Download as pdf or txt
You might also like
- 27 Adbri Masonry Versaloc TechnicalDocument24 pages27 Adbri Masonry Versaloc TechnicalSteveMateNo ratings yet
- Ziehm Solo FD Service ManualDocument442 pagesZiehm Solo FD Service Manualdrakon100% (1)
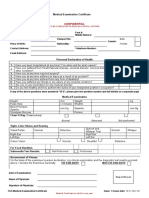
- Medical Examination Certificate: ConfidentialDocument2 pagesMedical Examination Certificate: ConfidentialVioleta100% (1)
- Manual Lab Results Daddy Peds CbcASDDocument12 pagesManual Lab Results Daddy Peds CbcASDJohn Benedict LascunaNo ratings yet
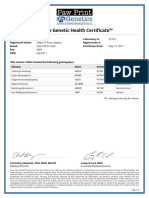
- Legolas Genetic Health CertificateDocument1 pageLegolas Genetic Health Certificateapi-522868583No ratings yet
- Strahlenfolter Stalking - TI - V2K - RNM Remote Neural Monitoring Satellite Terrorism - October 2010 - Satelliteterrorism3.Blogspot - deDocument5 pagesStrahlenfolter Stalking - TI - V2K - RNM Remote Neural Monitoring Satellite Terrorism - October 2010 - Satelliteterrorism3.Blogspot - deKurt-Schneider50% (2)
- DARPA Accomplishments Vol 2Document410 pagesDARPA Accomplishments Vol 2sunburngr100% (1)
- Studi Kasus SCMDocument8 pagesStudi Kasus SCMMuflihul Khair0% (5)
- Trim Clean 2030-Msds (Bld-1656 v1)Document8 pagesTrim Clean 2030-Msds (Bld-1656 v1)Tri Febrianto PamungkasNo ratings yet
- Thal - DNA Analysis Request Consent Form - Version 4.1 Issued 03 Jan 2023 With BI ConsentDocument2 pagesThal - DNA Analysis Request Consent Form - Version 4.1 Issued 03 Jan 2023 With BI ConsentZalina ZamirayyanNo ratings yet
- Cytogenetic Findings in Patients With Intellectual Disability And/or Multiple Congenital AnomaliesDocument7 pagesCytogenetic Findings in Patients With Intellectual Disability And/or Multiple Congenital Anomaliesshf.mxlikNo ratings yet
- TRN2044095 7939696 Clinical ReportDocument10 pagesTRN2044095 7939696 Clinical ReportWARNET SANTONo ratings yet
- Advt For Fellowship in Clinical Genetics 01.07.2019 0Document8 pagesAdvt For Fellowship in Clinical Genetics 01.07.2019 0m nNo ratings yet
- TRN2044041 7939695 Clinical ReportDocument10 pagesTRN2044041 7939695 Clinical ReportWARNET SANTONo ratings yet
- Brain 123Document58 pagesBrain 123rahafNo ratings yet
- Birth Defectscreening Webiner 2024Document62 pagesBirth Defectscreening Webiner 2024Debasish SarkarNo ratings yet
- Battaglia 2013Document11 pagesBattaglia 2013ОльгаЛевченкоNo ratings yet
- Format Pre EmploymentDocument10 pagesFormat Pre EmploymentNurman HidayatNo ratings yet
- KAL24061100Document2 pagesKAL24061100Tanisha DadhichNo ratings yet
- MTPC 137 Case StudyDocument8 pagesMTPC 137 Case StudyJoe-ali ManampanNo ratings yet
- A Manual of Laboratory Techniques in Clinical Hematology 1Document15 pagesA Manual of Laboratory Techniques in Clinical Hematology 1Jaycel Mae Ba-ay (Gaikokujinn)No ratings yet
- Detection of Deletions at 7q11.23 in Williams-BeurenDocument6 pagesDetection of Deletions at 7q11.23 in Williams-BeurenAmisadai ArévaloNo ratings yet
- YSF24043407Document2 pagesYSF24043407Sachin KumarNo ratings yet
- XX063Document3 pagesXX063BittuNo ratings yet
- URINALYSISDocument1 pageURINALYSISMaymay PalmaNo ratings yet
- HM Medical Checkups at Project Sites Medical CampsDocument2 pagesHM Medical Checkups at Project Sites Medical Campsraj kumariNo ratings yet
- Biological Variations Technical StabilitDocument8 pagesBiological Variations Technical StabilitOumar SourabieNo ratings yet
- Congenital Cataract Clinical Proforma: Clinical ProformaDocument2 pagesCongenital Cataract Clinical Proforma: Clinical ProformaAsmat Khan UFzNo ratings yet
- 2018 Ghaffari AnnHumGenetDocument8 pages2018 Ghaffari AnnHumGenetEAPNo ratings yet
- Problem CardsDocument12 pagesProblem CardsBahnishikha GhoshNo ratings yet
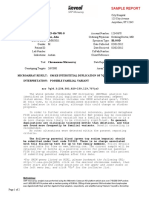
- Sample Report Reveal Pediatric VOUS 072512Document2 pagesSample Report Reveal Pediatric VOUS 072512saipavani kummaraguntlaNo ratings yet
- PM - NaceDocument3 pagesPM - Nacemohammad tahirNo ratings yet
- Skrening - Deteksi Dini ThalassemiaDocument29 pagesSkrening - Deteksi Dini ThalassemiapasebatNo ratings yet
- Karyotyping LabDocument8 pagesKaryotyping LabVarit SuriyasomboonNo ratings yet
- Histopathology Requisition FormDocument2 pagesHistopathology Requisition Formr4raheNo ratings yet
- HMFBPDocument2 pagesHMFBPainihzrhNo ratings yet
- Clinical Genetics - 2015 - Palmer - New Insights Into Brunner Syndrome and Potential For Targeted TherapyDocument8 pagesClinical Genetics - 2015 - Palmer - New Insights Into Brunner Syndrome and Potential For Targeted Therapysilaaturann8No ratings yet
- Glucose, Fasting (FBS) : Req. No: 031903144201Document17 pagesGlucose, Fasting (FBS) : Req. No: 031903144201SRIPERAMBHUDURI KRISHNANo ratings yet
- Homoeopathic Case Interview ProformaDocument9 pagesHomoeopathic Case Interview ProformaAmit Singh PalNo ratings yet
- CCG - Genomic Testing Request FormDocument6 pagesCCG - Genomic Testing Request Formapi-644140941No ratings yet
- Genetic Testing ReviewDocument5 pagesGenetic Testing ReviewVaishnavi KawthankarNo ratings yet
- IMPORTANT: The Original of This Form Is To Be Kept by The Seafarer. A Copy Must Be Kept by The ClinicDocument2 pagesIMPORTANT: The Original of This Form Is To Be Kept by The Seafarer. A Copy Must Be Kept by The ClinicTigreal MLNo ratings yet
- Post Graduate ClinicsDocument113 pagesPost Graduate ClinicsSnehal PatilNo ratings yet
- Lab Report - 040767-2122 - 1Document1 pageLab Report - 040767-2122 - 1Muhammad ImranNo ratings yet
- Case Study 9Document11 pagesCase Study 9Angel MayNo ratings yet
- Patient Report Direct ViewDocument2 pagesPatient Report Direct ViewSyed Tahir BukhariNo ratings yet
- Mowat Wilson SyndromeDocument25 pagesMowat Wilson SyndromeVikash SharmaNo ratings yet
- Milan Jena ReportDocument1 pageMilan Jena Reportmridhatapas2No ratings yet
- Epidemiology and Etiology of Infantile Developmental andDocument8 pagesEpidemiology and Etiology of Infantile Developmental andyavuzatas23No ratings yet
- Basics of Practical Genetics: Workbook I Course International Medical Faculty GroupDocument16 pagesBasics of Practical Genetics: Workbook I Course International Medical Faculty GroupNehaNo ratings yet
- Sars-Cov-2 (Qualitative RTPCR) : Nasopharyngeal / Oropharyngeal SwabDocument2 pagesSars-Cov-2 (Qualitative RTPCR) : Nasopharyngeal / Oropharyngeal SwabNaushadNo ratings yet
- Tema 4Document13 pagesTema 4Nerea OteguiNo ratings yet
- 使用染色体微阵列和外显子组测序对有孤立和非分离性先天性心脏缺陷的胎儿进行产前诊断Prenat DiagnDocument8 pages使用染色体微阵列和外显子组测序对有孤立和非分离性先天性心脏缺陷的胎儿进行产前诊断Prenat DiagnchenziendrNo ratings yet
- A Case Study of G2 P1 (2023) of 35 2/7 Weeks Aog by Normal Spontaneously Vaginal Delivery To A Live Baby GirlDocument19 pagesA Case Study of G2 P1 (2023) of 35 2/7 Weeks Aog by Normal Spontaneously Vaginal Delivery To A Live Baby GirlMikes CastroNo ratings yet
- CMA Quick Facts: Genomic Tools: Chromosomal MicroarrayDocument1 pageCMA Quick Facts: Genomic Tools: Chromosomal MicroarrayNational Coalition for Health Professional Education in GeneticsNo ratings yet
- Medical Examintation Report: Document No MTIPL/HR/F0006 1Document1 pageMedical Examintation Report: Document No MTIPL/HR/F0006 1Kabir ShelkeNo ratings yet
- A5vn52dev5p3ydx510txlxeuDocument2 pagesA5vn52dev5p3ydx510txlxeuRAVINDERNo ratings yet
- Antenatal Assessment ToolDocument13 pagesAntenatal Assessment ToolBlessy MadhuriNo ratings yet
- Identification, Evaluation and Comparative Assessment of Apoptotic Cells in Oral Epithelium of Pre Malignant Lesion andDocument7 pagesIdentification, Evaluation and Comparative Assessment of Apoptotic Cells in Oral Epithelium of Pre Malignant Lesion andcdcrioralpathNo ratings yet
- Clinical Biochemistry: Mrs Seema JainDocument10 pagesClinical Biochemistry: Mrs Seema JainAnkit Jain chinese interpreterNo ratings yet
- History Taking in Clinical OphthalmologyDocument12 pagesHistory Taking in Clinical OphthalmologykarkitjainaadaniNo ratings yet
- Pathology Urine Complete Examination: Albumin Sugar (R) Bile Salts Bile PigmentsDocument1 pagePathology Urine Complete Examination: Albumin Sugar (R) Bile Salts Bile PigmentsGuru KathirNo ratings yet
- Case Study Patient SLDocument23 pagesCase Study Patient SLAbby AusteroNo ratings yet
- Prenatal Aneuploidy ScreeningDocument80 pagesPrenatal Aneuploidy ScreeningBharti Pant GahtoriNo ratings yet
- DownloadDocument10 pagesDownloadmandapatiNo ratings yet
- Genetic Disorders and the Fetus: Diagnosis, Prevention, and TreatmentFrom EverandGenetic Disorders and the Fetus: Diagnosis, Prevention, and TreatmentNo ratings yet
- If You Are Tested If You Are Tested Covid-19 Positive and Instructed To Be and Instructed To Be Quarantined at Home ,, You ShouldDocument4 pagesIf You Are Tested If You Are Tested Covid-19 Positive and Instructed To Be and Instructed To Be Quarantined at Home ,, You ShouldRicardanteNo ratings yet
- Crochetage Sign: An Invaluable Independent ECG Sign in Detecting ASDDocument2 pagesCrochetage Sign: An Invaluable Independent ECG Sign in Detecting ASDRicardanteNo ratings yet
- To The Requesting Lab / Person, Please Stamp HereDocument4 pagesTo The Requesting Lab / Person, Please Stamp HereRicardanteNo ratings yet
- Approaches To Clinical Case PresentationDocument15 pagesApproaches To Clinical Case PresentationRicardanteNo ratings yet
- Sonia Thakker 184 Jignesh Bhatt 105 Rekha Wachkawde 188 Shailendra Singh 178 Pravin Nayak 147 Jibu James 128Document44 pagesSonia Thakker 184 Jignesh Bhatt 105 Rekha Wachkawde 188 Shailendra Singh 178 Pravin Nayak 147 Jibu James 128treakoNo ratings yet
- TechNote CableModellingDocument12 pagesTechNote CableModellingLeonardo LeonNo ratings yet
- Service Manual: No. SEB-83ACEDocument129 pagesService Manual: No. SEB-83ACEThein Htoon lwin100% (3)
- ControlDocument58 pagesControlRobinson CardenasNo ratings yet
- Dance VolumeDocument11 pagesDance VolumeuiuiuiuNo ratings yet
- Soal Bahasa Inggris Kelas Xii Semua JurusanDocument13 pagesSoal Bahasa Inggris Kelas Xii Semua Jurusaneka sanjayaNo ratings yet
- Eurocode Conference 2023 Pluijm Van Der Eurocode 6Document14 pagesEurocode Conference 2023 Pluijm Van Der Eurocode 6Rodolfo BlanchiettiNo ratings yet
- Analisis Potensi Dan Tingkat Pemanfaatan Sumberdaya Ikan Di Perairan Kabupaten Bangka SelatanDocument12 pagesAnalisis Potensi Dan Tingkat Pemanfaatan Sumberdaya Ikan Di Perairan Kabupaten Bangka SelatanShope IkmaNo ratings yet
- Up ListDocument200 pagesUp Listprashant guptaNo ratings yet
- Motor Circuit Analysis For Energy, Reliability and Production Cost ImprovementsDocument4 pagesMotor Circuit Analysis For Energy, Reliability and Production Cost ImprovementsAmin Mustangin As-SalafyNo ratings yet
- Worksheet - Orbital Diagrams - TeacherDocument2 pagesWorksheet - Orbital Diagrams - Teacherdela2100% (3)
- Unit Two. Dominant Theories Approaches: Positivism Rational Choice Theory MarxismDocument8 pagesUnit Two. Dominant Theories Approaches: Positivism Rational Choice Theory MarxismPaul RicoNo ratings yet
- GCRP TX InterruptionDocument13 pagesGCRP TX InterruptionPanNo ratings yet
- English FinalDocument71 pagesEnglish FinalKhadeeja MarjanNo ratings yet
- Adriafil SummerDocument5 pagesAdriafil SummerTatu AradiNo ratings yet
- CROSS REFERENCE DE VALVULAS SOLENOIDES - Danfoss - Alco - Sporlan-ParkerDocument4 pagesCROSS REFERENCE DE VALVULAS SOLENOIDES - Danfoss - Alco - Sporlan-ParkerJoss CastellNo ratings yet
- BusDocument24 pagesBusSyed Noman AhmedNo ratings yet
- Samsung Galaxy S22 Ultra 5G - Full Phone SpecificationsDocument13 pagesSamsung Galaxy S22 Ultra 5G - Full Phone SpecificationsAb BossNo ratings yet
- Lesson Plan Format (Acad)Document4 pagesLesson Plan Format (Acad)Aienna Lacaya MatabalanNo ratings yet
- Music Therapy When Death Is Imminent - A Phenomenological InquiryDocument32 pagesMusic Therapy When Death Is Imminent - A Phenomenological InquiryJuan Luis Köstner MartinoNo ratings yet
- Class 9 - ScienceDocument228 pagesClass 9 - ScienceYashwanth KasturiNo ratings yet
- Railway Ballast PerformanceDocument27 pagesRailway Ballast PerformanceSamuel Carlos Sanjuán TorresNo ratings yet
- MN402 01Document22 pagesMN402 01UnknownNo ratings yet
- Pressure Relief Valve, Pilot-OperatedDocument52 pagesPressure Relief Valve, Pilot-OperatedAlvaro YépezNo ratings yet