Download as pdf or txt
You might also like
- 07 Palatal Expansion With The Nitanium Palatal ExpanderDocument12 pages07 Palatal Expansion With The Nitanium Palatal ExpanderIG Fraga100% (1)
- Reverse Facial Mask: Prepared by Shafa Fwad FaeeqDocument5 pagesReverse Facial Mask: Prepared by Shafa Fwad Faeeqمحمد العراقيNo ratings yet
- Fixed Functional AppliancesDocument82 pagesFixed Functional Appliancesdisha 146jandialNo ratings yet
- Maxillary ExpansionDocument8 pagesMaxillary ExpansionJoji IsacNo ratings yet
- Retention of Removable Orthodontic AppliancesDocument18 pagesRetention of Removable Orthodontic AppliancesFahd Yusuf KariapperNo ratings yet
- Final OrthoDocument46 pagesFinal OrthoAparna YadavNo ratings yet
- Evolution of The Leaf ExpanderDocument18 pagesEvolution of The Leaf ExpanderDevangana DasNo ratings yet
- Methods of Correction of Unilateral Posterior CrossbiteDocument36 pagesMethods of Correction of Unilateral Posterior CrossbiteSwathiLingannagariNo ratings yet
- Ijcrims 1Document9 pagesIjcrims 1smritiNo ratings yet
- Presentation 1Document10 pagesPresentation 1Osama GamilNo ratings yet
- Maxillary Expansion AppliancesDocument8 pagesMaxillary Expansion Appliancesmotivation munkeyNo ratings yet
- Orthodontics Ii (Lecture Note)Document29 pagesOrthodontics Ii (Lecture Note)Rufai HarunaNo ratings yet
- Molar Distalization.Document102 pagesMolar Distalization.BimalKrishnaNo ratings yet
- Slow Maxillary Expansion A Review 209085c4Document12 pagesSlow Maxillary Expansion A Review 209085c4jabbarNo ratings yet
- Jco - 2011!12!657 Locking The Screw After Rapid Palatal ExpansionDocument4 pagesJco - 2011!12!657 Locking The Screw After Rapid Palatal ExpansionAdrian Silva SantosNo ratings yet
- Twin Force Bite CorrectorDocument26 pagesTwin Force Bite CorrectorMohammed ElgendyNo ratings yet
- KLoop Molar Distalizing AppDocument7 pagesKLoop Molar Distalizing AppAngie Römer HaroNo ratings yet
- Bite RegistratnDocument68 pagesBite RegistratnBimalKrishnaNo ratings yet
- Paper Molar Distalization SambalpurDocument21 pagesPaper Molar Distalization SambalpurAsmita RayNo ratings yet
- FridayDocument55 pagesFridayJim HungNo ratings yet
- Know Your Tools Series: 'A Mind That Can Comprehend The Principle Will Device Its Own Methods.'' Nicolas AndryDocument91 pagesKnow Your Tools Series: 'A Mind That Can Comprehend The Principle Will Device Its Own Methods.'' Nicolas Andrymuhammad ammar naqviNo ratings yet
- Overdenture AttachmentsDocument42 pagesOverdenture AttachmentsEmad Alryashi100% (1)
- Nitanium Palatal Expander-A New Addition To Contemporary OrthodonticsDocument2 pagesNitanium Palatal Expander-A New Addition To Contemporary OrthodonticsVidal Almanza AvilaNo ratings yet
- 3 To 7 Years Longit Study 2004Document6 pages3 To 7 Years Longit Study 2004Hicham AL KHAYARNo ratings yet
- Stress BreakerDocument7 pagesStress BreakerEshan Verma33% (3)
- An Alternative Method of Space Closure: The Hycon DeviceDocument11 pagesAn Alternative Method of Space Closure: The Hycon DeviceBikramjeet SinghNo ratings yet
- Prosthodontics Preperation Before Implant Placement by DR Mohamed MarwanDocument17 pagesProsthodontics Preperation Before Implant Placement by DR Mohamed Marwanmostafa fayezNo ratings yet
- Distalization With The Miniscrew-Supported EZ Slider AuxiliaryDocument37 pagesDistalization With The Miniscrew-Supported EZ Slider AuxiliaryAnushriya DuttaNo ratings yet
- 6 D11-116 Julia Elodie VlachojannisDocument10 pages6 D11-116 Julia Elodie VlachojannisDr. Neesu KumbhatNo ratings yet
- 6.the Butterfly SystemDocument41 pages6.the Butterfly SystemShruti Garg100% (1)
- Evaluation of An Intraoral Maxillary MolarDocument8 pagesEvaluation of An Intraoral Maxillary MolarOdilon SouzaNo ratings yet
- Intramaxillary ElasticDocument4 pagesIntramaxillary ElasticMurshid SakhrNo ratings yet
- AbstractsDocument5 pagesAbstractsElham ZareNo ratings yet
- DR Kiara Kirpalani - Extra Oral Versus Intra Oral Appliance For Distal Movement of Maxillary Molars.Document27 pagesDR Kiara Kirpalani - Extra Oral Versus Intra Oral Appliance For Distal Movement of Maxillary Molars.Dr Kiara KirpalaniNo ratings yet
- Materi OSC DamonDocument20 pagesMateri OSC Damonfika_khayanNo ratings yet
- Molar Distalization in Begg Technique / Orthodontic Courses by Indian Dental AcademyDocument46 pagesMolar Distalization in Begg Technique / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Max ExpansionDocument4 pagesMax ExpansionPZNo ratings yet
- Major and Minor ConnectorsDocument34 pagesMajor and Minor Connectorsflee2alia0% (1)
- Amit Kumar BPT 2 Year CPRS, JmiDocument18 pagesAmit Kumar BPT 2 Year CPRS, JmiamaniNo ratings yet
- Refernce 18Document11 pagesRefernce 18Ali ZubiediNo ratings yet
- Zygoma ImplantDocument63 pagesZygoma ImplantKristina Robles100% (2)
- Transpalatal, Nance & Lingual Arch Appliances: Clinical Tips and ApplicationsDocument9 pagesTranspalatal, Nance & Lingual Arch Appliances: Clinical Tips and ApplicationsbanyubiruNo ratings yet
- Acumed ClavicleDocument6 pagesAcumed Claviclesiddig7No ratings yet
- Rapid Molar Intrusion Device / Orthodontic Courses by Indian Dental AcademyDocument55 pagesRapid Molar Intrusion Device / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- UntitledDocument61 pagesUntitledAdarsh varmaNo ratings yet
- Comparative Study Between Conventional En-Masse Retraction (Sliding Mechanics) and En-Masse Retraction Using Orthodontic Micro ImplantDocument9 pagesComparative Study Between Conventional En-Masse Retraction (Sliding Mechanics) and En-Masse Retraction Using Orthodontic Micro Implantdrgeorgejose7818No ratings yet
- Hybrid Appliances An UpdateDocument7 pagesHybrid Appliances An UpdateSushma DhimanNo ratings yet
- Maxillary Major ConnectorsDocument20 pagesMaxillary Major ConnectorsRohan GroverNo ratings yet
- Use Nonextraction Treatment When Possihle: Assessment of Borderline PatientsDocument18 pagesUse Nonextraction Treatment When Possihle: Assessment of Borderline PatientsMonse Sanchez UrbinaNo ratings yet
- Role of Stress Breakers in Removable Partial DentureDocument66 pagesRole of Stress Breakers in Removable Partial DentureNimra WaniNo ratings yet
- Or Dinar Yor Thodontics: S Tar Ting With The End in MindDocument10 pagesOr Dinar Yor Thodontics: S Tar Ting With The End in MindvijayprabugNo ratings yet
- Major Connectors and Minor Connectors: DR Prathibha Prasad Mds 1 Year KcdsDocument93 pagesMajor Connectors and Minor Connectors: DR Prathibha Prasad Mds 1 Year KcdsMNSNo ratings yet
- Seminar Components of CPDDocument77 pagesSeminar Components of CPDAtharva KambleNo ratings yet
- Stress Distribution in The Abutment and Retention Screw of A Single Implant Supporting A Prosthesis With Platform SwitchingDocument10 pagesStress Distribution in The Abutment and Retention Screw of A Single Implant Supporting A Prosthesis With Platform SwitchingMarlene Kasumi Gantier TakanoNo ratings yet
- Activatoranditsmodifications 120531102843 Phpapp02Document91 pagesActivatoranditsmodifications 120531102843 Phpapp02CarlosAndresPabonCortesNo ratings yet
- Elastics EditedDocument127 pagesElastics Editedmohammed.eskanderNo ratings yet
- Pendulum PedagogyDocument20 pagesPendulum PedagogyGudiyA KaurNo ratings yet
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- 2 Ib Nielsen StructurelDocument14 pages2 Ib Nielsen StructurelAomChanumpornNo ratings yet
- Changes in Bone Metabolisim Around Osseointegrated Implants Under LoadingDocument17 pagesChanges in Bone Metabolisim Around Osseointegrated Implants Under LoadingAomChanumpornNo ratings yet
- Treatment of Transverse DiscrepancyDocument75 pagesTreatment of Transverse DiscrepancyAomChanumpornNo ratings yet
- Rapid Palatal Expansion in The Young Adult A Case Report: January 2015Document7 pagesRapid Palatal Expansion in The Young Adult A Case Report: January 2015AomChanumpornNo ratings yet
- Journal of The World Federation of Orthodontists: ResearchDocument6 pagesJournal of The World Federation of Orthodontists: ResearchAomChanumpornNo ratings yet
- J Ijom 2009 06 028Document7 pagesJ Ijom 2009 06 028AomChanumpornNo ratings yet
- Investigation of The Levels of Different Salivary Stress Markers in Chronic Periodontitis PatientsDocument5 pagesInvestigation of The Levels of Different Salivary Stress Markers in Chronic Periodontitis PatientsAomChanumpornNo ratings yet
- DAFTAR PUSTAKA FixDocument3 pagesDAFTAR PUSTAKA FixRegina YunitaNo ratings yet
- Active and Passive Organs of SpeechDocument15 pagesActive and Passive Organs of SpeechТаня БродаNo ratings yet
- Ent CaseDocument5 pagesEnt CaseJENNIFER JOHN MBBS2020No ratings yet
- Prof. DR. M. Thaufiq S. Boesoirie, Dr. Sp. THT - KL, (K) - TERBARUDocument14 pagesProf. DR. M. Thaufiq S. Boesoirie, Dr. Sp. THT - KL, (K) - TERBARUalpriani patrasNo ratings yet
- Diagnosis & Management of Midface FracturesDocument66 pagesDiagnosis & Management of Midface FracturesSobia NaseemNo ratings yet
- Perforated EardrumDocument5 pagesPerforated EardrumElvinNo ratings yet
- Miñano - (OS 204) PN 2 - Skull and MandibleDocument2 pagesMiñano - (OS 204) PN 2 - Skull and MandibleMarion Rodelle MiñanoNo ratings yet
- 35 Hottest Hairstyles For Men With Straight HairDocument41 pages35 Hottest Hairstyles For Men With Straight HairStanleyNo ratings yet
- Okeson Dental CH 1-4 SummaryDocument9 pagesOkeson Dental CH 1-4 Summaryhallab1230% (1)
- Temporary Blindness After Inferior Alveolar Nerve BlockDocument2 pagesTemporary Blindness After Inferior Alveolar Nerve BlockIbramanto WarganegaraNo ratings yet
- Anatomy and Physiology of The Salivary GlandsDocument13 pagesAnatomy and Physiology of The Salivary GlandsTadjul Arifin Jr.No ratings yet
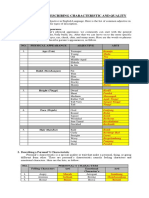
- Material Adjective in Describing Characteristic and QualityDocument2 pagesMaterial Adjective in Describing Characteristic and QualityAyu Ray Govinda DasiNo ratings yet
- Head Trauma: Group BDocument49 pagesHead Trauma: Group Bneal caffreyNo ratings yet
- Nasal Irrigation - RachanonDocument2 pagesNasal Irrigation - RachanonShakritnat SakonNo ratings yet
- Sensory Organs: Medical Surgical NursingDocument17 pagesSensory Organs: Medical Surgical NursingHoney PrasadNo ratings yet
- The Cisterna Magna SeptaDocument13 pagesThe Cisterna Magna SeptaFrancisco A. Villegas-LópezNo ratings yet
- Muscles of Facial ExpressionDocument93 pagesMuscles of Facial Expressionsiddu76100% (2)
- Otorhino Dr. R. RegaladoDocument4 pagesOtorhino Dr. R. RegaladoDoctor CastleNo ratings yet
- Oral Physio Slides - 5.mastication Dynamics of OcclusionDocument48 pagesOral Physio Slides - 5.mastication Dynamics of OcclusionMuhammadHafizZainudinNo ratings yet
- Anatomy of AirwayDocument50 pagesAnatomy of AirwayHari Om ChaurasiyaNo ratings yet
- Canine ImpactionDocument144 pagesCanine ImpactionMini Robert100% (1)
- Cranial Nerve TestsDocument2 pagesCranial Nerve TestsJustin Derick C. JaraNo ratings yet
- Competitive Comparison Tampa, Florida: June 2020Document4 pagesCompetitive Comparison Tampa, Florida: June 2020Marie Carh CabingasNo ratings yet
- Complications of SinusitisDocument96 pagesComplications of Sinusitiskamal saudNo ratings yet
- Access Osteotomies in Oral and Maxillofacial SurgeryDocument47 pagesAccess Osteotomies in Oral and Maxillofacial SurgeryRehana Sultana100% (3)
- Head & Neck A&pDocument15 pagesHead & Neck A&pJSeashark100% (6)
- Monro Kellie Doctrine/ PrincipleDocument5 pagesMonro Kellie Doctrine/ PrincipleAngelu Gabrielle CastroNo ratings yet
- CraniumDocument20 pagesCraniumDifa ZafiraNo ratings yet
- Describing People Greyscale Key Picture Description Exercises 14721Document3 pagesDescribing People Greyscale Key Picture Description Exercises 14721Gulderay IklassovaNo ratings yet
- 2 Full-Cusp Class II Malocclusion With BilateralDocument20 pages2 Full-Cusp Class II Malocclusion With BilateralJULIAN ANDRES CAICEDO RIVERANo ratings yet