Download as pdf or txt
You might also like
- Pain AssessmentDocument2 pagesPain Assessmentانور الحاجNo ratings yet
- Assessing Pain: The Fifth Vital SignDocument58 pagesAssessing Pain: The Fifth Vital SignErica GyeolsilNo ratings yet
- Pain Management TechniquesDocument22 pagesPain Management Techniques9tmj9b22xvNo ratings yet
- Psycho-Social Aspects of Pain-1Document29 pagesPsycho-Social Aspects of Pain-1nugraha sultanNo ratings yet
- Final - Pain ManagementDocument18 pagesFinal - Pain ManagementFatma Shnewra100% (2)
- Week 3 NotesDocument18 pagesWeek 3 NotesAlvia MagnoNo ratings yet
- Pain Management For Medical StudentsDocument37 pagesPain Management For Medical Studentsamq aloqiliNo ratings yet
- Lecture 1 Fundamentals of Pain ManagementDocument23 pagesLecture 1 Fundamentals of Pain Managementkennedycm4No ratings yet
- Pain Sessment: Pain in The Cognitively ImpairedDocument43 pagesPain Sessment: Pain in The Cognitively Impairedalya1alya1No ratings yet
- Silvanus Chakra Puspita: Medical Staff of Mayapada Hospital Jakarta SelatanDocument44 pagesSilvanus Chakra Puspita: Medical Staff of Mayapada Hospital Jakarta Selatanroby yuliandaNo ratings yet
- Acute Pain (Nyeri Akut)Document8 pagesAcute Pain (Nyeri Akut)Eki MegaraniNo ratings yet
- PainDocument14 pagesPainAmer Abdulla SachitNo ratings yet
- Unit 5 PainDocument133 pagesUnit 5 Painnoo.wannNo ratings yet
- Clinical Care Plan Assignment-HeadacheDocument5 pagesClinical Care Plan Assignment-Headacheafeefahalli5No ratings yet
- Pain AssessmentDocument43 pagesPain AssessmentJalajarani AridassNo ratings yet
- Acute Pain Nursing Diagnosis & Care Plans - NurseTogetherDocument22 pagesAcute Pain Nursing Diagnosis & Care Plans - NurseTogetherrachealakusukNo ratings yet
- Pain Management in The Emergency: Dr. Prathiba Prasad Emergency Physician Masafi HospitalDocument50 pagesPain Management in The Emergency: Dr. Prathiba Prasad Emergency Physician Masafi HospitalPrathiba PrassaddNo ratings yet
- Unit 14 - PainDocument20 pagesUnit 14 - Paindhruvikprajapati2006No ratings yet
- Curs 3 - Durerea La Persoanele in Varsta Institutionalizate LTCDocument30 pagesCurs 3 - Durerea La Persoanele in Varsta Institutionalizate LTCPop AndreiNo ratings yet
- Pain ManagementDocument18 pagesPain ManagementEimhie Lee CasiNo ratings yet
- Palliative Care and Pain Management in AnesthesiaDocument48 pagesPalliative Care and Pain Management in AnesthesiaHammy LizerNo ratings yet
- 3 +Pain+2018+PDF+1ppDocument33 pages3 +Pain+2018+PDF+1pphorace_linNo ratings yet
- Pain and Pain ManagementDocument7 pagesPain and Pain ManagementNatukunda DianahNo ratings yet
- Pathway For Pain Perception and Response: What Is ??Document6 pagesPathway For Pain Perception and Response: What Is ??Jc MendiolaNo ratings yet
- Grieve and LossDocument6 pagesGrieve and LossRuffy AbdulazisNo ratings yet
- Chronic Pain and PsychologyDocument3 pagesChronic Pain and PsychologyOluwafemi OlarindeNo ratings yet
- Acute PainDocument3 pagesAcute PainTyisha CharlesNo ratings yet
- Pain Sessment: Pain in The Cognitively ImpairedDocument43 pagesPain Sessment: Pain in The Cognitively ImpairedJalajarani AridassNo ratings yet
- PainDocument90 pagesPainmikErlh100% (4)
- Ot in Rehab PPT 2Document37 pagesOt in Rehab PPT 2Aarthi ArumugamNo ratings yet
- Pain ManagementDocument40 pagesPain ManagementPutra Pratama100% (1)
- Materi Pain AssesmentDocument4 pagesMateri Pain AssesmentMalini MaliniNo ratings yet
- Lab Manual Assessing Pain Pg. 51 52Document7 pagesLab Manual Assessing Pain Pg. 51 52Joyce JaysonNo ratings yet
- PainDocument90 pagesPainTobiDaNo ratings yet
- Pain Below The Ribs Treatment GuideDocument9 pagesPain Below The Ribs Treatment GuidepaulartistdingleNo ratings yet
- Pain in Children: Ikeu NurhidayahDocument52 pagesPain in Children: Ikeu NurhidayahBURHAN NURDINNo ratings yet
- PNS Pain Management Guideline For Nursing CompetencyDocument10 pagesPNS Pain Management Guideline For Nursing Competencyvhon100% (1)
- Pain and Pain Assessment in Palliative Care 1Document29 pagesPain and Pain Assessment in Palliative Care 1Disala RanaweeraNo ratings yet
- 2009 Pain Assessment and ManagementDocument22 pages2009 Pain Assessment and ManagementErnawa RikaNo ratings yet
- NCP Nursing DiagnosisDocument24 pagesNCP Nursing Diagnosisphvega06No ratings yet
- Pain ManagementDocument162 pagesPain ManagementFASIKAW GIZAWNo ratings yet
- Pain Management - 03-07 VersionDocument51 pagesPain Management - 03-07 VersionanreilegardeNo ratings yet
- Unit II-3. PainDocument42 pagesUnit II-3. PainFikir EsheteNo ratings yet
- Pain Management MFMDocument40 pagesPain Management MFMTamaChanPerawatGokilNo ratings yet
- Comfort Therapy CaringDocument30 pagesComfort Therapy Caringapi-652914452No ratings yet
- Pain Assessment and Management: Lecturer: Sharon A. Guillo Date: TimeDocument31 pagesPain Assessment and Management: Lecturer: Sharon A. Guillo Date: Timesharon alvarezNo ratings yet
- Lesson 2Document8 pagesLesson 2Random RandomNo ratings yet
- Acute Pain Nursing DiagnosisDocument5 pagesAcute Pain Nursing DiagnosisAngelo Cuaresma0% (1)
- Pain ManagementDocument5 pagesPain ManagementWanZack Wan ZaharinNo ratings yet
- PQRST Pain Assessment MethodDocument2 pagesPQRST Pain Assessment MethodKryza Dale Bunado Batican100% (2)
- TonsillectomyDocument50 pagesTonsillectomyChikinPhukkoNo ratings yet
- Konsep Nyeri Dan Manajemen NyeriDocument36 pagesKonsep Nyeri Dan Manajemen NyeriFira AlumanNo ratings yet
- Pain LectureDocument13 pagesPain LectureDale BuckmanNo ratings yet
- PainDocument35 pagesPainixora n100% (1)
- Nursing Intervention of PainDocument3 pagesNursing Intervention of PainRezhaNo ratings yet
- The Art of Holistic Pain Management: A Practical HandbookFrom EverandThe Art of Holistic Pain Management: A Practical HandbookNo ratings yet
- Pain ManagementDocument11 pagesPain Managementenam professorNo ratings yet
- Holistic Pain Relief: How to ease muscles, joints and other painful conditionsFrom EverandHolistic Pain Relief: How to ease muscles, joints and other painful conditionsNo ratings yet
- Pyrolysis of Plastic Waste - Opportunities and ChallengesDocument17 pagesPyrolysis of Plastic Waste - Opportunities and Challengesgavin meadeNo ratings yet
- Tatalaksana Gizi BurukDocument80 pagesTatalaksana Gizi BurukIntania FadillaNo ratings yet
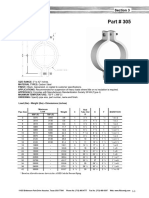
- Part 305 Heavy Pipe ClampDocument1 pagePart 305 Heavy Pipe ClampezhiljananiNo ratings yet
- Fundamentals in Computer Investigations - General Digital ForensicsDocument60 pagesFundamentals in Computer Investigations - General Digital ForensicsMick YoNo ratings yet
- CPL EbrochureDocument4 pagesCPL EbrochureAnuj_WNo ratings yet
- Angel Baby LyricsDocument1 pageAngel Baby LyricsBianca Mongaya100% (1)
- OBIEE Technical Check-ListDocument6 pagesOBIEE Technical Check-ListKrista SmithNo ratings yet
- Semantic Segmentation Data Labelling: Classes and InstructionsDocument9 pagesSemantic Segmentation Data Labelling: Classes and InstructionsMar FieldsNo ratings yet
- Barangay Health Worker Registration FormDocument1 pageBarangay Health Worker Registration FormJairah Marie100% (2)
- Craig Pirrong-Commodity Price Dynamics - A Structural Approach-Cambridge University Press (2011) PDFDocument239 pagesCraig Pirrong-Commodity Price Dynamics - A Structural Approach-Cambridge University Press (2011) PDFchengadNo ratings yet
- Data Mining Assignment HelpDocument5 pagesData Mining Assignment HelpStatistics Homework SolverNo ratings yet
- ChalukyanDocument44 pagesChalukyannimisha jainNo ratings yet
- QuickRide LogcatDocument179 pagesQuickRide Logcatap131096No ratings yet
- Carnot Cycle - Working Principle & Processes With (PV - Ts Diagram)Document8 pagesCarnot Cycle - Working Principle & Processes With (PV - Ts Diagram)Sharif Muhammad HossainNo ratings yet
- 360 Degree Peer Evaluation FormDocument4 pages360 Degree Peer Evaluation FormAjisafe Jerry T-money100% (1)
- Abdellatif Kashkoush SMDocument5 pagesAbdellatif Kashkoush SMRacha BadrNo ratings yet
- Scanfrost Washing Machine ManualDocument5 pagesScanfrost Washing Machine ManualAbdulAzeez ADEBAYONo ratings yet
- Mass Intention Request FormDocument1 pageMass Intention Request FormsergioNo ratings yet
- Branches of Medicine & Wards and Departements - EditkuDocument31 pagesBranches of Medicine & Wards and Departements - EditkuGigih Sanjaya PutraNo ratings yet
- Lesson 7 Protection For Estaurieas and Intertidal ZoneDocument15 pagesLesson 7 Protection For Estaurieas and Intertidal ZoneTeacher JoanNo ratings yet
- Terms and Conditions - Deposit BonusDocument4 pagesTerms and Conditions - Deposit BonusNorakmal Andika YusriNo ratings yet
- Neo FuturismDocument16 pagesNeo Futurismboddutilak100% (1)
- CH 2 - Guide To Physics PracticalsDocument20 pagesCH 2 - Guide To Physics PracticalsNong Hm100% (2)
- South Bend SB1002 Lathe Owners ManualDocument84 pagesSouth Bend SB1002 Lathe Owners ManualRendab100% (2)
- Weekly Meal Planner TemplateDocument11 pagesWeekly Meal Planner TemplateAshok JagtapNo ratings yet
- Ch04 6e Slutions HoyleDocument44 pagesCh04 6e Slutions HoyleJackie PerezNo ratings yet
- Unit Iv Linear Block Codes: Channel EncoderDocument26 pagesUnit Iv Linear Block Codes: Channel EncoderSudhaNo ratings yet
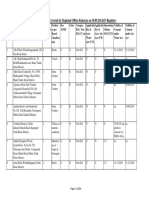
- List of Organisations Covered by Regional Office-Kolar (As On 30.09.2014) (F-Register)Document284 pagesList of Organisations Covered by Regional Office-Kolar (As On 30.09.2014) (F-Register)mutton moonswamiNo ratings yet
- Personal Details: SRM Institute of Science and TechnologyDocument2 pagesPersonal Details: SRM Institute of Science and TechnologyZenelNo ratings yet
- TDS - Emaco R907 PlusDocument2 pagesTDS - Emaco R907 PlusVenkata RaoNo ratings yet