Download as pdf or txt
You might also like
- History Taking Form in Gynecology & ObstetricsDocument8 pagesHistory Taking Form in Gynecology & ObstetricsAbdullah Matar86% (7)
- Alternative Item Formats: Sample QuestionsDocument33 pagesAlternative Item Formats: Sample QuestionsCristianFranceschi100% (2)
- Dentistry Reviewer: C. Tricuspid ValveDocument47 pagesDentistry Reviewer: C. Tricuspid ValvePatricia L.No ratings yet
- PNDSDocument9 pagesPNDSivy_espesoNo ratings yet
- Journal of ElectrocardiologyDocument4 pagesJournal of ElectrocardiologyMaria AlejandraNo ratings yet
- Depooter 2017Document9 pagesDepooter 2017Maria AlejandraNo ratings yet
- Circep 119 008210Document12 pagesCircep 119 008210Paul CalbureanNo ratings yet
- Noninvasive Electrocardiographic Mapping To Improve Patient Selection For Cardiac Resynchronization TherapyDocument9 pagesNoninvasive Electrocardiographic Mapping To Improve Patient Selection For Cardiac Resynchronization TherapyHappy PramandaNo ratings yet
- Real-Time 3D Echo in Patient Selection For Cardiac Resynchronization TherapyDocument11 pagesReal-Time 3D Echo in Patient Selection For Cardiac Resynchronization TherapycesareNo ratings yet
- Journal of Electrocardiology: ArticleinfoDocument6 pagesJournal of Electrocardiology: ArticleinfoVlada SiricNo ratings yet
- Journal of Electrocardiology 50 (2017) 652 - 660-1Document9 pagesJournal of Electrocardiology 50 (2017) 652 - 660-1arnabsengNo ratings yet
- Does Mechanical Dyssynchrony in Addition To QRS Area Ensure Sustained Response To Cardiac Resynchronization Therapy?Document8 pagesDoes Mechanical Dyssynchrony in Addition To QRS Area Ensure Sustained Response To Cardiac Resynchronization Therapy?Венцислав МирчевNo ratings yet
- TSV Con Aberrancia o TVDocument7 pagesTSV Con Aberrancia o TVOliverVasconcelosNo ratings yet
- Wide Complex TachyDocument26 pagesWide Complex TachywongNo ratings yet
- Sequential Versus Simultaneous Biventricular Resynchronization For Severe Heart Failure - Evaluation by Tissue Doppler ImagingDocument7 pagesSequential Versus Simultaneous Biventricular Resynchronization For Severe Heart Failure - Evaluation by Tissue Doppler Imagingfluid_man_brazilNo ratings yet
- YQVx Q47 XSBK 6 NCG 4 W 9 Ypp KRDocument6 pagesYQVx Q47 XSBK 6 NCG 4 W 9 Ypp KRRicardo MingireanovNo ratings yet
- Arrhythmia 4 KDHDocument61 pagesArrhythmia 4 KDHMarcela MurafaNo ratings yet
- Electrocardiographic Optimization Techniques in Resynchronization TherapyDocument11 pagesElectrocardiographic Optimization Techniques in Resynchronization TherapyAndri AkbarNo ratings yet
- Biomedical Signal Processing and ControlDocument8 pagesBiomedical Signal Processing and ControlMaria AlejandraNo ratings yet
- Luis Fernando Pava MolanoDocument5 pagesLuis Fernando Pava MolanoVallejo Romo Alberto CristianNo ratings yet
- Rashid 2021Document10 pagesRashid 2021Carmen Cuadros BeigesNo ratings yet
- QT Dispersion Problems of Methodology AnDocument15 pagesQT Dispersion Problems of Methodology AnedNo ratings yet
- DTI Superposition PDFDocument7 pagesDTI Superposition PDFEtel SilvaNo ratings yet
- 2009 - Donis - Improving The Diagnosis of Bundle Branch Block by Analysing BSPMDocument9 pages2009 - Donis - Improving The Diagnosis of Bundle Branch Block by Analysing BSPMbamarcliNo ratings yet
- Quantification Asynchhrony Last REv 03 2008 Reordenando AntDocument20 pagesQuantification Asynchhrony Last REv 03 2008 Reordenando AntEtel SilvaNo ratings yet
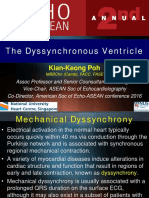
- The Dyssynchronous Ventricle: Kian-Keong PohDocument33 pagesThe Dyssynchronous Ventricle: Kian-Keong PohcesareNo ratings yet
- Wide Complex Tachycardia Differentiation: A Reappraisal of The State-Of - The - ArtDocument9 pagesWide Complex Tachycardia Differentiation: A Reappraisal of The State-Of - The - ArtmikiNo ratings yet
- 10 1002@ejhf 769Document7 pages10 1002@ejhf 769Florescu VladimirNo ratings yet
- High Prevalence of Left Ventricular Systolic and Diastolic Asynchrony in Patients With Congestive Heart Failure and Normal QRS DurationDocument8 pagesHigh Prevalence of Left Ventricular Systolic and Diastolic Asynchrony in Patients With Congestive Heart Failure and Normal QRS DurationVashish RamrechaNo ratings yet
- Cardiac Resynchronization Therapy and Cardiac Contractility Modulation in Patients With Advanced Heart FailureDocument8 pagesCardiac Resynchronization Therapy and Cardiac Contractility Modulation in Patients With Advanced Heart FailuresunhaolanNo ratings yet
- 3 Badhwar ECG VTDocument29 pages3 Badhwar ECG VTdrsanjeevsenNo ratings yet
- 3.regression of Electrocardiographic Left VentricularDocument6 pages3.regression of Electrocardiographic Left VentricularGaal PinNo ratings yet
- 1 s2.0 S073510970502108X MainDocument10 pages1 s2.0 S073510970502108X MainAmelia Yulian SariNo ratings yet
- J HLC 2020 09 872Document2 pagesJ HLC 2020 09 872aswedi nersNo ratings yet
- Fragmented QRS Complex FrequencyDocument7 pagesFragmented QRS Complex FrequencyBinod KumarNo ratings yet
- Lin 2009Document7 pagesLin 2009Nur Syamsiah MNo ratings yet
- Kupo 2021Document9 pagesKupo 2021BözskeNo ratings yet
- Cardiac Resynchronization Therapy With His Bundle Pacing, 2018.Document7 pagesCardiac Resynchronization Therapy With His Bundle Pacing, 2018.Abel GarcíaNo ratings yet
- Alahmadi 2021Document21 pagesAlahmadi 2021NeaguNo ratings yet
- Euad 043Document29 pagesEuad 043Pedro SeguraNo ratings yet
- Swinkels Et Al - Effect of Aortic Cross-Clamp Time On LateDocument7 pagesSwinkels Et Al - Effect of Aortic Cross-Clamp Time On LateMurat MukharyamovNo ratings yet
- Samol2012 PDFDocument8 pagesSamol2012 PDFnaniro orinanNo ratings yet
- An Overview of Current Cardiac Resynchronization Therapy: Mini Forum For Heart Failure Acta Cardiol Sin 2013 29:496Document9 pagesAn Overview of Current Cardiac Resynchronization Therapy: Mini Forum For Heart Failure Acta Cardiol Sin 2013 29:496Andika Prasdipta HidayatNo ratings yet
- Circep 112 970939 PDFDocument7 pagesCircep 112 970939 PDFMostafizu Rrahman JhalakNo ratings yet
- Difference Vectors To Describe Dynamics of The ST Segment and The Ventricular Gradient in Acute IschemiaDocument10 pagesDifference Vectors To Describe Dynamics of The ST Segment and The Ventricular Gradient in Acute IschemiaComisión Académica FCM - UNAHNo ratings yet
- Archive of SID: New Correlation Between Angles of Wide Qrs Complex in Electrocardiogram and Echocardiographic IndicesDocument4 pagesArchive of SID: New Correlation Between Angles of Wide Qrs Complex in Electrocardiogram and Echocardiographic IndicesВиктор БебенинNo ratings yet
- Khalida - Clinical Significance of Early Repolarization On Long QT SyndromeDocument7 pagesKhalida - Clinical Significance of Early Repolarization On Long QT SyndromeraniakjsNo ratings yet
- 2007 - CAVI - Carotid Atherosclerosis - Pts With Essential Hypertension - HypertResDocument6 pages2007 - CAVI - Carotid Atherosclerosis - Pts With Essential Hypertension - HypertResMichail PapafaklisNo ratings yet
- Relationship Between Fragmented QRS Complex and Left Ventricular Systolic and Diastolic Function in Kidney Transplant PatientsDocument6 pagesRelationship Between Fragmented QRS Complex and Left Ventricular Systolic and Diastolic Function in Kidney Transplant PatientsMiguelNo ratings yet
- LBBBDocument4 pagesLBBBDolly JazmiNo ratings yet
- F QRSDocument9 pagesF QRSaisyah hamzakirNo ratings yet
- VT SVT AvrDocument3 pagesVT SVT AvragneselimNo ratings yet
- Epicardial ArrythmiasDocument9 pagesEpicardial ArrythmiasTor JaNo ratings yet
- Development of Robust, Fast and Efficient QRS Complex Detector: A Methodological ReviewDocument20 pagesDevelopment of Robust, Fast and Efficient QRS Complex Detector: A Methodological ReviewAllam Jaya PrakashNo ratings yet
- Fully Automated Method For QT Interval Measurement in ECG: October 2006Document5 pagesFully Automated Method For QT Interval Measurement in ECG: October 2006Cristina DragomirNo ratings yet
- Circimaging 112 975623Document10 pagesCircimaging 112 975623PanfilAlinaNo ratings yet
- QRS Interval - LITFL - ECG Library BasicsDocument10 pagesQRS Interval - LITFL - ECG Library Basicssilver silvaNo ratings yet
- Tachdjian 5Document8 pagesTachdjian 5Abrudan GabrielNo ratings yet
- Vereckei Criteria As A Diagnostic Tool Amongst Emergency Medicine Residents To Distinguish Between Ventricular Tachycardia and Supra-Ventricular Tachycardia With AberrancyDocument6 pagesVereckei Criteria As A Diagnostic Tool Amongst Emergency Medicine Residents To Distinguish Between Ventricular Tachycardia and Supra-Ventricular Tachycardia With AberrancyGading AuroraNo ratings yet
- 1 s2.0 073510979390233Q MainDocument10 pages1 s2.0 073510979390233Q MainSuryati HusinNo ratings yet
- Cardiac Resynchronization Therapy, Robotic LV Epicardial Lead Placement: Indications and TechniqueDocument34 pagesCardiac Resynchronization Therapy, Robotic LV Epicardial Lead Placement: Indications and TechniquedcicareNo ratings yet
- Agreement Between Manual and Automated Measurements of Simple QRS/T AngleDocument4 pagesAgreement Between Manual and Automated Measurements of Simple QRS/T AngleĐỗ Đăng KhoaNo ratings yet
- VT CriteriaDocument8 pagesVT CriterianitipatNo ratings yet
- Clinical Handbook of Cardiac ElectrophysiologyFrom EverandClinical Handbook of Cardiac ElectrophysiologyBenedict M. GloverNo ratings yet
- Discriminating Electrocardiographic Responses To His-Bundle Pacing Using Machine LearningDocument10 pagesDiscriminating Electrocardiographic Responses To His-Bundle Pacing Using Machine LearningMaria AlejandraNo ratings yet
- Journal of ElectrocardiologyDocument4 pagesJournal of ElectrocardiologyMaria AlejandraNo ratings yet
- Depooter 2017Document9 pagesDepooter 2017Maria AlejandraNo ratings yet
- Biomedical Signal Processing and ControlDocument8 pagesBiomedical Signal Processing and ControlMaria AlejandraNo ratings yet
- Courtney Connolly Critical Elements For Health Assessment Documentation HistoryDocument4 pagesCourtney Connolly Critical Elements For Health Assessment Documentation HistorycourtneyNo ratings yet
- Cardiac L3Document18 pagesCardiac L3Qutaybah JahmanyNo ratings yet
- DM 2022-0025 - Reiteration of The Policies To Ensure Adequacy of Hemodialysis Units For COVID-19 PatientsDocument2 pagesDM 2022-0025 - Reiteration of The Policies To Ensure Adequacy of Hemodialysis Units For COVID-19 PatientsAbigael VianaNo ratings yet
- CHE 243 MODIFIED ESSENTIAL NEWBORN CAREDocument35 pagesCHE 243 MODIFIED ESSENTIAL NEWBORN CAREabubakarauwal690No ratings yet
- Valvular Heart DiseaseDocument32 pagesValvular Heart DiseaseyunielsyaNo ratings yet
- HRCT Protocols & Artifacts: Leena. R. David M.SC - MITDocument24 pagesHRCT Protocols & Artifacts: Leena. R. David M.SC - MITNadeem ShahNo ratings yet
- Disease Signs and Symptoms Deficiency/Problem Notes AmyloidosisDocument14 pagesDisease Signs and Symptoms Deficiency/Problem Notes AmyloidosisSriKavya DevineniNo ratings yet
- Pricelist November2021Document20 pagesPricelist November2021Apotek C 8No ratings yet
- A Study On Impact of Acne Vulgaris On Quality of LifeDocument7 pagesA Study On Impact of Acne Vulgaris On Quality of LifeIJAR JOURNALNo ratings yet
- Immunization PDFDocument23 pagesImmunization PDFعبدالرحمن علىNo ratings yet
- Medicalcertificate: Locsin ST, Molo, Iloilo City, 5000 Iloilo TelDocument1 pageMedicalcertificate: Locsin ST, Molo, Iloilo City, 5000 Iloilo TelMixedTvNo ratings yet
- Classification Based On Biosafety LevelDocument2 pagesClassification Based On Biosafety LevelKitty OrtxNo ratings yet
- Am, VK, EoDocument18 pagesAm, VK, EoBritney ClaireNo ratings yet
- Hadpsar List Corentine 25.03.20Document10 pagesHadpsar List Corentine 25.03.20snagoorNo ratings yet
- Burns E 2013 PHD Thesis PDFDocument338 pagesBurns E 2013 PHD Thesis PDFDr-Rabia AlmamalookNo ratings yet
- Solanum - Zombiepedia - FandomDocument5 pagesSolanum - Zombiepedia - FandomJohn SutphinNo ratings yet
- Miniguia de EstudosDocument6 pagesMiniguia de EstudosMaykom LiraNo ratings yet
- Community MedicineDocument7 pagesCommunity MedicinePavithra S 1 8 2001No ratings yet
- Furman 2013 Vestibular MigraineDocument10 pagesFurman 2013 Vestibular MigraineJuan Hernández GarcíaNo ratings yet
- Just Another Sebaceous Cyst?: I. Clinical QuestionDocument3 pagesJust Another Sebaceous Cyst?: I. Clinical QuestionJaessa FelicianoNo ratings yet
- 2022 - JCEM - RS Supporting The Hypercalcemia of Malignancy GuidelinesDocument7 pages2022 - JCEM - RS Supporting The Hypercalcemia of Malignancy GuidelinesLuiz Fernando Fonseca VieiraNo ratings yet
- Uspi LomotilDocument8 pagesUspi LomotilhaiduvnNo ratings yet
- New-DLP Phase2 Assignment-4 Module-B Final-9.8.18Document6 pagesNew-DLP Phase2 Assignment-4 Module-B Final-9.8.18PNo ratings yet
- Duttons Introductory Skills and Procedures For The Physical Therapist Assistant 1St Edition Mark Dutton Full ChapterDocument51 pagesDuttons Introductory Skills and Procedures For The Physical Therapist Assistant 1St Edition Mark Dutton Full Chaptersusie.blankenship630100% (6)
- Arakaki 2017Document8 pagesArakaki 2017Gabriella Kezia LiongNo ratings yet
- Pablo GarciaDocument3 pagesPablo GarciaCygrusNo ratings yet