesVaricose Veins: Dr. Yonas G. (MD)Mikiale kirosNo ratings yet
- Somatic UmbrellaDocument10 pagesSomatic UmbrellaYiomarie Ojeda-Rodz100% (1)
- NCP - DENGUE Meg Raven AlvezDocument2 pagesNCP - DENGUE Meg Raven AlvezIngrid Sasha FongNo ratings yet
- Antifilm Activity of PlantsDocument7 pagesAntifilm Activity of PlantsArshia NazirNo ratings yet
- Pudina MintDocument10 pagesPudina MintjunaidNo ratings yet
- Cardiac Catheterization - Post ProcedureDocument2 pagesCardiac Catheterization - Post ProcedureHendi Refiaguna100% (1)































































































Download as docx, pdf, or txt
You might also like
- Child Dental Examination FormDocument1 pageChild Dental Examination FormElok Faiqotul Umma67% (3)
- Acute Gastritis CPG FINALDocument5 pagesAcute Gastritis CPG FINALkimadlo656No ratings yet
- Discharge Plan FormatDocument2 pagesDischarge Plan FormatChristian67% (6)
- Training To See AurasDocument24 pagesTraining To See Auraskflip7593% (15)
- Vaccination Schedule For HorsesDocument3 pagesVaccination Schedule For HorsesKikiNo ratings yet
- Consent Sample For Sexual AbuseDocument8 pagesConsent Sample For Sexual Abuseamarch517No ratings yet
- Facial Clinical HistoryDocument3 pagesFacial Clinical HistoryScribdTranslationsNo ratings yet
- Consent FormsDocument2 pagesConsent FormsKristeline MedelNo ratings yet
- PONR - Comprehensive Nursing Health History and Physical ExaminationDocument21 pagesPONR - Comprehensive Nursing Health History and Physical ExaminationDRJC100% (1)
- Questionnaire Pre Natale HMEDocument8 pagesQuestionnaire Pre Natale HMEKhanza Dzikra AgyaNo ratings yet
- Chnursing NotesDocument21 pagesChnursing Notesjimmy boy canlas jrNo ratings yet
- Procedural Sedation RecordDocument2 pagesProcedural Sedation RecordRosanne AguilarNo ratings yet
- Initial and Annual Health RecordDocument2 pagesInitial and Annual Health Recordmariegold mortola fabelaNo ratings yet
- Max Life Insurance Company LimitedDocument1 pageMax Life Insurance Company LimitedRavindranathNo ratings yet
- Discharge PlanDocument3 pagesDischarge PlanDoneva Lyn MedinaNo ratings yet
- Date: - : (Last) (First) (Middle)Document5 pagesDate: - : (Last) (First) (Middle)KatieNo ratings yet
- Medical Health RecordDocument1 pageMedical Health RecordNikay SerdeñaNo ratings yet
- Consultation and Informed Consent VejDocument7 pagesConsultation and Informed Consent Vejlovrata4550No ratings yet
- Riwayat Klinis WajahDocument3 pagesRiwayat Klinis WajahScribdTranslationsNo ratings yet
- Patient Chart TemplateDocument3 pagesPatient Chart TemplateV NNo ratings yet
- Halitosis QuestionnaireDocument3 pagesHalitosis Questionnairealumera50% (2)
- Master Packing List3 - PDFDocument1 pageMaster Packing List3 - PDFPatricia HNo ratings yet
- Sedation Record: Patient Selection Criteria DateDocument2 pagesSedation Record: Patient Selection Criteria Datenona aryanNo ratings yet
- Pcca Confidential Hormone Evaluation: Medical HistoryDocument5 pagesPcca Confidential Hormone Evaluation: Medical HistoryhaindnxjNo ratings yet
- Circumcision 2-4-09Document2 pagesCircumcision 2-4-09twells417No ratings yet
- Rle Worksheet: Labor Room and Delivery RoomDocument15 pagesRle Worksheet: Labor Room and Delivery RoomLalisaM Activity100% (1)
- Gordon's FormDocument6 pagesGordon's FormHarry AglugobNo ratings yet
- PA Forms FindingsDocument30 pagesPA Forms FindingstmmrsptlnNo ratings yet
- Drug Study 3Document1 pageDrug Study 3Coleen Angelique MontenegroNo ratings yet
- Blood Transfusion Reaction FormDocument2 pagesBlood Transfusion Reaction Formbmci.bongNo ratings yet
- Dental Trauma WorksheetDocument2 pagesDental Trauma WorksheetSteliana CaramanNo ratings yet
- Phone: ( - ) - Fax: ( - ) - : (Company Name) Outpatient Physical Therapy EvaluationDocument2 pagesPhone: ( - ) - Fax: ( - ) - : (Company Name) Outpatient Physical Therapy Evaluationpt.mahmoudNo ratings yet
- Medical Form For Grade 7 12Document3 pagesMedical Form For Grade 7 12Deonna Angeline100% (1)
- Health History Assessment ToolDocument3 pagesHealth History Assessment ToolDaniela Suarez NimNo ratings yet
- Gordons Functional Health Patterns Assessment 1Document11 pagesGordons Functional Health Patterns Assessment 1Katherine Lizell Lopez100% (1)
- Cuidados Posoperatorio CirugiaDocument1 pageCuidados Posoperatorio CirugiaAna CristernaNo ratings yet
- Asessment and Evaluation FormsDocument11 pagesAsessment and Evaluation FormsJU DYNo ratings yet
- History Guide Ob GyneDocument5 pagesHistory Guide Ob Gyned99452727No ratings yet
- ISO 05 Student Health Record 1 RevDocument2 pagesISO 05 Student Health Record 1 RevHahaha HihihooNo ratings yet
- 2019-ShadowerObserver-Application 191003 195038Document9 pages2019-ShadowerObserver-Application 191003 195038omer khanNo ratings yet
- Clinical Pathway For Hypertensive Urgency (Revised)Document6 pagesClinical Pathway For Hypertensive Urgency (Revised)Heide Danica A. BaltazarNo ratings yet
- EHS-Net Foodborne Illness Complaint FormDocument4 pagesEHS-Net Foodborne Illness Complaint Formsimiprince80No ratings yet
- 8.) Health-and-Medical-Profile Template Ver.2Document4 pages8.) Health-and-Medical-Profile Template Ver.2SocialWelfare SilangNo ratings yet
- MED-F-009 Discharge Planning FormDocument1 pageMED-F-009 Discharge Planning Formdrakmalik71No ratings yet
- Obstetric FormDocument4 pagesObstetric FormKhylamarie VillalunaNo ratings yet
- MediSpa Intake FormsDocument9 pagesMediSpa Intake FormsUtopiaawaitsNo ratings yet
- 2018 WSRDocument1 page2018 WSR2ncnz6999mNo ratings yet
- Kidney and Urinary Disorder QuestionnaireDocument2 pagesKidney and Urinary Disorder Questionnairejeevan820No ratings yet
- Consent For Medications 2011Document1 pageConsent For Medications 2011maconjanice222No ratings yet
- Referral SourceDocument10 pagesReferral SourceHumberto FuentesNo ratings yet
- Documentation FormDocument2 pagesDocumentation FormAlya Al DihainiNo ratings yet
- FORMAT Pengkajian Bahasa InggrisDocument13 pagesFORMAT Pengkajian Bahasa InggrisMadiinaaftNo ratings yet
- Breast Cancer Assessment ChartDocument2 pagesBreast Cancer Assessment ChartNigel Leigh Godfrey GutierrezNo ratings yet
- ANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientDocument5 pagesANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientjackydoodsonNo ratings yet
- Gordon S Functional Health Pattern Assessment ToolDocument10 pagesGordon S Functional Health Pattern Assessment ToolMiguel VicenteNo ratings yet
- CovidreportformDocument1 pageCovidreportformapi-460314063No ratings yet
- Vaccination Record InglesDocument1 pageVaccination Record Inglescidaparecida141977No ratings yet
- Revised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)Document3 pagesRevised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)Lindo Gondales Jr.No ratings yet
- Med HX and PE Wards FormDocument8 pagesMed HX and PE Wards FormFMDCNo ratings yet
- Governmental Traumatizing Investigations: An Application to Get a New Toilet, Part IFrom EverandGovernmental Traumatizing Investigations: An Application to Get a New Toilet, Part INo ratings yet
- RMA Skill Practice: Registered Medical Assistant Practice Test QuestionsFrom EverandRMA Skill Practice: Registered Medical Assistant Practice Test QuestionsNo ratings yet
- 3 - Nursing Guide For Evidence and IndicatorsDocument18 pages3 - Nursing Guide For Evidence and IndicatorsOlaya alghareniNo ratings yet
- MHS CL Pci Form 027 Homevisit Checklist and ReportDocument3 pagesMHS CL Pci Form 027 Homevisit Checklist and ReportOlaya alghareniNo ratings yet
- Call Center Job Duties and ResponsibilitiesDocument2 pagesCall Center Job Duties and ResponsibilitiesOlaya alghareniNo ratings yet
- Key Performance Indicator Description: Nursing Care Kpis (1/2)Document4 pagesKey Performance Indicator Description: Nursing Care Kpis (1/2)Olaya alghareniNo ratings yet
- The Caregiver Training CurriculumDocument10 pagesThe Caregiver Training CurriculumOlaya alghareniNo ratings yet
- A P H B H C S H H A O C: Labama Ublic Ealth Ureau of Ome and Ommunity Ervices OME Ealth IDE Rientation HecklistDocument2 pagesA P H B H C S H H A O C: Labama Ublic Ealth Ureau of Ome and Ommunity Ervices OME Ealth IDE Rientation HecklistOlaya alghareniNo ratings yet
- Hha ExamDocument8 pagesHha ExamOlaya alghareniNo ratings yet
- Safety of Dairy Products Webinar ContentDocument24 pagesSafety of Dairy Products Webinar ContentSutha Tamil NambeNo ratings yet
- Commercial Greenhouse Tomato Production: Tomato Plant PropagationDocument20 pagesCommercial Greenhouse Tomato Production: Tomato Plant PropagationSethNo ratings yet
- Maternal Physiology: Metabolic Changes Hematological ChangesDocument33 pagesMaternal Physiology: Metabolic Changes Hematological ChangesironNo ratings yet
- Delgado Guay (2015)Document7 pagesDelgado Guay (2015)Aprilla Ayu WulandariNo ratings yet
- CAMBRA: Best Practices in Dental Caries Management: 3 CE CreditsDocument8 pagesCAMBRA: Best Practices in Dental Caries Management: 3 CE CreditsDino MainoNo ratings yet
- Teaching Plan On Breast CancerDocument6 pagesTeaching Plan On Breast CancerSteph YapNo ratings yet
- Case Study On Wound HealingDocument5 pagesCase Study On Wound HealingINSANE LEO GAMINGNo ratings yet
- EU Fundamentals 7thed Sample ChapterDocument12 pagesEU Fundamentals 7thed Sample ChapterAndrada ArmasuNo ratings yet
- Bacillus Coagulans Probiotic of Choice Nutracos March April 2012Document3 pagesBacillus Coagulans Probiotic of Choice Nutracos March April 2012Gabriel ManriquezNo ratings yet
- Nursing Care PlanDocument10 pagesNursing Care PlanIsabelle Madrid100% (1)
- Herbs in Periodontal DiseaseDocument5 pagesHerbs in Periodontal DiseaseNadhilahNo ratings yet
- World Obesity Atlas 2023 ReportDocument232 pagesWorld Obesity Atlas 2023 ReportVozMediaNo ratings yet
- Government Policy and People Attitudes Towards Covid-19 Mitigation Strategies in Calabar Municipality, Cross River State - NigeriaDocument7 pagesGovernment Policy and People Attitudes Towards Covid-19 Mitigation Strategies in Calabar Municipality, Cross River State - NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 4 1 1 Student Response Sheet Pathblood (Revised 2 2 15)Document5 pages4 1 1 Student Response Sheet Pathblood (Revised 2 2 15)api-281824634No ratings yet
- NCM 116 Lect Visual PerceptionDocument45 pagesNCM 116 Lect Visual PerceptionMariano MarbellaNo ratings yet
- Mustard Rapeseed Profile PDFDocument70 pagesMustard Rapeseed Profile PDFVatsal GadhiaNo ratings yet
- Ascending CholangitisDocument7 pagesAscending CholangitisAmar HasanNo ratings yet
- 7) Preventive Health and EPIDocument51 pages7) Preventive Health and EPIDr. Zirwa AsimNo ratings yet
- HandbookDocument225 pagesHandbookArdoni SaharilNo ratings yet
- NCMB316: Compilation Finals in NCMB316Document23 pagesNCMB316: Compilation Finals in NCMB316Armand Bong Santiago100% (1)
- ARDSDocument26 pagesARDSDuratul FahliaNo ratings yet
- Rosalina Q. de Sagun, M.D. Maria Antonia Aurora Moral - Valencia, M.DDocument52 pagesRosalina Q. de Sagun, M.D. Maria Antonia Aurora Moral - Valencia, M.DDaphne Jo ValmonteNo ratings yet
- Varicose Veins: Dr. Yonas G. (MD)Document18 pagesVaricose Veins: Dr. Yonas G. (MD)Mikiale kirosNo ratings yet
- Somatic UmbrellaDocument10 pagesSomatic UmbrellaYiomarie Ojeda-Rodz100% (1)
- NCP - DENGUE Meg Raven AlvezDocument2 pagesNCP - DENGUE Meg Raven AlvezIngrid Sasha FongNo ratings yet
- Antifilm Activity of PlantsDocument7 pagesAntifilm Activity of PlantsArshia NazirNo ratings yet
- Pudina MintDocument10 pagesPudina MintjunaidNo ratings yet
- Cardiac Catheterization - Post ProcedureDocument2 pagesCardiac Catheterization - Post ProcedureHendi Refiaguna100% (1)