
Matern Child Health J
Matern Child Health J
You might also like
- The Calling of The Health Care ProviderDocument6 pagesThe Calling of The Health Care ProviderRobin Edeza100% (1)
- Policy MemoDocument4 pagesPolicy Memoapi-340053591No ratings yet
- Core Elements of Evidence-Bases Gerontological Nursing PracticeDocument15 pagesCore Elements of Evidence-Bases Gerontological Nursing PracticeGrape Juice67% (3)
- Kepkel 1Document11 pagesKepkel 1dewi retnoNo ratings yet
- Associations of Family-Centered Care With Health Care Outcomes For Children With Special Health Care NeedsDocument13 pagesAssociations of Family-Centered Care With Health Care Outcomes For Children With Special Health Care NeedsAstridNo ratings yet
- IIN RobertRCetal - healthEducationResearch.vol22.No.3Document14 pagesIIN RobertRCetal - healthEducationResearch.vol22.No.3Iniciativa Contra la Desnutrición Infantil - IDINo ratings yet
- Print 1-3 - School-Based - Health - CentersDocument5 pagesPrint 1-3 - School-Based - Health - CentersNikolas IGDNo ratings yet
- Health Services Needs Day Centers: of ChildrenDocument5 pagesHealth Services Needs Day Centers: of ChildrenAndreea RaduNo ratings yet
- Practical Research 2 Fin-1Document24 pagesPractical Research 2 Fin-1yyadperezNo ratings yet
- Pediatric Health 2011 Report BriefDocument4 pagesPediatric Health 2011 Report BriefJayCesarNo ratings yet
- Manuscript Revision 10.15.20Document22 pagesManuscript Revision 10.15.20John SmithNo ratings yet
- RRL 1Document7 pagesRRL 1Jannah BalasbasNo ratings yet
- Home Visiting 101Document2 pagesHome Visiting 101Center for American ProgressNo ratings yet
- 20.3 Noyes GrosserDocument20 pages20.3 Noyes GrosserRashidah Abd WahidNo ratings yet
- Pediatrics 2012 Fu E496 503jnnjnjnjDocument10 pagesPediatrics 2012 Fu E496 503jnnjnjnjDyera JessenskyNo ratings yet
- Parental Satisfaction of Child 'S Perioperative CareDocument8 pagesParental Satisfaction of Child 'S Perioperative CareHasriana BudimanNo ratings yet
- Care Map FinalDocument18 pagesCare Map Finalapi-311540850No ratings yet
- RRL 3Document6 pagesRRL 3Jannah BalasbasNo ratings yet
- Perception of Students On The Health Services of The School ClinicDocument2 pagesPerception of Students On The Health Services of The School ClinicMary BiscochoNo ratings yet
- Breastfeeding Knowledge and Attitudes of Health Professional Students: A Systematic ReviewDocument11 pagesBreastfeeding Knowledge and Attitudes of Health Professional Students: A Systematic ReviewMohamed L TarawalieNo ratings yet
- Liza Journal ReadingDocument5 pagesLiza Journal ReadingAziil LiizaNo ratings yet
- Pediatric Recent AdvancementDocument2 pagesPediatric Recent AdvancementAnonymous ceYk4p4No ratings yet
- Press Release 12-09 - New Study Raises Health and Safety Concerns inDocument3 pagesPress Release 12-09 - New Study Raises Health and Safety Concerns inhealthoregonNo ratings yet
- Medical HomeDocument1 pageMedical Homemina000005No ratings yet
- What Reasonably Expect?: The Contribution of School Health Education Community Health Promotion: CanDocument8 pagesWhat Reasonably Expect?: The Contribution of School Health Education Community Health Promotion: CansapiokaravoNo ratings yet
- E N I F - C C A C C: Ositive Ffects of A Ursing Ntervention ON Amily Entered ARE IN Dult Ritical AREDocument11 pagesE N I F - C C A C C: Ositive Ffects of A Ursing Ntervention ON Amily Entered ARE IN Dult Ritical AREJ-lLya EdeltRudisNo ratings yet
- Discussion For Module 7Document3 pagesDiscussion For Module 7Hussain MirzaNo ratings yet
- Family Centred Care Literature ReviewDocument6 pagesFamily Centred Care Literature Reviewc5pgcqzv100% (1)
- School-Based Health Centers: Cost-Benefit Analysis and Impact On Health Care DisparitiesDocument7 pagesSchool-Based Health Centers: Cost-Benefit Analysis and Impact On Health Care DisparitiesNikolas IGDNo ratings yet
- 3 School Health Nursing - Field in NursingDocument14 pages3 School Health Nursing - Field in NursingsannsannNo ratings yet
- Jurnal Tentang KeperawatanDocument8 pagesJurnal Tentang KeperawatanAlex Synyster Gates VNo ratings yet
- Familiy AssesentDocument35 pagesFamiliy AssesentmurvinandNo ratings yet
- Incorporating Patient-And Family-Centered Care Into Practice: The PA Medical Home InitiativeDocument6 pagesIncorporating Patient-And Family-Centered Care Into Practice: The PA Medical Home InitiativeNikmahNo ratings yet
- 3 School Health Nursing - Field in NursingDocument14 pages3 School Health Nursing - Field in NursingsannsannNo ratings yet
- Chapter 1 5Document132 pagesChapter 1 5Kylle AlimosaNo ratings yet
- Stressors Facing Home-Based Primary Care ProvidersDocument5 pagesStressors Facing Home-Based Primary Care ProvidersSandra RNo ratings yet
- Patient Safety A Literature Review To Inform An Evaluation of A Maternity ServiceDocument5 pagesPatient Safety A Literature Review To Inform An Evaluation of A Maternity ServicetdqmodcndNo ratings yet
- RetrieveDocument29 pagesRetrievemarielecostudio80No ratings yet
- Barriers and Facilitators To The Implementation of Lay Health Worker Programmes To Improve Access To Maternal and Child Health: Qualitative Evidence Synthesis (Review)Document5 pagesBarriers and Facilitators To The Implementation of Lay Health Worker Programmes To Improve Access To Maternal and Child Health: Qualitative Evidence Synthesis (Review)ArisNo ratings yet
- CHAPTER 1 Community Health Nursing IIDocument10 pagesCHAPTER 1 Community Health Nursing IIFrances LiqueNo ratings yet
- Shi 2001Document15 pagesShi 2001pamelwNo ratings yet
- Literature Review Childhood ObesityDocument4 pagesLiterature Review Childhood Obesityc5j07dce100% (1)
- Factors Constraining Adherence SDocument20 pagesFactors Constraining Adherence SayangsarulNo ratings yet
- Ebr MacalolotDocument4 pagesEbr Macalolotquen.chuaNo ratings yet
- An Intensive Family Intervention Clinic For Reducing Childhood ObesityDocument8 pagesAn Intensive Family Intervention Clinic For Reducing Childhood ObesityFarha AamirNo ratings yet
- 01-0 Canadá - or - Mantel-HaenszelDocument16 pages01-0 Canadá - or - Mantel-HaenszelLUIS GUSTAVO ESCOBAL DIAZNo ratings yet
- Family-Centred Care For Hospitalized Children Aged 0-12 Years: A Systematic Review of Qualitative Studies ReviewersDocument19 pagesFamily-Centred Care For Hospitalized Children Aged 0-12 Years: A Systematic Review of Qualitative Studies ReviewersJUBY24No ratings yet
- MCN FINALS MergedDocument193 pagesMCN FINALS MergedNeru RoriNo ratings yet
- Nursing Symposium ReportDocument16 pagesNursing Symposium ReportTom MeyerNo ratings yet
- Bclac Grant Proposal FinalDocument30 pagesBclac Grant Proposal Finalapi-261666555No ratings yet
- Healthy Teens Counseling ApproachDocument6 pagesHealthy Teens Counseling ApproachDebbie CharlotteNo ratings yet
- ArikDocument14 pagesArikArditya Romy Stay CoolNo ratings yet
- Qualifications of Head Teachers and The Numbers of Healthcare Personnel Available in Public and Private Schools in Owerri Municipal, Imo State, NigeriaDocument17 pagesQualifications of Head Teachers and The Numbers of Healthcare Personnel Available in Public and Private Schools in Owerri Municipal, Imo State, NigeriaPUBLISHER JOURNALNo ratings yet
- Family-Centred Care in Paediatric and Neonatal Nursing - A Literature ReviewDocument4 pagesFamily-Centred Care in Paediatric and Neonatal Nursing - A Literature Reviewhyzypif0gif3No ratings yet
- Community Health Planning, Implementation, and EvaluationDocument9 pagesCommunity Health Planning, Implementation, and EvaluationKarl Angelo MontanoNo ratings yet
- Articulo OdontopediatriaDocument8 pagesArticulo OdontopediatriaEvelyn RiveraNo ratings yet
- Medical Home Blog ArticleDocument6 pagesMedical Home Blog Article99tomellsNo ratings yet
- Pediatrics 2013 Miller S215 8Document6 pagesPediatrics 2013 Miller S215 8Timothy Eduard A. SupitNo ratings yet
- Obesity Literature ReviewDocument8 pagesObesity Literature Revieweubvhsvkg100% (1)
- Ke Ku Una Na Au: A Native Hawaiian Behavioral Health Initiative at The Queen's Medical CenterDocument7 pagesKe Ku Una Na Au: A Native Hawaiian Behavioral Health Initiative at The Queen's Medical CenterChandra EkaNo ratings yet
- Needs Assessment in Public Health: A Practical Guide for Students and ProfessionalsFrom EverandNeeds Assessment in Public Health: A Practical Guide for Students and ProfessionalsNo ratings yet
- Pharmacotherapy of Schizophrenia Paranoid TypeDocument7 pagesPharmacotherapy of Schizophrenia Paranoid TypeCynthia GendiNo ratings yet
- Nursing: Your Name, Your Department Faculty and Preceptor This Is 68 Point FontDocument1 pageNursing: Your Name, Your Department Faculty and Preceptor This Is 68 Point FontCynthia GendiNo ratings yet
- Wound Healing: Student Name Institutional Affiliation Course Title Instructor Name Due DateDocument5 pagesWound Healing: Student Name Institutional Affiliation Course Title Instructor Name Due DateCynthia GendiNo ratings yet
- Organizational Change Text Pages 297 318Document24 pagesOrganizational Change Text Pages 297 318Cynthia GendiNo ratings yet
- Pharmaceutical Company ProfileDocument8 pagesPharmaceutical Company Profilejagdale kunal100% (1)
- Adjective Clause Ilave Test (Tipdil)Document6 pagesAdjective Clause Ilave Test (Tipdil)İlayda ErdoğanNo ratings yet
- HPCSA Booklet 9 Patient Informed ConsentDocument18 pagesHPCSA Booklet 9 Patient Informed Consentpieterinpretoria391No ratings yet
- Live Music Promotes Positive Behaviours inDocument9 pagesLive Music Promotes Positive Behaviours inSaul MorenoNo ratings yet
- Individual Contingent PayDocument14 pagesIndividual Contingent PaybullionhameedNo ratings yet
- Clinical Documentation Zuri March 28 2023Document36 pagesClinical Documentation Zuri March 28 2023KUYA CHICO MORALESNo ratings yet
- Pharmaceuticals Executive Summary PDFDocument10 pagesPharmaceuticals Executive Summary PDFPaes C. MarceloNo ratings yet
- Soal Hitungan DosisDocument2 pagesSoal Hitungan DosissabrinaNo ratings yet
- BP Monitoring Log BookDocument2 pagesBP Monitoring Log Bookroland acacioNo ratings yet
- An Historical Perspective On Principles of Osteopathy - Jane Eliza Stark. 2013Document8 pagesAn Historical Perspective On Principles of Osteopathy - Jane Eliza Stark. 2013Adolfo Esteban Soto MartinezNo ratings yet
- Hospital-Bill-Form DDocument2 pagesHospital-Bill-Form Ddeharemmanuel64No ratings yet
- Personalize Nutrition TechnologyDocument4 pagesPersonalize Nutrition TechnologySBSNo ratings yet
- IsbarDocument2 pagesIsbarKristian Karl Bautista Kiw-isNo ratings yet
- The Importance of Confidentiality in HealthcareDocument16 pagesThe Importance of Confidentiality in HealthcareBurly StoneNo ratings yet
- Name: Age: Sex: Date:: Date Ordered Medication-Dose-Route TIM E Date Sign Date Sign Date SignDocument3 pagesName: Age: Sex: Date:: Date Ordered Medication-Dose-Route TIM E Date Sign Date Sign Date SignCezanne CruzNo ratings yet
- The Open Dentistry Journal: Methodologies in Orthodontic Pain Management: A ReviewDocument6 pagesThe Open Dentistry Journal: Methodologies in Orthodontic Pain Management: A Reviewnevin santhoshNo ratings yet
- Emergency Action PlanDocument2 pagesEmergency Action Planapi-456450858No ratings yet
- 2018 08 13 (一) 「醫療器材法規與實務」講座系列課程十二Document84 pages2018 08 13 (一) 「醫療器材法規與實務」講座系列課程十二Dr.Sivakumar SelvarajNo ratings yet
- Care Plan BronchitisDocument3 pagesCare Plan BronchitisYousef JafarNo ratings yet
- Tamaraw PDFDocument2 pagesTamaraw PDFGab MolinaNo ratings yet
- All India Institute of Medical Sciences: List of Faculty - Departmentswise As On 10.10.2014 at The A.I.I.M.S., New DelhiDocument23 pagesAll India Institute of Medical Sciences: List of Faculty - Departmentswise As On 10.10.2014 at The A.I.I.M.S., New DelhiSaif AliNo ratings yet
- SOGC - Endometriosis Diagnosis and ManagementDocument36 pagesSOGC - Endometriosis Diagnosis and ManagementreioctabianoNo ratings yet
- MBBS Seat AllotmentDocument4 pagesMBBS Seat AllotmentAnbalagan VNo ratings yet
- DR Jack Barker & Colin Sweeney - 'War and Peace A CCIO and ICT Director Working Together'Document20 pagesDR Jack Barker & Colin Sweeney - 'War and Peace A CCIO and ICT Director Working Together'CCIONetworkNo ratings yet
- DME UG MOP UP Round Allotment Result 2021Document32 pagesDME UG MOP UP Round Allotment Result 2021Harsh vardhan BhattNo ratings yet
- 2 - Manejo de DVA en El Shock - Desde La Norepinefrina Al Azul de MetilenoDocument72 pages2 - Manejo de DVA en El Shock - Desde La Norepinefrina Al Azul de MetilenoJose Soto (Pepe S)No ratings yet
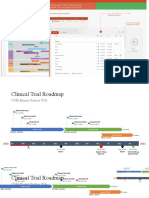
- Clinical Trial Roadmap Template - WsDocument4 pagesClinical Trial Roadmap Template - WsDaniel AlejandroNo ratings yet
- CV Dyki Dwi Anwar NewDocument3 pagesCV Dyki Dwi Anwar NewDyki AnwarNo ratings yet




























































































Download as docx, pdf, or txt
You might also like
- The Calling of The Health Care ProviderDocument6 pagesThe Calling of The Health Care ProviderRobin Edeza100% (1)
- Policy MemoDocument4 pagesPolicy Memoapi-340053591No ratings yet
- Core Elements of Evidence-Bases Gerontological Nursing PracticeDocument15 pagesCore Elements of Evidence-Bases Gerontological Nursing PracticeGrape Juice67% (3)
- Kepkel 1Document11 pagesKepkel 1dewi retnoNo ratings yet
- Associations of Family-Centered Care With Health Care Outcomes For Children With Special Health Care NeedsDocument13 pagesAssociations of Family-Centered Care With Health Care Outcomes For Children With Special Health Care NeedsAstridNo ratings yet
- IIN RobertRCetal - healthEducationResearch.vol22.No.3Document14 pagesIIN RobertRCetal - healthEducationResearch.vol22.No.3Iniciativa Contra la Desnutrición Infantil - IDINo ratings yet
- Print 1-3 - School-Based - Health - CentersDocument5 pagesPrint 1-3 - School-Based - Health - CentersNikolas IGDNo ratings yet
- Health Services Needs Day Centers: of ChildrenDocument5 pagesHealth Services Needs Day Centers: of ChildrenAndreea RaduNo ratings yet
- Practical Research 2 Fin-1Document24 pagesPractical Research 2 Fin-1yyadperezNo ratings yet
- Pediatric Health 2011 Report BriefDocument4 pagesPediatric Health 2011 Report BriefJayCesarNo ratings yet
- Manuscript Revision 10.15.20Document22 pagesManuscript Revision 10.15.20John SmithNo ratings yet
- RRL 1Document7 pagesRRL 1Jannah BalasbasNo ratings yet
- Home Visiting 101Document2 pagesHome Visiting 101Center for American ProgressNo ratings yet
- 20.3 Noyes GrosserDocument20 pages20.3 Noyes GrosserRashidah Abd WahidNo ratings yet
- Pediatrics 2012 Fu E496 503jnnjnjnjDocument10 pagesPediatrics 2012 Fu E496 503jnnjnjnjDyera JessenskyNo ratings yet
- Parental Satisfaction of Child 'S Perioperative CareDocument8 pagesParental Satisfaction of Child 'S Perioperative CareHasriana BudimanNo ratings yet
- Care Map FinalDocument18 pagesCare Map Finalapi-311540850No ratings yet
- RRL 3Document6 pagesRRL 3Jannah BalasbasNo ratings yet
- Perception of Students On The Health Services of The School ClinicDocument2 pagesPerception of Students On The Health Services of The School ClinicMary BiscochoNo ratings yet
- Breastfeeding Knowledge and Attitudes of Health Professional Students: A Systematic ReviewDocument11 pagesBreastfeeding Knowledge and Attitudes of Health Professional Students: A Systematic ReviewMohamed L TarawalieNo ratings yet
- Liza Journal ReadingDocument5 pagesLiza Journal ReadingAziil LiizaNo ratings yet
- Pediatric Recent AdvancementDocument2 pagesPediatric Recent AdvancementAnonymous ceYk4p4No ratings yet
- Press Release 12-09 - New Study Raises Health and Safety Concerns inDocument3 pagesPress Release 12-09 - New Study Raises Health and Safety Concerns inhealthoregonNo ratings yet
- Medical HomeDocument1 pageMedical Homemina000005No ratings yet
- What Reasonably Expect?: The Contribution of School Health Education Community Health Promotion: CanDocument8 pagesWhat Reasonably Expect?: The Contribution of School Health Education Community Health Promotion: CansapiokaravoNo ratings yet
- E N I F - C C A C C: Ositive Ffects of A Ursing Ntervention ON Amily Entered ARE IN Dult Ritical AREDocument11 pagesE N I F - C C A C C: Ositive Ffects of A Ursing Ntervention ON Amily Entered ARE IN Dult Ritical AREJ-lLya EdeltRudisNo ratings yet
- Discussion For Module 7Document3 pagesDiscussion For Module 7Hussain MirzaNo ratings yet
- Family Centred Care Literature ReviewDocument6 pagesFamily Centred Care Literature Reviewc5pgcqzv100% (1)
- School-Based Health Centers: Cost-Benefit Analysis and Impact On Health Care DisparitiesDocument7 pagesSchool-Based Health Centers: Cost-Benefit Analysis and Impact On Health Care DisparitiesNikolas IGDNo ratings yet
- 3 School Health Nursing - Field in NursingDocument14 pages3 School Health Nursing - Field in NursingsannsannNo ratings yet
- Jurnal Tentang KeperawatanDocument8 pagesJurnal Tentang KeperawatanAlex Synyster Gates VNo ratings yet
- Familiy AssesentDocument35 pagesFamiliy AssesentmurvinandNo ratings yet
- Incorporating Patient-And Family-Centered Care Into Practice: The PA Medical Home InitiativeDocument6 pagesIncorporating Patient-And Family-Centered Care Into Practice: The PA Medical Home InitiativeNikmahNo ratings yet
- 3 School Health Nursing - Field in NursingDocument14 pages3 School Health Nursing - Field in NursingsannsannNo ratings yet
- Chapter 1 5Document132 pagesChapter 1 5Kylle AlimosaNo ratings yet
- Stressors Facing Home-Based Primary Care ProvidersDocument5 pagesStressors Facing Home-Based Primary Care ProvidersSandra RNo ratings yet
- Patient Safety A Literature Review To Inform An Evaluation of A Maternity ServiceDocument5 pagesPatient Safety A Literature Review To Inform An Evaluation of A Maternity ServicetdqmodcndNo ratings yet
- RetrieveDocument29 pagesRetrievemarielecostudio80No ratings yet
- Barriers and Facilitators To The Implementation of Lay Health Worker Programmes To Improve Access To Maternal and Child Health: Qualitative Evidence Synthesis (Review)Document5 pagesBarriers and Facilitators To The Implementation of Lay Health Worker Programmes To Improve Access To Maternal and Child Health: Qualitative Evidence Synthesis (Review)ArisNo ratings yet
- CHAPTER 1 Community Health Nursing IIDocument10 pagesCHAPTER 1 Community Health Nursing IIFrances LiqueNo ratings yet
- Shi 2001Document15 pagesShi 2001pamelwNo ratings yet
- Literature Review Childhood ObesityDocument4 pagesLiterature Review Childhood Obesityc5j07dce100% (1)
- Factors Constraining Adherence SDocument20 pagesFactors Constraining Adherence SayangsarulNo ratings yet
- Ebr MacalolotDocument4 pagesEbr Macalolotquen.chuaNo ratings yet
- An Intensive Family Intervention Clinic For Reducing Childhood ObesityDocument8 pagesAn Intensive Family Intervention Clinic For Reducing Childhood ObesityFarha AamirNo ratings yet
- 01-0 Canadá - or - Mantel-HaenszelDocument16 pages01-0 Canadá - or - Mantel-HaenszelLUIS GUSTAVO ESCOBAL DIAZNo ratings yet
- Family-Centred Care For Hospitalized Children Aged 0-12 Years: A Systematic Review of Qualitative Studies ReviewersDocument19 pagesFamily-Centred Care For Hospitalized Children Aged 0-12 Years: A Systematic Review of Qualitative Studies ReviewersJUBY24No ratings yet
- MCN FINALS MergedDocument193 pagesMCN FINALS MergedNeru RoriNo ratings yet
- Nursing Symposium ReportDocument16 pagesNursing Symposium ReportTom MeyerNo ratings yet
- Bclac Grant Proposal FinalDocument30 pagesBclac Grant Proposal Finalapi-261666555No ratings yet
- Healthy Teens Counseling ApproachDocument6 pagesHealthy Teens Counseling ApproachDebbie CharlotteNo ratings yet
- ArikDocument14 pagesArikArditya Romy Stay CoolNo ratings yet
- Qualifications of Head Teachers and The Numbers of Healthcare Personnel Available in Public and Private Schools in Owerri Municipal, Imo State, NigeriaDocument17 pagesQualifications of Head Teachers and The Numbers of Healthcare Personnel Available in Public and Private Schools in Owerri Municipal, Imo State, NigeriaPUBLISHER JOURNALNo ratings yet
- Family-Centred Care in Paediatric and Neonatal Nursing - A Literature ReviewDocument4 pagesFamily-Centred Care in Paediatric and Neonatal Nursing - A Literature Reviewhyzypif0gif3No ratings yet
- Community Health Planning, Implementation, and EvaluationDocument9 pagesCommunity Health Planning, Implementation, and EvaluationKarl Angelo MontanoNo ratings yet
- Articulo OdontopediatriaDocument8 pagesArticulo OdontopediatriaEvelyn RiveraNo ratings yet
- Medical Home Blog ArticleDocument6 pagesMedical Home Blog Article99tomellsNo ratings yet
- Pediatrics 2013 Miller S215 8Document6 pagesPediatrics 2013 Miller S215 8Timothy Eduard A. SupitNo ratings yet
- Obesity Literature ReviewDocument8 pagesObesity Literature Revieweubvhsvkg100% (1)
- Ke Ku Una Na Au: A Native Hawaiian Behavioral Health Initiative at The Queen's Medical CenterDocument7 pagesKe Ku Una Na Au: A Native Hawaiian Behavioral Health Initiative at The Queen's Medical CenterChandra EkaNo ratings yet
- Needs Assessment in Public Health: A Practical Guide for Students and ProfessionalsFrom EverandNeeds Assessment in Public Health: A Practical Guide for Students and ProfessionalsNo ratings yet
- Pharmacotherapy of Schizophrenia Paranoid TypeDocument7 pagesPharmacotherapy of Schizophrenia Paranoid TypeCynthia GendiNo ratings yet
- Nursing: Your Name, Your Department Faculty and Preceptor This Is 68 Point FontDocument1 pageNursing: Your Name, Your Department Faculty and Preceptor This Is 68 Point FontCynthia GendiNo ratings yet
- Wound Healing: Student Name Institutional Affiliation Course Title Instructor Name Due DateDocument5 pagesWound Healing: Student Name Institutional Affiliation Course Title Instructor Name Due DateCynthia GendiNo ratings yet
- Organizational Change Text Pages 297 318Document24 pagesOrganizational Change Text Pages 297 318Cynthia GendiNo ratings yet
- Pharmaceutical Company ProfileDocument8 pagesPharmaceutical Company Profilejagdale kunal100% (1)
- Adjective Clause Ilave Test (Tipdil)Document6 pagesAdjective Clause Ilave Test (Tipdil)İlayda ErdoğanNo ratings yet
- HPCSA Booklet 9 Patient Informed ConsentDocument18 pagesHPCSA Booklet 9 Patient Informed Consentpieterinpretoria391No ratings yet
- Live Music Promotes Positive Behaviours inDocument9 pagesLive Music Promotes Positive Behaviours inSaul MorenoNo ratings yet
- Individual Contingent PayDocument14 pagesIndividual Contingent PaybullionhameedNo ratings yet
- Clinical Documentation Zuri March 28 2023Document36 pagesClinical Documentation Zuri March 28 2023KUYA CHICO MORALESNo ratings yet
- Pharmaceuticals Executive Summary PDFDocument10 pagesPharmaceuticals Executive Summary PDFPaes C. MarceloNo ratings yet
- Soal Hitungan DosisDocument2 pagesSoal Hitungan DosissabrinaNo ratings yet
- BP Monitoring Log BookDocument2 pagesBP Monitoring Log Bookroland acacioNo ratings yet
- An Historical Perspective On Principles of Osteopathy - Jane Eliza Stark. 2013Document8 pagesAn Historical Perspective On Principles of Osteopathy - Jane Eliza Stark. 2013Adolfo Esteban Soto MartinezNo ratings yet
- Hospital-Bill-Form DDocument2 pagesHospital-Bill-Form Ddeharemmanuel64No ratings yet
- Personalize Nutrition TechnologyDocument4 pagesPersonalize Nutrition TechnologySBSNo ratings yet
- IsbarDocument2 pagesIsbarKristian Karl Bautista Kiw-isNo ratings yet
- The Importance of Confidentiality in HealthcareDocument16 pagesThe Importance of Confidentiality in HealthcareBurly StoneNo ratings yet
- Name: Age: Sex: Date:: Date Ordered Medication-Dose-Route TIM E Date Sign Date Sign Date SignDocument3 pagesName: Age: Sex: Date:: Date Ordered Medication-Dose-Route TIM E Date Sign Date Sign Date SignCezanne CruzNo ratings yet
- The Open Dentistry Journal: Methodologies in Orthodontic Pain Management: A ReviewDocument6 pagesThe Open Dentistry Journal: Methodologies in Orthodontic Pain Management: A Reviewnevin santhoshNo ratings yet
- Emergency Action PlanDocument2 pagesEmergency Action Planapi-456450858No ratings yet
- 2018 08 13 (一) 「醫療器材法規與實務」講座系列課程十二Document84 pages2018 08 13 (一) 「醫療器材法規與實務」講座系列課程十二Dr.Sivakumar SelvarajNo ratings yet
- Care Plan BronchitisDocument3 pagesCare Plan BronchitisYousef JafarNo ratings yet
- Tamaraw PDFDocument2 pagesTamaraw PDFGab MolinaNo ratings yet
- All India Institute of Medical Sciences: List of Faculty - Departmentswise As On 10.10.2014 at The A.I.I.M.S., New DelhiDocument23 pagesAll India Institute of Medical Sciences: List of Faculty - Departmentswise As On 10.10.2014 at The A.I.I.M.S., New DelhiSaif AliNo ratings yet
- SOGC - Endometriosis Diagnosis and ManagementDocument36 pagesSOGC - Endometriosis Diagnosis and ManagementreioctabianoNo ratings yet
- MBBS Seat AllotmentDocument4 pagesMBBS Seat AllotmentAnbalagan VNo ratings yet
- DR Jack Barker & Colin Sweeney - 'War and Peace A CCIO and ICT Director Working Together'Document20 pagesDR Jack Barker & Colin Sweeney - 'War and Peace A CCIO and ICT Director Working Together'CCIONetworkNo ratings yet
- DME UG MOP UP Round Allotment Result 2021Document32 pagesDME UG MOP UP Round Allotment Result 2021Harsh vardhan BhattNo ratings yet
- 2 - Manejo de DVA en El Shock - Desde La Norepinefrina Al Azul de MetilenoDocument72 pages2 - Manejo de DVA en El Shock - Desde La Norepinefrina Al Azul de MetilenoJose Soto (Pepe S)No ratings yet
- Clinical Trial Roadmap Template - WsDocument4 pagesClinical Trial Roadmap Template - WsDaniel AlejandroNo ratings yet
- CV Dyki Dwi Anwar NewDocument3 pagesCV Dyki Dwi Anwar NewDyki AnwarNo ratings yet