Download as docx, pdf, or txt
You might also like
- Guide To Nursing Management and Leadership 8th Edition Tomey Test BankDocument9 pagesGuide To Nursing Management and Leadership 8th Edition Tomey Test BankJillianMontoyasepza100% (13)
- Hotel Incident ReportDocument2 pagesHotel Incident ReportApirinmu100% (8)
- Time Management Self-AssessmentDocument4 pagesTime Management Self-Assessmenthasithlakashan67% (3)
- Vitamins VM0822Document57 pagesVitamins VM0822fdfsdfNo ratings yet
- JSA - Mechanical-Excavation PDFDocument1 pageJSA - Mechanical-Excavation PDFAhmed GomaaNo ratings yet
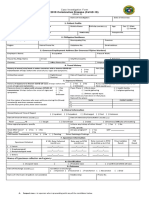
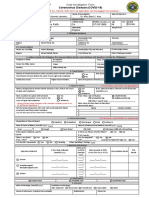
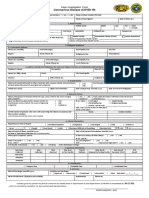
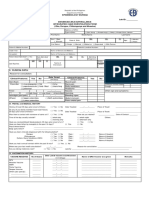
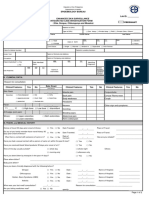
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument4 pagesCoronavirus Disease (COVID-19) : Case Investigation FormMaria JoselaNo ratings yet
- Pre Employment Medical Form PDFDocument1 pagePre Employment Medical Form PDFKristina Miller100% (1)
- Las Piñas CIFDocument1 pageLas Piñas CIFchrisNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormMizraim TupazNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormPresinto Dos Parañaque KnightsNo ratings yet
- New Cif FormDocument2 pagesNew Cif FormNovie FeneciosNo ratings yet
- CoViD19-Covid Investigation FormDocument1 pageCoViD19-Covid Investigation FormMc Arem PaghunasanNo ratings yet
- CoViD19-CIF-v6-Fillable QCv3-2Document1 pageCoViD19-CIF-v6-Fillable QCv3-2Patrice De CastroNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormJudeLaxNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormShiela E. EladNo ratings yet
- CIF TemplateDocument2 pagesCIF Templateluvaire23No ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormChamee MallillinNo ratings yet
- Coronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalDocument1 pageCoronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalKarsenley Cal-el Iddig BurigsayNo ratings yet
- DOH PIDSR COVID-19 CIF TemplateDocument1 pageDOH PIDSR COVID-19 CIF TemplateMargaux Faith CCNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormHerbert Tierra Ponce Jr.100% (1)
- Case Lnvestigation FormDocument3 pagesCase Lnvestigation FormChum ChitaruNo ratings yet
- Saric CifDocument1 pageSaric CifMarav SymbNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormBabiejoy Beltran AceloNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormBabiejoy Beltran AceloNo ratings yet
- Arrival Card in PH 1Document2 pagesArrival Card in PH 1gleric custodioNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormmaelisaNo ratings yet
- Health Declaration Form: Applicant ProfileDocument1 pageHealth Declaration Form: Applicant ProfileOnyx XynoNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormChum ChitaruNo ratings yet
- CIF (For BMDL PhilHealth Purposes Only)Document1 pageCIF (For BMDL PhilHealth Purposes Only)BALIUAG DISTRICT LABORATORYNo ratings yet
- Philippine Integrated Disease Surveillance and Response: 14 DaysDocument1 pagePhilippine Integrated Disease Surveillance and Response: 14 DaysAlpha BatteryNo ratings yet
- Zika IcifDocument2 pagesZika IcifMarav SymbNo ratings yet
- Fwri Cif FormDocument3 pagesFwri Cif FormMHO GloriaNo ratings yet
- COVID 19 Form 1 1 PDFDocument1 pageCOVID 19 Form 1 1 PDFTuguinay EmilynNo ratings yet
- Annex 2i Investigation Form 29092020Document6 pagesAnnex 2i Investigation Form 29092020nik mohamad zulfikriNo ratings yet
- FWRI Form ReviseDocument3 pagesFWRI Form ReviseJm uniteNo ratings yet
- Viral Haemorrhagic Fever - Case Reporting Form IDSR Viral Hemorrhagic Fever Case Report FormDocument1 pageViral Haemorrhagic Fever - Case Reporting Form IDSR Viral Hemorrhagic Fever Case Report FormSalihu MustaphaNo ratings yet
- Contact Listing Form: (For Investigation Team)Document4 pagesContact Listing Form: (For Investigation Team)Dristhi ShresthaNo ratings yet
- FWRI 2023 CIF v2Document3 pagesFWRI 2023 CIF v2Terence John ChebatNo ratings yet
- Chikungunya FormDocument2 pagesChikungunya FormTin Causaren-Gertos100% (1)
- Released: Sunpower Philippines Medical Screening Form (MSF)Document2 pagesReleased: Sunpower Philippines Medical Screening Form (MSF)glenn dalesNo ratings yet
- Dr. Eutiquio Ll. Atanacio Jr. Memorial Hospital, Inc: DOH-EB-AEHMD-FWRIPIS-2021-0Document3 pagesDr. Eutiquio Ll. Atanacio Jr. Memorial Hospital, Inc: DOH-EB-AEHMD-FWRIPIS-2021-0deamhi nursing serviceNo ratings yet
- Health Declaration FormDocument12 pagesHealth Declaration FormAmelia Delos ReyesNo ratings yet
- New Enhanced Zika CIFDocument3 pagesNew Enhanced Zika CIFMarav SymbNo ratings yet
- CIF PertussisDocument2 pagesCIF PertussisDan Joseph AguilarNo ratings yet
- Self Declaration Form MeluhaDocument1 pageSelf Declaration Form MeluhaSandy BergerNo ratings yet
- Laboratory Requisition Form 18062021Document2 pagesLaboratory Requisition Form 18062021Sanja KostićNo ratings yet
- ESR Verification Form ReviseDocument4 pagesESR Verification Form ReviseRouella DoverteNo ratings yet
- CIF DiphDocument2 pagesCIF DiphIvy marie BonNo ratings yet
- FinalclaimDocument12 pagesFinalclaimSatyam TiwariNo ratings yet
- Health Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiDocument2 pagesHealth Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiCoin CharNo ratings yet
- Guests DeclarationDocument2 pagesGuests DeclarationRuddy NaranjoNo ratings yet
- Joining InstructionsDocument5 pagesJoining InstructionsCraftyZaidNo ratings yet
- DeputationProforma PDFDocument3 pagesDeputationProforma PDFPratap YedlaNo ratings yet
- Discharge Planning TBDocument2 pagesDischarge Planning TBNurida LatipahNo ratings yet
- CT-FORM-BLANKDocument3 pagesCT-FORM-BLANKArce RostumNo ratings yet
- TRF For COVID-19 TEST (Coronavirus) : History Yes NoDocument1 pageTRF For COVID-19 TEST (Coronavirus) : History Yes NoRajendra ChavanNo ratings yet
- Accident or Dangerous Incident Report FormDocument4 pagesAccident or Dangerous Incident Report FormFNo ratings yet
- Medical Survey: Covid-19 Tests: RT-PCR - Rapid Antigen - SerologicDocument1 pageMedical Survey: Covid-19 Tests: RT-PCR - Rapid Antigen - SerologicSales DptNo ratings yet
- Death Claim Doctor'S Statement: Symptoms Presented at First Consultation Date Symptoms First Started (DD/MM/YY)Document2 pagesDeath Claim Doctor'S Statement: Symptoms Presented at First Consultation Date Symptoms First Started (DD/MM/YY)onlineNo ratings yet
- Group Health - Claim FormDocument6 pagesGroup Health - Claim FormSubhash SharmaNo ratings yet
- F001 OP R Encoding SheetDocument2 pagesF001 OP R Encoding SheetAnnalien AlaanNo ratings yet
- AEFI Reporting Form en Jan2016Document2 pagesAEFI Reporting Form en Jan2016madhuNo ratings yet
- CT Form BlankDocument3 pagesCT Form BlankArce RostumNo ratings yet
- Case Investigation Form: DiphtheriaDocument3 pagesCase Investigation Form: DiphtheriaSalihu MustaphaNo ratings yet
- Good' Food Islamic Food Ethics Beyond Religious Dietary LawsDocument16 pagesGood' Food Islamic Food Ethics Beyond Religious Dietary Lawsnovi diyantoNo ratings yet
- Prac Res Q2 Module 8Document12 pagesPrac Res Q2 Module 8Benicel Lane De VeraNo ratings yet
- Presentation: Submitted To Ma'am Ayesha Sadaf Subject Media & SocietyDocument23 pagesPresentation: Submitted To Ma'am Ayesha Sadaf Subject Media & Societylaiba asadNo ratings yet
- Star Comprehensive BrochureDocument1 pageStar Comprehensive BrochureShakti ShivanandNo ratings yet
- Health Hunters: Expect The UnexpectedDocument8 pagesHealth Hunters: Expect The UnexpectedConciencia CristalinaNo ratings yet
- P3-F Grammar Revision For MidyearDocument10 pagesP3-F Grammar Revision For MidyearnewtonelifNo ratings yet
- Sustainable Development Goal 2 - Zero HungerDocument11 pagesSustainable Development Goal 2 - Zero HungeralomerdenisNo ratings yet
- 21 Advanced Supplements Antihistamines Mast Cell StabilizersDocument18 pages21 Advanced Supplements Antihistamines Mast Cell Stabilizersdarija_ilic100% (1)
- Digital Studio: Course DescriptionDocument12 pagesDigital Studio: Course DescriptionCornNo ratings yet
- MYTHDocument6 pagesMYTHCherian MominNo ratings yet
- The Dynamics of Psychological Security-Insecurity: Brooklyn CollegeDocument15 pagesThe Dynamics of Psychological Security-Insecurity: Brooklyn Collegetanisya aurely12No ratings yet
- The Effect of Work-Family Conflict On Job Satisfaction Among School Teachers in ErodeDocument4 pagesThe Effect of Work-Family Conflict On Job Satisfaction Among School Teachers in ErodeDiwya Bharathi V I MBANo ratings yet
- Marram Email BrochureDocument5 pagesMarram Email Brochurethangth1986No ratings yet
- Implementation of The African Charter On The Rights and Welfare of The Child in UgandaDocument52 pagesImplementation of The African Charter On The Rights and Welfare of The Child in UgandashjahsjanshaNo ratings yet
- A. A. A. Abdel-KareemDocument17 pagesA. A. A. Abdel-KareemDRHAMADA ELWANNo ratings yet
- CIDP Kitui - 2013-2017Document424 pagesCIDP Kitui - 2013-2017Wilson MuguroNo ratings yet
- Classification and Coding of NeoplasmsDocument18 pagesClassification and Coding of NeoplasmsNajmul HasanNo ratings yet
- Genu ValgumDocument5 pagesGenu Valgumtjr845sjvbNo ratings yet
- Republic of The Philippines Region VII Central Visayas Division of Cebu Province Tambongon, San Remegio, CebuDocument7 pagesRepublic of The Philippines Region VII Central Visayas Division of Cebu Province Tambongon, San Remegio, CebuLenie PelegrinNo ratings yet
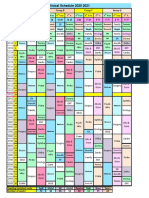
- R Schedule 2020 2021Document1 pageR Schedule 2020 2021Mohammed AhmedNo ratings yet
- Egyptian Stories - Egypt Bottled Water - UNSAFEDocument4 pagesEgyptian Stories - Egypt Bottled Water - UNSAFEtefovNo ratings yet
- Bathroom Wordlist: Bath Brush Comb MirrorDocument1 pageBathroom Wordlist: Bath Brush Comb MirrorQuyetNo ratings yet
- Chapter 2 - Market Analysis - Group 2Document26 pagesChapter 2 - Market Analysis - Group 2Allan AntonioNo ratings yet
- What Is A Competent TeacherDocument2 pagesWhat Is A Competent TeacherJoy Dacuan100% (2)
- Wolford EDM511 Case 4Document10 pagesWolford EDM511 Case 4geraldwolford1No ratings yet