Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ieee C37.20.3-2013Document70 pagesIeee C37.20.3-2013damaso taracena100% (2)
- Polymer Degradation and Stability: Long Yan, Zhisheng Xu, Nan DengDocument13 pagesPolymer Degradation and Stability: Long Yan, Zhisheng Xu, Nan DengEkansh ChoudharyNo ratings yet
- Demosthenes, Speeches 1-17Document364 pagesDemosthenes, Speeches 1-17silviudx100% (1)
- Observations vs. Inferences: "You Can Observe A Lot Just by Watching."Document18 pagesObservations vs. Inferences: "You Can Observe A Lot Just by Watching."Teresita CamachoNo ratings yet
- Liquid in Glass ThermometerDocument21 pagesLiquid in Glass Thermometerkamyar farsNo ratings yet
- LinguisticsDocument5 pagesLinguisticsOumniaNo ratings yet
- PROBLEMSDocument6 pagesPROBLEMSSaranya GunasekarNo ratings yet
- Java Lab (Mca) SyllabusDocument2 pagesJava Lab (Mca) SyllabusAMAN PANDEY 22SCSE2030634No ratings yet
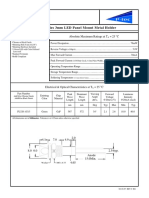
- PL320 Series 3mm LED Panel Mount Metal Holder: Features Absolute Maximum Ratings at T 25 °CDocument1 pagePL320 Series 3mm LED Panel Mount Metal Holder: Features Absolute Maximum Ratings at T 25 °CJajang JajaNo ratings yet
- Mathematics Actual SBaDocument8 pagesMathematics Actual SBaRohan lall100% (1)
- i30-Drive-N-Limited-EditioN-Product BulletinDocument2 pagesi30-Drive-N-Limited-EditioN-Product BulletinYaxuan ZhuNo ratings yet
- Fleet Strategy - ACS Power TransformersDocument96 pagesFleet Strategy - ACS Power TransformersManojNo ratings yet
- Spss SyllabusDocument2 pagesSpss SyllabusBhagwati ShuklaNo ratings yet
- Slide Presentation For Literature ReviewDocument8 pagesSlide Presentation For Literature Reviewfvg7vpte100% (1)
- Handbook of Alien Species in EuropeDocument26 pagesHandbook of Alien Species in Europehy0% (1)
- Avoiding Sentence ErrorsDocument26 pagesAvoiding Sentence Errorsapi-327193447No ratings yet
- Option B - BiochemistryDocument24 pagesOption B - BiochemistryRosaNo ratings yet
- HEIGHTS and GROUND COVERAGEDocument5 pagesHEIGHTS and GROUND COVERAGEanon_871836529No ratings yet
- UNV 【Datasheet】VMS-B180-A Datasheet - V1.3-ENDocument4 pagesUNV 【Datasheet】VMS-B180-A Datasheet - V1.3-ENChristian Hurtado S.No ratings yet
- At Syllabus NewDocument8 pagesAt Syllabus NewJohn Rey Bantay RodriguezNo ratings yet
- RE 2.3 MioDocument4 pagesRE 2.3 MioAngel Perez100% (1)
- Localization and InternationalizationDocument34 pagesLocalization and InternationalizationalexnekitaNo ratings yet
- Gurukul Hindi e Book by Sirhud KalraDocument17 pagesGurukul Hindi e Book by Sirhud KalraPARVANo ratings yet
- 1 Quarter TLE 7 Week 7 Lesson: Hazard and Risk in The WorkplaceDocument15 pages1 Quarter TLE 7 Week 7 Lesson: Hazard and Risk in The WorkplaceNazzer NacuspagNo ratings yet
- Ibo Vs Western CultureDocument4 pagesIbo Vs Western CultureSajida HydoubNo ratings yet
- PT Foundations-1Document5 pagesPT Foundations-1YNNo ratings yet
- PeopleSoft Integration BrokerDocument14 pagesPeopleSoft Integration BrokerGowriPachanathan0% (1)
- Digital BankingDocument3 pagesDigital BankingDPC Gym100% (1)
- Geothermal DrillingDocument14 pagesGeothermal DrillingDaniel TobingNo ratings yet
- Clase 23. Inosilicatos Cadena Doble AnfibolesDocument57 pagesClase 23. Inosilicatos Cadena Doble AnfibolesFranks Larry Antezana CalatayudNo ratings yet