Download as docx, pdf, or txt
You might also like
- Fibrocystic Breast DiseaseDocument3 pagesFibrocystic Breast Diseasebadshah007777No ratings yet
- Lec#17 Benign Breast ConditionsDocument67 pagesLec#17 Benign Breast ConditionsBalqees abusahuonNo ratings yet
- Group3 11Document18 pagesGroup3 11Lacangan, Thea YvonneNo ratings yet
- Breast DiseasesDocument47 pagesBreast DiseasesDR/ AL-saifiNo ratings yet
- Mammography. NotesDocument9 pagesMammography. Notescorrainnejimenez.24No ratings yet
- Unit 1 - Breast Anatomy and PhysiologyDocument50 pagesUnit 1 - Breast Anatomy and PhysiologyClyde R.OrtegaNo ratings yet
- Case Study MastectomyDocument26 pagesCase Study MastectomyIcheAnne Nilay100% (2)
- MastectomyDocument52 pagesMastectomyCogie SalvadorNo ratings yet
- Benign & Malignant Breast Lesions Presented By: Omar Al. Ma'aita Mais Al - Shboul 6 Year, Surgery Course, J.U.S.TDocument87 pagesBenign & Malignant Breast Lesions Presented By: Omar Al. Ma'aita Mais Al - Shboul 6 Year, Surgery Course, J.U.S.TRussia Al Shboul100% (1)
- NCM 106Document13 pagesNCM 106Calimlim KimNo ratings yet
- Screening of Breast CancerDocument19 pagesScreening of Breast CancerIncredible DivineNo ratings yet
- Breast DisorderDocument89 pagesBreast DisorderYang TayengNo ratings yet
- LP Tumor Mamae OkDocument13 pagesLP Tumor Mamae OkDiban namiNo ratings yet
- Case Study 1Document7 pagesCase Study 1Keir Mrls ForcadillaNo ratings yet
- An Overview of Breast Cancer: Presented by Group IVDocument76 pagesAn Overview of Breast Cancer: Presented by Group IVifcrstarsNo ratings yet
- Case Study About Cervical CancerDocument11 pagesCase Study About Cervical CancerJisel-Apple Bulan100% (1)
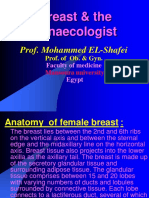
- Breast & The Gynaecologist: Prof. Mohammed EL-ShafeiDocument17 pagesBreast & The Gynaecologist: Prof. Mohammed EL-ShafeiAhmed BassettNo ratings yet
- Assessing BreastDocument42 pagesAssessing BreastKara Kristine TuanoNo ratings yet
- 4 1Document265 pages4 1sillypoloNo ratings yet
- Assessing Breasts and Lymphatic SystemDocument5 pagesAssessing Breasts and Lymphatic SystemGiselle EstoquiaNo ratings yet
- Breast: Anatomy & PhysiologyDocument6 pagesBreast: Anatomy & PhysiologyironNo ratings yet
- Affinity of Homoeopathic Drugs in Cases of FibroadenomaDocument5 pagesAffinity of Homoeopathic Drugs in Cases of FibroadenomaMohini GhãÑghàsNo ratings yet
- Breast Cancer: Case ReviewDocument10 pagesBreast Cancer: Case Reviewirma suwandi sadikinNo ratings yet
- Anatomy and Physiology of The BreastDocument42 pagesAnatomy and Physiology of The BreastNicole SooNo ratings yet
- Module 1 - Breast Anatomy and Mammographic CorrelationDocument31 pagesModule 1 - Breast Anatomy and Mammographic CorrelationAndrei YabutNo ratings yet
- The BreastsDocument20 pagesThe BreastsAmeer MattaNo ratings yet
- Breast CancerDocument27 pagesBreast CancerJils SureshNo ratings yet
- Gynaecology NotesDocument175 pagesGynaecology NotesNathaniel Mbiu TimNo ratings yet
- ENDOMETRIOMADocument8 pagesENDOMETRIOMAJennine ReyesNo ratings yet
- Reproduction PPT 7 MAMMARY GLANDSDocument23 pagesReproduction PPT 7 MAMMARY GLANDSlisanames.23No ratings yet
- Breast Lump-Nipple Disch Mastalgia Case ScenariosDocument34 pagesBreast Lump-Nipple Disch Mastalgia Case Scenariossamakashif1No ratings yet
- 1.anatomi MammaeDocument15 pages1.anatomi MammaeKatou Jeffrey ShigehitoNo ratings yet
- Case Presentation Group CDocument65 pagesCase Presentation Group CRea Jane Astrologo PastorNo ratings yet
- OB Nursing ProcessDocument26 pagesOB Nursing Processapi-38225080% (1)
- C2015 Medjur Finals Reviewer (Gumpal)Document71 pagesC2015 Medjur Finals Reviewer (Gumpal)Rad IsnaniNo ratings yet
- Mastectomy Power PointDocument63 pagesMastectomy Power PointokaciaNo ratings yet
- Male and Female Reproductive SystemDocument79 pagesMale and Female Reproductive SystemNaveen ChNo ratings yet
- Laparoscopic Management of Giant Ovarian Cyst A Case ReportDocument3 pagesLaparoscopic Management of Giant Ovarian Cyst A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- MAC11656Womb-E9 Endometrial CancerDocument106 pagesMAC11656Womb-E9 Endometrial Cancerjhon heriansyahNo ratings yet
- PBL 3 Breast CancerDocument17 pagesPBL 3 Breast Cancerนีล ไบรอันNo ratings yet
- Breast AnatomyDocument53 pagesBreast AnatomyShriniwas RushiNo ratings yet
- Breast Cancer: Pathophysiology What Is It All About?Document1 pageBreast Cancer: Pathophysiology What Is It All About?Kathleen VargasNo ratings yet
- Lesson Plan On Breast CancerDocument12 pagesLesson Plan On Breast CancerManisha DavidNo ratings yet
- Open Breast Disorders (Benign and Malignant) DoneDocument117 pagesOpen Breast Disorders (Benign and Malignant) Donereema.saleh123No ratings yet
- 2018.03.02 - Dr. Iwan - Breast Cancer 1Document102 pages2018.03.02 - Dr. Iwan - Breast Cancer 1SuryooNo ratings yet
- Female Reproductive System: Praktikum KBK Semester VDocument44 pagesFemale Reproductive System: Praktikum KBK Semester VXeniel AlastairNo ratings yet
- Ultrasound Breast ScanningDocument36 pagesUltrasound Breast ScanningPhuntsho Ongmo100% (1)
- Subject-Obstretic and Gyanecology: Ashoka Institute of Nursing, PatialaDocument16 pagesSubject-Obstretic and Gyanecology: Ashoka Institute of Nursing, PatialaRamandeep KaurNo ratings yet
- 3 - Anatomy Presentation NotesDocument43 pages3 - Anatomy Presentation Notesonezwa1992No ratings yet
- Fam New 4Document5 pagesFam New 4novaNo ratings yet
- Breast Anatomy For The Interventionalist: Robert A. Jesinger, MD, MSEDocument7 pagesBreast Anatomy For The Interventionalist: Robert A. Jesinger, MD, MSErasminojNo ratings yet
- Physical Examination-BREAST: Health Assessment - LectureDocument10 pagesPhysical Examination-BREAST: Health Assessment - LectureJunghoon YangParkNo ratings yet
- Breast: Baconga, KeziahDocument153 pagesBreast: Baconga, KeziahPaul Valdez100% (2)
- Breast Lumps Part 1Document55 pagesBreast Lumps Part 1Umar AzlanNo ratings yet
- 45 - Breast Developement and AnatomyDocument5 pages45 - Breast Developement and AnatomysasNo ratings yet
- What Is The Differential Diagnosis For The Breast Mass in An Adolescent?Document4 pagesWhat Is The Differential Diagnosis For The Breast Mass in An Adolescent?theodore_estradaNo ratings yet
- An Overview of Mammogram Analysis: Health and WellnessDocument8 pagesAn Overview of Mammogram Analysis: Health and WellnessAtakan GolNo ratings yet
- Breast AnatomyDocument3 pagesBreast AnatomyAshuNo ratings yet
- RAD334 - PPT.3 (1)Document70 pagesRAD334 - PPT.3 (1)fatymohammad1dNo ratings yet
- Penis Cancer, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPenis Cancer, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka, Annexure Ii Proforma For Registration of Subject For DissertationDocument13 pagesRajiv Gandhi University of Health Sciences, Bangalore, Karnataka, Annexure Ii Proforma For Registration of Subject For DissertationGirish SubashNo ratings yet
- Adult Primary Intraventricular HemorrhageDocument16 pagesAdult Primary Intraventricular Hemorrhageedi_ikhsan417No ratings yet
- Intervention MCQDocument2 pagesIntervention MCQmoath alseadyNo ratings yet
- Acute CholecystitisDocument25 pagesAcute Cholecystitissri wula moniNo ratings yet
- Flyer ORLIAC PITODocument2 pagesFlyer ORLIAC PITORatih GustifaNo ratings yet
- Herbst in Adults and TMDDocument12 pagesHerbst in Adults and TMDkhaled mohammadNo ratings yet
- Brochure NZOACON 2023Document4 pagesBrochure NZOACON 2023chaitanyaNo ratings yet
- Sr. No. Cghs Treatment Procedure/Investigation List (Delhi/Ncr) Non-Nabh/No Nabh/Nabl Rates Cghs Chennai Rate List 2014Document55 pagesSr. No. Cghs Treatment Procedure/Investigation List (Delhi/Ncr) Non-Nabh/No Nabh/Nabl Rates Cghs Chennai Rate List 2014Jaidilip JNo ratings yet
- Surgery Approved Dissertation Proposal and Dissertation Topics June 20 2019Document85 pagesSurgery Approved Dissertation Proposal and Dissertation Topics June 20 2019asi bassey50% (2)
- Clinical Science Session CT Scan Anatomi Kepala Normal: Preceptor: Dyana Eka Hadiati, DR., SP - RadDocument25 pagesClinical Science Session CT Scan Anatomi Kepala Normal: Preceptor: Dyana Eka Hadiati, DR., SP - Radfatimah putriNo ratings yet
- 2-9 Reda KamelDocument8 pages2-9 Reda KamelMoustafa Amin AlyNo ratings yet
- Microvascular and Laparoscopic InstrumentsDocument2 pagesMicrovascular and Laparoscopic InstrumentsJms RsNo ratings yet
- Portal VeinDocument7 pagesPortal VeinAsher Eby VargeeseNo ratings yet
- Pulmonary Artery Dissection in Eight DogsDocument13 pagesPulmonary Artery Dissection in Eight DogsYoga RivaldiNo ratings yet
- Fetal ContentDocument5 pagesFetal ContentPratima KushwahaNo ratings yet
- Conduct of Physical Examination RemindersDocument23 pagesConduct of Physical Examination RemindersJazer DairoNo ratings yet
- Anestesia EXIT 2021 Anae.15423Document6 pagesAnestesia EXIT 2021 Anae.15423joseNo ratings yet
- Acl Reconstruction Medial Portal With Toggleloc Fixation Device With Ziploop Technology and Compositcp Interference Screw Surgical TechniqueDocument20 pagesAcl Reconstruction Medial Portal With Toggleloc Fixation Device With Ziploop Technology and Compositcp Interference Screw Surgical TechniqueHArdz NavarroNo ratings yet
- Anae15291 Sup 0001 Appendixs1Document10 pagesAnae15291 Sup 0001 Appendixs1iamseraNo ratings yet
- Case Scenario Tia RevisedDocument1 pageCase Scenario Tia RevisedSherena NicolasNo ratings yet
- Arrangement of File For Medical PatientDocument3 pagesArrangement of File For Medical PatientIamnurse NylejNo ratings yet
- Introduction To Sectional AnatomyDocument56 pagesIntroduction To Sectional AnatomyMohd Izuan IbrahimNo ratings yet
- Acg 8 207Document5 pagesAcg 8 207Hung DoNo ratings yet
- Radial JawDocument32 pagesRadial Jawangelica giraldoNo ratings yet
- Carsh CartDocument35 pagesCarsh CartChinmayiNo ratings yet
- 4 Steps: Instrument PassingDocument3 pages4 Steps: Instrument PassingGwyn Leen CagasNo ratings yet
- Pages From FU784-293-The Only EKG Book You'Ll Ever N - Thaler, Malcolm SDocument3 pagesPages From FU784-293-The Only EKG Book You'Ll Ever N - Thaler, Malcolm Sindri lestari100% (1)
- Dhammi 2015Document3 pagesDhammi 2015Lisa AdeliaNo ratings yet
- Airway Management - CHFDocument2 pagesAirway Management - CHFRindang_Citraw_1819No ratings yet
- Cranial Nerve Examination OSCE GuideDocument34 pagesCranial Nerve Examination OSCE Guideluq9fifNo ratings yet