Download as pdf or txt
You might also like
- Baby Wise NotesDocument7 pagesBaby Wise Notesblashhill0% (1)
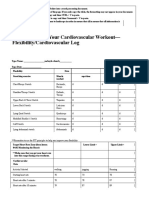
- 4.06 Recording Your Cardiovascular Workout - SchoologyDocument3 pages4.06 Recording Your Cardiovascular Workout - SchoologyMcKayla ChurchNo ratings yet
- Mikasa Ackerman Workout PDFDocument8 pagesMikasa Ackerman Workout PDFMaría100% (1)
- Pet CT and Pet Mri in Head and Neck MalignancyDocument10 pagesPet CT and Pet Mri in Head and Neck MalignancyAndrés Faúndez TeránNo ratings yet
- Second Primary OSCC 4Document8 pagesSecond Primary OSCC 4James BondNo ratings yet
- 1 s2.0 S0167814017326567 MainDocument23 pages1 s2.0 S0167814017326567 MainMadalina mNo ratings yet
- Imaging Characteristics of Nasopharyngeal Carcinoma For Predicting Distant MetastasisDocument7 pagesImaging Characteristics of Nasopharyngeal Carcinoma For Predicting Distant MetastasisJose JulianNo ratings yet
- One Stop Centre Staging by ContrastEnhanced FDG PETCT in Preoperative Assessment of Ovarian CancerDocument10 pagesOne Stop Centre Staging by ContrastEnhanced FDG PETCT in Preoperative Assessment of Ovarian CancerHana SalemNo ratings yet
- Cine MRI Based Analysis of Intrafractional Motion in Radiation Treatment PlanninDocument14 pagesCine MRI Based Analysis of Intrafractional Motion in Radiation Treatment Planninyuta titeNo ratings yet
- 10 1053@j Semnuclmed 2020 07 005Document10 pages10 1053@j Semnuclmed 2020 07 005anon_813722240No ratings yet
- Daisne 2004Document8 pagesDaisne 2004alinaNo ratings yet
- Surgical Management of Parapharyngeal Space Tumours in A Single Tertiary Care CenterDocument7 pagesSurgical Management of Parapharyngeal Space Tumours in A Single Tertiary Care CenterSilvia SoareNo ratings yet
- PETMRI and PETCT in Advanced Gynaecological TumoursDocument9 pagesPETMRI and PETCT in Advanced Gynaecological TumoursCsiszár MártonNo ratings yet
- Estro Acrop Prostate CancerDocument13 pagesEstro Acrop Prostate CancerStephanĭe Brĭto MartinezNo ratings yet
- 2019 Article 5894 PDFDocument8 pages2019 Article 5894 PDFGalgalo GarbichaNo ratings yet
- The Role of Imaging in Cervical Cancer Staging - ESGOESTROESP Guidelines (Update 2023)Document32 pagesThe Role of Imaging in Cervical Cancer Staging - ESGOESTROESP Guidelines (Update 2023)Limbert Rodríguez TiconaNo ratings yet
- Zumsteg Et Al 2015Document8 pagesZumsteg Et Al 2015Alyssa Anne GrandaNo ratings yet
- MainDocument8 pagesMainNurulrezki AtikaNo ratings yet
- 0040JKSMRM JKSMRM 17 8Document11 pages0040JKSMRM JKSMRM 17 8M P ChakravortyNo ratings yet
- Papaer Prueba 2Document9 pagesPapaer Prueba 2Joselyn CastroNo ratings yet
- JCB 12 42254Document7 pagesJCB 12 42254yohanasmjtNo ratings yet
- 1 s2.0 S036030160503097X MainDocument7 pages1 s2.0 S036030160503097X MainLuis Felipe Varela EspinozaNo ratings yet
- 10.1007@s00405 020 06019 2Document12 pages10.1007@s00405 020 06019 2luca totongNo ratings yet
- 1 s2.0 S1368837518304299 MainDocument8 pages1 s2.0 S1368837518304299 MainIgor VainerNo ratings yet
- Incidental Primary Breast Cancer Detected On PET-CTDocument8 pagesIncidental Primary Breast Cancer Detected On PET-CTMaxime PorcoNo ratings yet
- Theraphy RadDocument4 pagesTheraphy RadMega PuspitaNo ratings yet
- StudyDocument6 pagesStudyChandanaSanjeeNo ratings yet
- Promis TrialDocument8 pagesPromis TrialRubí BustamanteNo ratings yet
- Srep 30353Document7 pagesSrep 30353ErtyWitalayaL.ToruanNo ratings yet
- Mohamed 2020Document17 pagesMohamed 2020Alyssa Anne GrandaNo ratings yet
- Piis0167814019331123 230304 134522Document7 pagesPiis0167814019331123 230304 134522Samuel Kelvin RuslimNo ratings yet
- The Role of Diffusion-Weighted Magnetic Resonance Imaging in The Differentiation of Head and Neck MassesDocument10 pagesThe Role of Diffusion-Weighted Magnetic Resonance Imaging in The Differentiation of Head and Neck MassestaufikolingNo ratings yet
- Dziegielewski2017 Adressing The Contralateral TonsilDocument8 pagesDziegielewski2017 Adressing The Contralateral Tonsilnatalia.gallinoNo ratings yet
- Quantitative Ultrasound Characterization of Responses To Radiotherapy in Cancer Mouse ModelsDocument10 pagesQuantitative Ultrasound Characterization of Responses To Radiotherapy in Cancer Mouse Modelstaufiqur776No ratings yet
- Risk Factors For Brain Metastasis-Colocerctal CancerDocument8 pagesRisk Factors For Brain Metastasis-Colocerctal CancerIstianah SakdullahNo ratings yet
- ANZ Journal of Surgery - 2021 - Yang - Outcomes of Patients With Metastatic Cutaneous Squamous Cell Carcinoma To The Axilla PDFDocument8 pagesANZ Journal of Surgery - 2021 - Yang - Outcomes of Patients With Metastatic Cutaneous Squamous Cell Carcinoma To The Axilla PDFRong LiuNo ratings yet
- REQUITE A Prospective Multicentre Cohort Study ofDocument9 pagesREQUITE A Prospective Multicentre Cohort Study ofAhmad ShamyNo ratings yet
- PSS en SarcomatosisDocument6 pagesPSS en SarcomatosisJuan Torres MeleroNo ratings yet
- Highres Mri Surgery Early RectalccDocument10 pagesHighres Mri Surgery Early RectalccCsiszár MártonNo ratings yet
- 2011 - Kim, Kim, Beriwal - Contouring Inguinal and Femoral Nodes How Much Margin Is Needed Around The VesselsDocument1 page2011 - Kim, Kim, Beriwal - Contouring Inguinal and Femoral Nodes How Much Margin Is Needed Around The VesselsPoljarLijanNo ratings yet
- Lung Cancer Current Therapies and New Targeted TreatmentsDocument13 pagesLung Cancer Current Therapies and New Targeted TreatmentsWlad PaCaNo ratings yet
- Abordaje de Los Nodulos Pulmonares Indeterminados en El Tamizaje de Cancer de Pulmon Estudio Con PET CTDocument6 pagesAbordaje de Los Nodulos Pulmonares Indeterminados en El Tamizaje de Cancer de Pulmon Estudio Con PET CTAnaNo ratings yet
- P. Wang Et Al.2019Document6 pagesP. Wang Et Al.2019Mai M. AlshalNo ratings yet
- Radioterapia en CacUDocument6 pagesRadioterapia en CacUVicente RamosNo ratings yet
- Locally Recurrent Rectal Cancer: Toward A Second Chance at Cure? A Population-Based, Retrospective Cohort StudyDocument10 pagesLocally Recurrent Rectal Cancer: Toward A Second Chance at Cure? A Population-Based, Retrospective Cohort StudyYogeshBansodNo ratings yet
- A Domestic Porcine Model For Studying The Effects of Radiation On Head and Neck CancersDocument8 pagesA Domestic Porcine Model For Studying The Effects of Radiation On Head and Neck CancersdaruNo ratings yet
- Radiotherapy and OncologyDocument6 pagesRadiotherapy and OncologyIntan Kartika NursyahbaniNo ratings yet
- Fonc-09-00810 - Anisotropic CTV With DTIDocument8 pagesFonc-09-00810 - Anisotropic CTV With DTIgnunezNo ratings yet
- Radiomics Breakthrough Could Spark The Head and Neck Cancer Radiotherapy RevolutionDocument9 pagesRadiomics Breakthrough Could Spark The Head and Neck Cancer Radiotherapy Revolutionmazda626 retrocarsNo ratings yet
- 1530 Jul 27Document6 pages1530 Jul 27kelvin amahNo ratings yet
- Bacciu 2013Document10 pagesBacciu 2013AshokNo ratings yet
- Clinicopathological Predictors of Central Compartment Lymph Node Metastases in cN0 Papillary Thyroid CarcinomaDocument11 pagesClinicopathological Predictors of Central Compartment Lymph Node Metastases in cN0 Papillary Thyroid CarcinomaYacine Tarik AizelNo ratings yet
- Aaem 7 E8Document5 pagesAaem 7 E8hillarykNo ratings yet
- Radiomics Analysis For The Prediction of Locoregional Recurrence of Locally Advanced Oropharyngeal Cancer and Hypopharyngeal CancerDocument9 pagesRadiomics Analysis For The Prediction of Locoregional Recurrence of Locally Advanced Oropharyngeal Cancer and Hypopharyngeal CancermeghrajpurkayasthaNo ratings yet
- 22 Molecular Imaging and Biology Radiomics Cervical CancerDocument10 pages22 Molecular Imaging and Biology Radiomics Cervical CancerSara TovarNo ratings yet
- Extracranial ChondrosarcomaDocument8 pagesExtracranial ChondrosarcomaSyedNo ratings yet
- Piis0167814014005246 PDFDocument8 pagesPiis0167814014005246 PDFDiana MitreaNo ratings yet
- Radiotherapy and Oncology: ESTRO Consensus GuidelinesDocument8 pagesRadiotherapy and Oncology: ESTRO Consensus GuidelinesRaul Matute MartinNo ratings yet
- DX Evaluation Lung Cancer - UpToDateDocument2 pagesDX Evaluation Lung Cancer - UpToDateashlyanna3173No ratings yet
- Jurnal Ebm 2Document15 pagesJurnal Ebm 2Shadrina SafiraNo ratings yet
- Cancers-14-03105-With-CoverDocument16 pagesCancers-14-03105-With-CoverNovi OktaviantiNo ratings yet
- Imaging in Pediatric OncologyFrom EverandImaging in Pediatric OncologyStephan D. VossNo ratings yet
- Perbedaan Gambaran Radiologis Dari Avn, DDHDocument11 pagesPerbedaan Gambaran Radiologis Dari Avn, DDHEMIRZA NUR WICAKSONONo ratings yet
- PR LEviDocument14 pagesPR LEviEMIRZA NUR WICAKSONONo ratings yet
- EAP - Emirza Nur Wicaksono - Passive VoiceDocument1 pageEAP - Emirza Nur Wicaksono - Passive VoiceEMIRZA NUR WICAKSONONo ratings yet
- Vitri Widyaningsih, Khotijah, Balgis Faculty of Medicine, Sebelas Maret University, Surakarta, IndonesiaDocument1 pageVitri Widyaningsih, Khotijah, Balgis Faculty of Medicine, Sebelas Maret University, Surakarta, IndonesiaEMIRZA NUR WICAKSONONo ratings yet
- Limfoma Miokardial 2Document6 pagesLimfoma Miokardial 2EMIRZA NUR WICAKSONONo ratings yet
- Emirza Nur W - S022208020 - Bahasa InggrisDocument4 pagesEmirza Nur W - S022208020 - Bahasa InggrisEMIRZA NUR WICAKSONONo ratings yet
- Article Print 4609Document9 pagesArticle Print 4609EMIRZA NUR WICAKSONONo ratings yet
- Osteoporosis UASDocument200 pagesOsteoporosis UASEMIRZA NUR WICAKSONONo ratings yet
- GIT - Lec. 2 DR - BasimDocument28 pagesGIT - Lec. 2 DR - BasimEMIRZA NUR WICAKSONONo ratings yet
- Shahraiz Shah Rizvi, MBBS. Vidya Baleguli, MBBS. Merin Varghese, MD. Jawad Ahmed Ilyas, MD, MSDocument1 pageShahraiz Shah Rizvi, MBBS. Vidya Baleguli, MBBS. Merin Varghese, MD. Jawad Ahmed Ilyas, MD, MSEMIRZA NUR WICAKSONONo ratings yet
- Muhammad Rashid, Humaira Saleem, Saeed Bin Ayaz, Ijaz-Un-Nabi, Rashida Hussain, Faisal ManzoorDocument7 pagesMuhammad Rashid, Humaira Saleem, Saeed Bin Ayaz, Ijaz-Un-Nabi, Rashida Hussain, Faisal ManzoorEMIRZA NUR WICAKSONONo ratings yet
- Conventional Modalities and Novel, Emerging Imaging Techniques For Musculoskeletal TumorsDocument11 pagesConventional Modalities and Novel, Emerging Imaging Techniques For Musculoskeletal TumorsEMIRZA NUR WICAKSONONo ratings yet
- Diagnostic Imaging Modalities in Head and Neck Disease: Review ArticleDocument11 pagesDiagnostic Imaging Modalities in Head and Neck Disease: Review ArticleEMIRZA NUR WICAKSONONo ratings yet
- Content ServerDocument8 pagesContent ServerEMIRZA NUR WICAKSONONo ratings yet
- Tn. SaptoDocument17 pagesTn. SaptoEMIRZA NUR WICAKSONONo ratings yet
- Critical Changes in The Staging of Head and Neck Cancer: Christine M. Glastonbury, MBBSDocument8 pagesCritical Changes in The Staging of Head and Neck Cancer: Christine M. Glastonbury, MBBSEMIRZA NUR WICAKSONONo ratings yet
- Imaging Features and Differences Among The Three Primary Malignant Non-Wilms Tumors in ChildrenDocument9 pagesImaging Features and Differences Among The Three Primary Malignant Non-Wilms Tumors in ChildrenEMIRZA NUR WICAKSONONo ratings yet
- Heineken NV Annual Report 2020Document179 pagesHeineken NV Annual Report 2020Bich ThuyNo ratings yet
- Dental CariesDocument6 pagesDental CariesJerryboy69No ratings yet
- EQ FillableDocument3 pagesEQ FillableJenny Ruth TubanNo ratings yet
- LET Reviewer 2018Document55 pagesLET Reviewer 2018Jovy C. AndresNo ratings yet
- TH I Gian Làm Bài: 60 PhútDocument179 pagesTH I Gian Làm Bài: 60 PhútClone 3No ratings yet
- MODUL PRAKTEK Dental MaterialDocument11 pagesMODUL PRAKTEK Dental MaterialPutri Amalia MahsunNo ratings yet
- Euthanasia in CanadaDocument5 pagesEuthanasia in CanadaMariusz WesolowskiNo ratings yet
- Activity ProposalDocument3 pagesActivity ProposalMash JumahariNo ratings yet
- Forestry and Environmental Sciences: 1 AKLAN STATE UNIVERSITY - College of AgricultureDocument30 pagesForestry and Environmental Sciences: 1 AKLAN STATE UNIVERSITY - College of AgricultureAkeanon ReviewerNo ratings yet
- Appendix B Ecop-Eosh Tot - IntroDocument12 pagesAppendix B Ecop-Eosh Tot - IntroChristian MeanaNo ratings yet
- Caring Design. Insightful Technology.: GE HealthcareDocument20 pagesCaring Design. Insightful Technology.: GE HealthcareFunny Videos zNo ratings yet
- LH IflashDocument4 pagesLH IflashNIGHT tubeNo ratings yet
- HRM20016 Unit Outline - S12024 DR Vinesh-2Document12 pagesHRM20016 Unit Outline - S12024 DR Vinesh-2Roxy OngNo ratings yet
- 12 hk1 2Document4 pages12 hk1 2Na HyeNo ratings yet
- Functional MeatDocument54 pagesFunctional MeatnimraNo ratings yet
- Diet and Exercise EffectDocument5 pagesDiet and Exercise Effectsafar akramNo ratings yet
- Pitfalls Staging Oral Cavity Cancer 2013 AikenDocument19 pagesPitfalls Staging Oral Cavity Cancer 2013 AikenVilaseca224466No ratings yet
- Investigating The Preferences of Older People For Telehealth As A New Model of Health Care Service Delivery: A Discrete Choice ExperimentDocument13 pagesInvestigating The Preferences of Older People For Telehealth As A New Model of Health Care Service Delivery: A Discrete Choice Experimenttherese BNo ratings yet
- DLP in Grade 2 - HealthDocument8 pagesDLP in Grade 2 - HealthMariam KarisNo ratings yet
- EU Artificial Intelligence Act The European Approach To AIDocument11 pagesEU Artificial Intelligence Act The European Approach To AIIvana GreguricNo ratings yet
- Analysis of A Healthcare Risk Management PlanDocument6 pagesAnalysis of A Healthcare Risk Management PlanGeralds B GeraldNo ratings yet
- NCM 107 Transes Prelim 1Document7 pagesNCM 107 Transes Prelim 1Tatel JocelleNo ratings yet
- Marginal Costing in PepsicoDocument38 pagesMarginal Costing in Pepsicopallavi21_1992No ratings yet
- Textbook Narcissism and Its Discontents Diagnostic Dilemmas and Treatment Strategies With Narcissistic Patients Glen O Gabbard Ebook All Chapter PDFDocument54 pagesTextbook Narcissism and Its Discontents Diagnostic Dilemmas and Treatment Strategies With Narcissistic Patients Glen O Gabbard Ebook All Chapter PDFdarryl.potolsky581100% (9)
- PDF Doing Your Research Project A Guide For First Time Researchers 7Th Edition Stephen Waters Ebook Full ChapterDocument53 pagesPDF Doing Your Research Project A Guide For First Time Researchers 7Th Edition Stephen Waters Ebook Full Chapteredgar.addleman155100% (4)
- 4 Physical Fitness TestDocument7 pages4 Physical Fitness TestSergs Niño SamsonNo ratings yet