Professional Documents
Culture Documents
Schuetz EFFORT 2019 Lancet
Schuetz EFFORT 2019 Lancet
Uploaded by
Toño ZsucaritasCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Schuetz EFFORT 2019 Lancet
Schuetz EFFORT 2019 Lancet
Uploaded by
Toño ZsucaritasCopyright:
Available Formats
Articles
Individualised nutritional support in medical inpatients at
nutritional risk: a randomised clinical trial
Philipp Schuetz, Rebecca Fehr, Valerie Baechli, Martina Geiser, Manuela Deiss, Filomena Gomes, Alexander Kutz, Pascal Tribolet,
Thomas Bregenzer, Nina Braun, Claus Hoess, Vojtech Pavlicek, Sarah Schmid, Stefan Bilz, Sarah Sigrist, Michael Brändle, Carmen Benz,
Christoph Henzen, Silvia Mattmann, Robert Thomann, Claudia Brand, Jonas Rutishauser, Drahomir Aujesky, Nicolas Rodondi, Jacques Donzé,
Zeno Stanga*, Beat Mueller*
Summary
Lancet 2019; 393: 2312–21 Background Guidelines recommend the use of nutritional support during hospital stays for medical patients (patients
Published Online not critically ill and not undergoing surgical procedures) at risk of malnutrition. However, the supporting evidence
April 25, 2019 for this recommendation is insufficient, and there is growing concern about the possible negative effects of nutritional
http://dx.doi.org/10.1016/
therapy during acute illness on recovery and clinical outcomes. Our aim was thus to test the hypothesis that protocol-
S0140-6736(18)32776-4
guided individualised nutritional support to reach protein and caloric goals reduces the risk of adverse clinical
See Comment page 2278
outcomes in medical inpatients at nutritional risk.
*Equally contributing senior
authors
Methods The Effect of early nutritional support on Frailty, Functional Outcomes, and Recovery of malnourished
Medical University
Department, Division of medical inpatients Trial (EFFORT) is a pragmatic, investigator-initiated, open-label, multicentre study. We recruited
General Internal and medical patients at nutritional risk (nutritional risk screening 2002 [NRS 2002] score ≥3 points) and with an expected
Emergency Medicine, length of hospital stay of more than 4 days from eight Swiss hospitals. These participants were randomly assigned
Kantonsspital Aarau, Aarau,
Switzerland (Prof P Schuetz MD,
(1:1) to receive either protocol-guided individualised nutritional support to reach protein and caloric goals (intervention
R Fehr, V Baechli, M Geiser, group) or standard hospital food (control group). Randomisation was done with variable block sizes and stratification
M Deiss, F Gomes PhD, according to study site and severity of malnutrition using an interactive web-response system. In the intervention
A Kutz MD, Prof B Mueller MD); group, individualised nutritional support goals were defined by specialist dietitians and nutritional support was
Internal Medicine,
Spital Lachen, Lachen,
initiated no later than 48 h after admission. Patients in the control group received no dietary consultation. The
Switzerland (P Tribolet, composite primary endpoint was any adverse clinical outcome defined as all-cause mortality, admission to intensive
T Bregenzer MD); Internal care, non-elective hospital readmission, major complications, and decline in functional status at 30 days, and it was
Medicine, Kantonsspital measured in all randomised patients who completed the trial. This trial is registered with ClinicalTrials.gov, number
Münsterlingen, Münsterlingen,
Switzerland (N Braun MD,
NCT02517476.
C Hoess MD, V Pavlicek MD,
S Schmid); Internal Medicine Findings 5015 patients were screened, and 2088 were recruited and monitored between April 1, 2014, and Feb 28, 2018.
and Endocrinology, 1050 patients were assigned to the intervention group and 1038 to the control group. 60 patients withdrew consent
Kantonsspital St Gallen,
St Gallen, Switzerland
during the course of the trial (35 in the intervention group and 25 in the control group). During the hospital stay,
(S Bilz MD, S Sigrist MD, caloric goals were reached in 800 (79%) and protein goals in 770 (76%) of 1015 patients in the intervention group. By
Prof M Brändle MD, C Benz); 30 days, 232 (23%) patients in the intervention group experienced an adverse clinical outcome, compared with
Internal Medicine, 272 (27%) of 1013 patients in the control group (adjusted odds ratio [OR] 0·79 [95% CI 0·64–0·97], p=0·023). By
Kantonsspital Luzern, Luzern,
Switzerland (Prof C Henzen MD,
day 30, 73 [7%] patients had died in the intervention group compared with 100 [10%] patients in the control group
S Mattmann); Internal (adjusted OR 0·65 [0·47–0·91], p=0·011). There was no difference in the proportion of patients who experienced
Medicine, Bürgerspital side-effects from nutritional support between the intervention and the control group (162 [16%] vs 145 [14%], adjusted
Solothurn, Solothurn,
OR 1·16 [0·90–1·51], p=0·26).
Switzerland (R Thomann MD,
C Brand); Internal Medicine,
Kantonsspital Baselland, Interpretation In medical inpatients at nutritional risk, the use of individualised nutritional support during the
Standort Bruderholz hospital stay improved important clinical outcomes, including survival, compared with standard hospital food. These
Switzerland
findings strongly support the concept of systematically screening medical inpatients on hospital admission regarding
(Prof J Rutishauser PhD);
Department of General Internal nutritional risk, independent of their medical condition, followed by a nutritional assessment and introduction of
Medicine (Prof D Aujesky MD, individualised nutritional support in patients at risk.
Prof N Rodondi MD, J Donzé MD)
and Division of Diabetology,
Funding The Swiss National Science Foundation and the Research Council of the Kantonsspital Aarau, Switzerland.
Endocrinology, Nutritional
Medicine, and Metabolism
(Prof Z Stanga MD), Inselspital, Copyright © 2019 Elsevier Ltd. All rights reserved.
Bern University Hospital,
University of Bern, Bern,
Switzerland; Medical Faculty of
Introduction endocrine stress response, these nutritional deficits
the University of Basel, Basel, Anorexia arises as a physiological response to acute contribute to muscle wasting and progressive
Switzerland (Prof P Schuetz, illness and predisposes hospital inpatients to serious deterioration of metabolic and functional status, par
Prof B Mueller); Institute of caloric and protein deficits.1 In combination with ticularly in medical patients with multiple morbidities.2,3
Primary Health Care (BIHAM),
immobilisation and a pronounced inflammatory and More than 30% of medical inpatients are at increased
2312 www.thelancet.com Vol 393 June 8, 2019
Descargado para Anonymous User (n/a) en Universidad El Bosque de ClinicalKey.es por Elsevier en junio 30, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Articles
University of Bern, Bern,
Research in context Switzerland (Prof N Rodondi);
Division of General Internal
Evidence before this study caloric goals in medical inpatients at nutritional risk is effective Medicine, Brigham and
Current clinical practice guidelines recommend to consider in increasing caloric and protein intakes and in lowering the risk Women’s Hospital, Boston,
initiating nutritional support during the hospital stay of of adverse outcomes and mortality within 30 days. Patients MA, USA (J Donzé);
The New York Academy of
medical inpatients at risk of malnutrition. However, these receiving nutritional support also had improvements in Sciences, New York, NY, USA
recommendations are largely based on physiological rationales functional outcomes and quality of life. The beneficial effects of (F Gomes); and Department of
and observational studies, rather than interventional research. nutritional support were robust and comparable in subgroups Health Professions, Bern
A systematic review and meta-analysis published in 2016 that according to patient age, sex, severity of nutritional risk, and University of Applied Sciences,
Bern, Switzerland (P Tribolet)
focused on randomised trials investigating the effects of underlying disease.
Correspondence to:
nutritional interventions on clinical outcomes in medical
Implications of all the available evidence Prof Philipp Schuetz, University
inpatients, found only 22 trials with a total of 3736 participants. Department of Medicine,
Malnutrition is a highly prevalent condition in medical
Trials were mostly small and heterogeneous with overall low Kantonsspital Aarau, Tellstrasse,
inpatients that negatively impacts clinical outcomes. In CH-5001 Aarau, Switzerland
study quality. The pooled analysis showed that nutritional
conjunction with results of earlier smaller trials and philipp.schuetz@unibas.ch
interventions increased caloric and protein intake, as well as
observational research, findings of EFFORT strongly support
patient weight, but there was no effect on mortality, functional
the concept of systematically screening medical inpatients on
outcomes, or length of hospital stay. Thus, based on current
their admission to hospital regarding nutritional risk,
clinical trials, it is still unclear whether systematic screening for
independent of medical condition, followed by a nutritional
malnutrition in medical patients on their admission to hospital
assessment and introduction of individualised nutritional
and introduction of nutritional support in patients at risk has
support in patients at risk.
positive effects on clinical outcomes.
Added value of this study
This pragmatic, large-scale, multicentre trial showed that early
use of individualised nutritional support to reach protein and
risk of malnutrition, a condition that is strongly trials of critical care, we did the Effect of early nutritional
associated with increased mortality and morbidity, support on Frailty, Functional Outcomes, and Recovery
functional decline, prolonged hospital stays, and in of malnourished medical inpatients Trial (EFFORT). We
creased costs of health care.4–6 tested the hypothesis that protocol-guided individualised
Current clinical practice guidelines, including those by nutritional support to reach protein and caloric goals
the European Society for Clinical Nutrition and reduces the risk of adverse clinical outcomes in medical
Metabolism7 and the American Society for Parenteral and inpatients at nutritional risk.
Enteral Nutrition,8 recommend considering placing
medical inpatients identified by screening and assess Materials and methods
ment as being at risk of malnutrition on nutritional Study design and participants
support during their hospital stay. However, these EFFORT is a pragmatic, investigator-initiated, open-
recommendations are largely based on physiological label, non-blinded, non-commercial, multicentre, ran
rationales and observational studies. Some small trials domised, controlled trial, that was undertaken in
have found that nutritional support reduced the length eight Swiss hospitals. The rationale for the trial, design
of hospital stays and decreased mortality.9–12 Yet, details, and eligibility features have been published
two meta-analyses reported no significant improvements previously.16
in clinical outcomes associated with nutritional inter The eight participating sites were secondary and tertiary
ventions in medical inpatients receiving nutritional care hospitals and included the University Clinic in Aarau,
support, despite their increased caloric and protein the University Hospital in Bern, the Cantonal hospitals in
intake.13,14 Additionally, the introduction of nutritional Lucerne, Solothurn, St Gallen, Muensterlingen, and
support in medical inpatients with acute illnesses is Baselland, and the hospital in Lachen. All sites routinely
currently challenged by results of several high-quality used a validated screening tool for malnutrition based on
trials in critical care settings, which reported harmful the nutritional risk screening 2002 (NRS 2002) score.17,18
effects of full replacement nutrition strategies.1 These Nutritional risk screening includes assessment of the
negative effects might be explained by suppression of patient’s nutritional status (based on weight loss, body-
autophagy with inadequate clearance of acute cell mass index (BMI), and general condition or food intake)
damage associated with illness.15 and disease severity (stress metabolism) and is associated
In view of the scarcity of high-quality data from with increased risk of adverse outcomes. Each risk
medical inpatients and possible conflicts between predictor is scored from 0 to 3 points, and patients receive
current recom mendations for medical inpatients and an extra point if they are aged over 70 years.
www.thelancet.com Vol 393 June 8, 2019 2313
Descargado para Anonymous User (n/a) en Universidad El Bosque de ClinicalKey.es por Elsevier en junio 30, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Articles
Nutrition risk screening (NRS 2002) within 48 h of hospital admission in all patients
of anorexia nervosa, acute pancreatitis, acute liver
failure, cystic fibrosis, or stem-cell transplantation; after
If increased risk for malnutrition → individual assessment of the patient → if risk for malnutrition is present and gastric bypass surgery; with contraindications for
nutritional therapy is not contraindicated → establish a strategy to achieve individual nutritional targets
nutritional support; and previously included in the trial.
Individual nutrition targets All patients or their authorised representatives provided
Caloric requirements Protein requirements Micronutrient Specific targets
written informed consent.
Harris-Benedict equation 1·2–1·5 g/kg bodyweight requirements Disease-specific The Ethics Committee of Northwest and Central
with adjusted bodyweight per day (0·8 g/kg of Multivitamin use; other adaptations Switzerland (EKNZ) approved the study protocol in
or indirect calorimetry bodyweight per day in micronutrients (eg, medium-chain
patients with renal failure according to specific triglycerides, low January, 2014 (registration ID 2014_001). The trial was
with no dialysis) laboratory results potassium in patients started with a pilot study in Kantonsspital Aarau (Aarau,
with renal failure)
Switzerland) between April 1, 2014, and Aug 15, 2015,
during which time 175 participants were recruited.
Strategy to reach the nutrition targets After funding for the trial was secured and the pilot
showed high feasibility of nutritional intervention to
Level 1: oral nutrition (meals adapted to preferences, Multivitamins and multimineral supplements according
+ improve patient outcomes, the trial was registered at
food fortification or enrichment, and snacks between to 100% of recommended dietary allowance
meals and oral nutritional supplements) ClinicalTrials.gov (NCT02517476), in August, 2015 and
enrolment of patients was broadened to all participating
Yes
centres. There was no change in protocol regarding
Reassessment outcomes and interventional procedures between the
every 24–48 h: ≥75% of caloric initial institutional review board protocol and the final
and protein targets
trial protocol.
met?
No Randomisation
After 5 days escalate to level 2
Patients were randomly assigned (1:1) to receive either
individualised nutritional support (intervention group) or
standard hospital food (control group). Randomisation
Level 2: enteral nutrition Oral nutrition, no additional vitamins and mineral
was done with an interactive web-response system, with
+ variable block sizes, and patients were stratified according
supplements needed if enteral nutrition provides
≥1500 kcal per day to site and the severity of malnutrition. All participants
Yes and investigators were aware of group assignment but
outcome assessment was done by masked nurses.
Reassessment
every 24–48 h: ≥75% of caloric
and protein targets
Procedures
met? In the intervention group, nutritional support was
initiated as soon as possible after randomisation and
No
within 48 h after hospital admission. Patients received
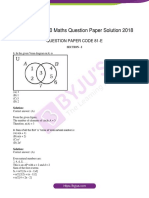
After 5 days escalate to level 3 individualised nutritional support (figure 1) to reach
protein and caloric goals, according to a previously
published consensus protocol19 that follows 2018 inter
Level 3: parenteral nutrition + Enteral and oral nutrition national guidelines.7 Briefly, individualised nutritional
goals were defined for each patient on hospital admission
Use concomitant minimal oral or enteral nutrition by a trained registered dietitian. Caloric requirements
(to avoid villous atrophy)
were predicted using the weight-adjusted Harris-Benedict
equation.20 Daily protein intake was set at 1·2–1·5 g/kg of
Figure 1: Nutritional algorithm used during the trial bodyweight to adjust for increased protein breakdown
Reproduced from Bounoure et al,19 by permission of Elsevier.
during acute disease,21 with lower targets for patients with
acute renal failure (0·8 g/kg of bodyweight). To reach
We enrolled patients aged at least 18 years at these goals, an individual nutritional plan was developed
nutritional risk of 3 or greater expected to stay in by a trained registered dietitian for each patient. This
hospital for more than 4 days if they were willing to plan was initially based on oral nutrition provided by the
provide informed consent within 48 h of hospital hospital kitchen (including food adjustment according to
admission for any reason. Patients were enrolled patient preferences, food fortification such as enrichment
between April 1, 2014, and Feb 28, 2018. We excluded of hospital food by adding protein powder, and snacks
patients who were initially admitted to intensive care between meals) and oral nutritional supplements.10,22 A
units or surgical units; unable to ingest oral nutrition; further increase in nutritional support to enteral tube
already receiving nutritional support on admission; feeding or parenteral feeding was recommended if at
with a terminal condition; admitted to hospital because least 75% of the daily caloric and protein targets could not
2314 www.thelancet.com Vol 393 June 8, 2019
Descargado para Anonymous User (n/a) en Universidad El Bosque de ClinicalKey.es por Elsevier en junio 30, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Articles
be reached through oral feeding within 5 days. Nutritional
intake was re-assessed every 24–48 h throughout the 5015 patients screened
hospital stay by a trained registered dietitian on the basis
of daily food records for each patient. On their discharge 1878 patients not included
from hospital, patients received dietary counselling 145 surgical patients
and, if indicated, a prescription for oral nutritional 268 unable to ingest oral nutrition
158 with a terminal condition
supplements in the outpatient setting. Patients did not 719 patients already receiving nutritional
receive dietary counselling in the outpatient setting after therapy on admission
31 hospitalised because of anorexia nervosa
discharge. 161 with acute pancreatitis
Patients in the control group received standard hospital 81 with acute liver failure
food according to their ability and desire to eat, with no 6 with cystic fibrosis
11 with stem cell transplantation
nutritional consultation and no recommendation for 27 with malnutrition after gastric bypass
additional nutritional support. On discharge, outcomes operations
43 with contraindication against nutritional
in these patients were followed up in the same way as therapy
patients in the intervention group but the decision to 228 previously included in the trial
prescribe nutritional support was at the discretion of the
nursing and physician team
3137 patients eligible for inclusion
Outcomes
The composite primary endpoint was defined as 1049 refused participation
adverse clinical outcome within 30 days, and it included:
all-cause mortality; admission to the intensive care
2088 patients randomly assigned
unit from the medical ward; non-elective hospital re-
admission after discharge; major complications as a
new occurrence including adjudicated nosocomial
infection, respiratory failure, a major cardiovascular 1050 assigned to intervention group 1038 assigned to control group
event (ie, stroke, intracranial bleeding, cardiac arrest,
myocardial infarction, or pulmonary embolism), acute
35 withdrew informed 25 withdrew informed
renal failure, gastro-intestinal failure (ie, haemorrhage, consent consent
intestinal perforation, acute pancreatitis); or a decline
in functional status of 10% or more from admission to
0 lost to follow-up 0 lost to follow-up
day 30 as measured by the Barthel’s index (scores range
from 0 to 100, with higher scores indicating better
functional status).23 Detailed definitions for each com 73 died 100 died
ponent of the primary endpoint are summarised in the
appendix.
942 completed interview at day 30 913 completed interview at day 30
The main secondary endpoints were each individual
component of the primary endpoint, daily protein and
caloric intake based on food records for each meal, and 1015 included in final analysis 1013 included in final analysis
total length of hospital stay, as well as short-term change
in bodyweight. Our protocol paper16 defined additional Figure 2: Trial profile
secondary outcomes, including other measurements at
day 7 and after 180 days of trial inclusion; however, we endpoints were side-effects from nutritional therapy, See Online for appendix
did not report all because of missing (ie, outcomes at defined as gastrointestinal side-effects, complications due
day 7) or incomplete information (long-term outcomes). to tube feeding or central venous catheter for parenteral
Additional assessment at day 30 was done through the nutrition, liver or gallbladder dysfunction, hyperglycaemia,
German version of the 5-level European Quality of Life 5 and refeeding syndrome.24 We obtained outcome data
Dimensions index (EQ-5D; index values range from 0 to 1, from charts reviewed by site research staff and trained
with higher scores indicating better quality of life), registered dietitians, and phone calls at day 30 with study
including the self-assessment visual analogue scale nurses masked to group assignment. Mortality during
(EQ-5D VAS; scores range from 0 to 100, with higher follow-up was verified by family members or the patient’s
scores indicating better health status). We did not refer to family physician.
the Functional Assessment Anorexia–Cancer Therapy
questionnaire, as denoted in the EFFORT protocol,16 Statistical analysis
because it is specifically aimed at patients with cancer and We tested the hypothesis that individualised nutritional
we did not investigate them separately from the overall support was superior to standard hospital food to avoid
population of medical patients in the analysis. Safety adverse clinical outcomes, which was our primary
www.thelancet.com Vol 393 June 8, 2019 2315
Descargado para Anonymous User (n/a) en Universidad El Bosque de ClinicalKey.es por Elsevier en junio 30, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Articles
data,25 we estimated that 40% of the target patient
Intervention Control group
group (n=1015) (n=1013) population would reach the primary endpoint within
30 days (10% mortality, 5% admission to an intensive
Sociodemographics
care unit from the hospital ward, 15% complications,
Mean age (years) 72·4 (14·1) 72·8 (14·1)
and 10% functional decline, with 10% of patients
Age group (years)
reaching more than one endpoint). We hypothesised
<65 177 (17%) 178 (18%)
that our nutritional intervention would decrease this risk
65–75 349 (34%) 322 (32%)
by an absolute number of 6% (relative decrease of 15%),
>75 489 (48%) 513 (51%)
from 40% to 34%. On the basis of these numbers,25 we
Male sex 525 (52%) 539 (53%)
estimated that a sample size of 1016 per group (total
Nutritional assessment number 2032) would have a power of at least 80% to find
Mean body-mass index (kg/m²)* 24·9 (5·4) 24·7 (5·3) a reduction in the probability of the primary composite
Mean bodyweight (kg) 70·9 (16·4) 70·9 (16·4) endpoint from 0·40 in the control group to 0·34 in
NRS 2002 score (%)† the intervention group, representing an absolute risk
3 points 310 (31%) 314 (31%) reduction of 6%.
4 points 391 (39%) 384 (38%) All analyses were done in the intention-to-treat
5 points 263 (26%) 261 (26%) population, which included all patients who had
>5 points 51 (5%) 54 (5%) undergone randomisation, unless they withdrew consent
Admission diagnosis or were lost to follow-up. For the primary outcome, we
Infection 298 (29%) 315 (31%) compared frequencies of adverse events using a χ² test.
Cancer 201 (20%) 173 (17%) The Kaplan-Meier method was used post hoc to visualise
Cardiovascular disease 92 (9%) 113 (11%) primary outcome data over time by calculating the
Failure to thrive 99 (10%) 95 (9%) probability of the primary outcome and of all-cause
Lung disease 50 (5%) 75 (7%) mortality within 30 days of randomisation. We also fitted
Gastrointestinal disease 96 (9%) 68 (7%) a logistic regression model predefined in the study
Neurological disease 42 (4%) 53 (5%) protocol and adjusted for main prognostic factors
Renal disease 34 (3%) 34 (3%) (Barthel’s index and NRS 2002 score at baseline) and
Metabolic disease‡ 30 (3%) 32 (3%) study centre. Results from the regression were reported
Other 30 (3%) 25 (2%) as adjusted odds ratios (OR) and corresponding 95% CIs.
Comorbidity We used a similar statistical approach for secondary
Hypertension 557 (55%) 552 (54%) endpoints, with Student’s t test and linear regression
Malignant disease 338 (33%) 329 (32%) models for continuous outcomes.
Chronic kidney disease 323 (32%) 318 (31%) We analysed predefined subgroups by including
Coronary heart disease 287 (28%) 279 (28%) interaction terms in the regression models to test for
Diabetes 215 (21%) 213 (21%) effect modification by important baseline factors.16
Congestive heart failure 174 (17%) 179 (18%)
Specifically, we tested for subgroups by patient age, sex,
Chronic obstructive pulmonary 147 (14%) 156 (15%)
NRS 2002 score, initial BMI, diagnosis at admission
disease (ie, infection, cardiovascular disease, renal failure,
Peripheral arterial disease 80 (8%) 106 (10%) gastrointestinal disease, cancer), and comorbidities
Cerebrovascular disease 75 (7%) 87 (9%) (diabetes, chronic kidney disease), as defined in the
Dementia 39 (4%) 36 (4%) protocol.
Data were analysed in STATA 15.1. There were no
Data are number of participants (%) or mean (SD). There were no significant interim analyses planned or made during the trial.
differences between the groups at baseline, except for admission diagnosis of
gastrointestinal disease and lung disease, and comorbidity of peripheral arterial
disease. NRS 2002=nutritional risk screening 2002. *The body-mass index is the Role of the funding source
weight in kilograms divided by the square of the height in metres. †Scores on The funders had no role in study design, data collection,
nutritional risk screening range from 0 to 7, with a score of 3 or more identifying
patients at nutritional risk and higher scores indicating increased risk. ‡Metabolic
data analysis, data interpretation, writing of the
disease included, but was not limited to, hypoglycaemia, hyperglycaemia, manuscript, and the decision to submit. The members
ketoacidosis, electrolyte disturbances including hyponatraemia and of the steering committee (appendix) designed the trial,
hypernatraemia, hypokalaemia, and hyperkalaemia.
collected and analysed the data, prepared the manu
Table 1: Characteristics of the patients at trial entry script, and decided to submit the manuscript for
publication.
composite endpoint. We postulated that early nutritional Results
therapy would reduce adverse clinical outcomes and From April 1, 2014, to Feb 28, 2018, we screened
mortality within a follow-up period of 30 days after the 5015 patients and enrolled 2088. Of these, 1050 were
index hospitalisation. From preliminary observational randomly assigned to the intervention group and 1038 to
2316 www.thelancet.com Vol 393 June 8, 2019
Descargado para Anonymous User (n/a) en Universidad El Bosque de ClinicalKey.es por Elsevier en junio 30, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Articles
the control group. With 60 patients withdrawing consent
A
and no other participants lost to follow-up, our final 100 Control
evaluable cohort consisted of 2028 patients (1015 patients Intervention
in the intervention group and 1013 patients in the control 90
group; figure 2). 80
Baseline characteristics were similar between groups
(table 1, appendix). Patients had a mean age of 72·6 years 70
Proportion of patients (%)
and a mean BMI of 24·8 kg/m². All patients were at 60
nutritional risk, with 31% of patients having a score of 3,
38% a score of 4, and 31% a score of 5 points or 50
more. The most frequent admission diagnoses were 40
infection, cancer, and cardiovascular disease. Patients
had a high burden of comorbidities, including malig 30
nant disease, chronic kidney disease, coronary artery
20
disease, diabetes, and congestive heart failure.
Protocol adherence during the hospital stay was high 10
and caloric goals were reached in 800 (79%) and protein
0
goals in 770 (76%) of 1015 patients in the intervention
group. 547 (54%) of 1013 patients in the control group B
reached their caloric goals and 557 (55%) reached their 100
protein goals. Compared with patients in the control
90
group, patients in the intervention group had significantly
higher mean daily caloric intake (1501 kcal per day 80
[SD 596] vs 1211 kcal per day [517], difference 290 kcal per
70
day [95% CI 240–340]), and protein intake (57 g per day
Proportion of patients (%)
[23] vs 47 g per day [21], difference 10 g per day [8–12]) 60
during their hospital stay (figure 3, appendix). These
50
numbers correspond to 22·2 kcal per kg bodyweight per
day (SD 9·6) versus 18·2 kcal per kg bodyweight per 40
day (8·8) in caloric intake, and 0·84 g protein per kg
30
bodyweight per day (0·35) versus 0·70 g protein per kg
bodyweight per day (0·34) versus in protein intake. In 20
the intervention group, 919 (91%) patients received oral
10
nutritional supplements in combination with enriched
hospital nutrition (appendix). Enteral nutrition was used 0
1 2 3 4 5 6 7 8 9 10
in eight patients and parenteral nutrition were used in
Days after random group assignment
12 in the intervention group. In the control group,
122 (12%) patients received some kind of nutritional Figure 3: Proportion of patients reaching caloric (A) and protein (B) requirements during the first 10 days
support during their hospital stay. On hospital discharge, after random group assignment
oral nutritional supplements were prescribed to
245 (24%) patients in the intervention group, compared non-elective hospital readmission, or major compli
with 21 (2%) patients in the control group (appendix). cations between groups.
We had complete information on the primary endpoint When compared with the control group, there was a
for all patients at day 30. An adverse clinical outcome significant improvement in the activities of daily living
(primary endpoint) occurred in 232 (23%) of 1015 patients score at 30 days in the intervention group, as measured
in the intervention group and in 272 (27%) of 1013 in the by the Barthel Index and higher quality of life measured
control group (adjusted OR 0·79 [95% CI 0·64–0·97]; by the EQ-5D index and the EQ-5D VAS (table 2). There
table 2). Kaplan-Meier estimates also showed a sig was no difference in the length of hospital stay between
nificantly shorter time to reach the primary endpoint in intervention and control group patients.
the control group (figure 4). We found no significant differences in potential side-
Regarding the different components of the composite effects from nutritional support including gastrointestinal
primary endpoint, patients in the intervention group had side-effects, complications due to enteral feeding, and
a lower risk of all-cause mortality within 30 days (table 2, hyperglycaemia (table 2).
appendix) and the survivors were at a lower risk of The effect of nutritional support on the risk for the
functional decline at day 30 of 10% or greater according primary endpoint was consistent across predefined sub
to the Barthel index, than control patients. There were no groups based on age, sex, baseline nutritional risk strati
differences in incidence of intensive care unit admission, fied for NRS 2002 score, initial BMI, diagnosis on
www.thelancet.com Vol 393 June 8, 2019 2317
Descargado para Anonymous User (n/a) en Universidad El Bosque de ClinicalKey.es por Elsevier en junio 30, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Articles
nutritional support increased daily energy and protein
Intervention Control group Odds ratio or p value
group (n=1015) (n=1013) coefficient (95% CI) intakes and lowered the risk of adverse clinical outcomes
at 30 days (primary outcome) and all-cause mortality
Outcomes
with improvements in functional status and quality of
Primary outcome
life without an apparent increase in adverse events from
Adverse outcome within 30 days 232 (23%) 272 (27%) 0·79 (0·64 to 0·97) 0·023
the intervention.
Single components of primary outcome
Several points of this trial are worth mentioning. First,
All-cause mortality 73 (7%) 100 (10%) 0·65 (0·47 to 0·91) 0·011
our findings validate some previous smaller trials9–12 but
Admission to the intensive care 23 (2%) 26 (3%) 0·85 (0·48 to 1·51) 0·58
contradict the findings of two meta-analyses, both of
unit
which reported no improvement in clinical outcomes.13,14
Non-elective hospital 89 (9%) 91 (9%) 0·99 (0·73 to 1·35) 0·96
readmission Set in a real-world context and without commercial
Major complications funding, our large-scale trial, which had high adherence
Any major complication 74 (7%) 76 (8%) 0·95 (0·68 to 1·34) 0·79 to the nutritional protocol and systematic assessment of
Nosocomial infection 40 (4%) 39 (4%) 1·01 (0·63 to 1·59) 0·98 outcomes, might resolve the current uncertainty about
Respiratory failure 14 (1%) 13 (1%) 1·06 (0·49 to 2·28) 0·89 the benefit of nutritional support in medical inpatients.
Major cardiovascular event 8 (1%) 7 (1%) 1·11 (0·40 to 3·11) 0·84
With a number needed to treat of 25 to prevent one
Acute kidney failure 32 (3%) 31 (3%) 1·01 (0·61 to 1·69) 0·96
adverse clinical outcome and 37 to prevent one death,
Gastrointestinal events 9 (1%) 15 (1%) 0·57 (0·25 to 1·31) 0·19
the nutritional intervention was effective at low
expenditure. The mortality benefit of nutritional support
Decline in functional status 35 (4%) of 942 55 (6%) of 913 0·62 (0·40 to 0·96) 0·034
of ≥10%* found in EFFORT was more pronounced, compared
Additional secondary outcomes with results of a pooled meta-analysis including
Mean length of stay (days) 9·5 (7·0) 9·6 (6·1) –0·21 (–0·76 to 0·35) 0·46 22 previous trials (9·8% vs 10·3% mortality, number
Mean Barthel score (points)* 88 (26) 85 (30) 3·26 (0·93 to 5·60) 0·006 needed to treat of 200),13 but was in the range of the
Mean EQ-5D VAS (points)† 59 (26) 56 (29) 3·06 (0·53 to 5·59) <0·0001 effect reported in the NOURISH trial (4·8% vs 9·7%
Mean EQ-5D index (points) 0·75 (0·32) 0·73 (0·34) 0·13 (0·09 to 0·17) 0·018
mortality, number needed to treat of 20).9 Second, to
Side-effects from nutritional support
increase external validity, EFFORT was pragmatic and
All side-effects 162 (16%) 145 (14%) 1·16 (0·90 to 1·51) 0·26
included a broad and heterogeneous population of
Gastrointestinal side-effects 43 (4%) 40 (4%) 1·12 (0·68 to 1·83) 0·66
medical inpatients with multiple morbidities, such as
different acute illnesses and chronic comorbidities.
Complications due to enteral 5 (<1%) 3 (<1%) 1·63 (0·38 to 6·95) 0·51
feeding or parenteral nutrition Several previous trials focused on specific patient
Liver or gall bladder dysfunction 4 (<1%) 7 (1%) 0·54 (0·15 to 1·91) 0·34 populations (eg, those with heart failure or cancer).9,13,26
Severe hyperglycaemia 48 (5%) 46 (5%) 1·06 (0·69 to 1·61) 0·80 However, we included patients with different internal
Refeeding syndrome 86 (8%) 73 (7%) 1·21 (0·86 to 1·70) 0·27 illnesses and our findings can thus be generalised to a
broader patient population (ie, patients with multiple
Data are number of events (%), unless otherwise stated. All odds ratios were calculated with a logistic regression for morbidities typically seen in internal medicine wards).
binary data and linear regression for continuous data. Models were adjusted for predefined prognostic factors (initial
nutritional risk screening score and baseline Barthel index) and study centre. *To estimate decline in functional status,
The beneficial effects of nutritional support were robust
we used the Barthel index (scores range from 0 to 100, with higher scores indicating better functional status) and and comparable in subgroups stratified according to
compared initial scores on admission with scores at day 30; only surviving patients were included in this analysis. patient age, sex, severity of nutritional risk, and
†To estimate quality of life we used the European Quality of Life 5 Dimensions index (EQ-5D; values range from
–0·205 to 1, with higher scores indicating better quality of life) including the visual-analogue scale (EQ-5D VAS;
underlying disease. The effects were even more
scores range from 0 to 100, with higher scores indicating better health status). pronounced in patients with chronic kidney disease, a
condition known to predispose patients to protein-
Table 2: Endpoints and adverse events
energy wasting.27 Third, no specific adverse side-effects
of the intervention were observed in our study. This was
hospital admission, or diabetes (p>0·05 for each sub also true for patients with diabetes, a population that
group analysis). However, we found a more pronounced was excluded in previous trials because of concerns of
beneficial effect of nutritional support in the population hyperglycaemia.9 Currently, there is a debate about the
of patients with chronic kidney disease, compared with benefits and optimal use of nutritional support in
patients in the control group (adjusted OR 0·61 [95% CI medical patients with acute and severe illness,28 with
0·44–0·86], p=0·045; figure 5). Findings regarding respect to the dose and quality of protein and overall
subgroup analysis for the outcome 30-day mortality were caloric intake, route of delivery, and if or how nutritional
similar, with a consistent effect across subgroups, except support needs to be adjusted for specific medical
for a more pronounced effect in patients with chronic conditions.28,29 Importantly, slower recovery and more
kidney disease (appendix). complications were reported in patients in critical care
receiving full replacement nutrition.1,30 There are
Discussion important differences between our study and other
In this multicentre trial, compared with a control critical care trials with regard to patient population,
group receiving standard hospital food, individualised severity of disease, and nutritional intervention. Because
2318 www.thelancet.com Vol 393 June 8, 2019
Descargado para Anonymous User (n/a) en Universidad El Bosque de ClinicalKey.es por Elsevier en junio 30, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Articles
patients in our population had milder disease severities
A
compared with patients in other trials in the critical care
1·00 Control group
setting, their cells might have been better at metabolising Intervention group
Proportion of patients with no adverse outcome
and using nutrients because of decreased insulin
resistance and decreased risk that nutrition would 0·90
interfere with autophagy.2,31
Our findings should not be used to support full 0·80
replacement nutrition in medical inpatients. Instead,
our concept of using individualised nutritional support
with the aim of reaching at least 75% of nutritional goals 0·70
has better clinical outcomes compared with not
providing nutritional support. Patients in our trial 0·60
received nutritional support according to a previously
published nutritional protocol with individualised HR 0·81 (95% CI 0·68–0·97), p=0·020
0·50
definition of each patient’s nutritional goals and the 0 10 20 30
required nutritional support.19 The nutritional protocol Number at risk
was based on a pathophysiological rationale and results Control group 1013 882 791 749
Intervention group 1015 895 825 786
of observational and smaller randomised trials. Unlike
other trials investigating the effect of specific nutritional B
formulas,9 we used a variety of nutritional support 1·00
strategies with the support of trained dietitians to reach
nutritional goals. Our trial does thus not provide
0·90
evidence on individual nutri tional components but
Proportion of surviving patients
supplies evidence that the overall strategy of providing
nutritional support to reach protein and caloric goals 0·80
during the acute phase of illness is beneficial for
patients. 0·70
EFFORT also has important ethical considerations.
Despite strong associations in observational research
between malnutrition and adverse clinical outcomes, it 0·60
has been unclear whether the provision of nutritional HR 0·65 (95% CI 0·48–0·88), p=0·0061
support has the potential to reduce the risks associated 0·50
with malnutrition, or whether it has deleterious effects 0 10 20 30
Analysis time (days)
on outcomes as demonstrated in critical care trials.30 Number at risk
After discussions with national experts in the field Control group 1013 967 922 913
Intervention group 1015 975 949 943
(ie, trial collaborators) and our ethical review board, we
were of the opinion that it was ethically acceptable that Figure 4: Kaplan-Meier estimates of the cumulative incidence of the primary endpoint and all-cause mortality
patients in the control group received no additional (A) Time to the first event of the composite primary endpoint (log-rank p value=0·035). (B) Time to death
(log-rank p value=0·031).
nutritional treatment. This is also in accordance with
a previous Swiss consensus ethics statement32 that
pointed out that “intake of standard food and fluids is a dietitians. Similar to real-life experience, several patient,
basic right of any patients”, yet any sort of nutritional treatment, and hospital factors (eg, delay or refusal to
therapy must be viewed as a therapeutic measure and start enteral or parenteral nutrition by the patient, early
must therefore fulfil all criteria for this, including proof discharge of patients, diagnostic exams interfering
of clinical effectiveness, safety, and cost-effectiveness.32 with nutritional support) might have prevented full
For our population of patients, such proof was still adherence to the protocol. Still, we expect this bias to
missing and was thus the main aim of this trial. be conservative with regard to the relevant endpoints,
We are aware of limitations in our study. First, our and protocol adherence was higher than in previous
trial was pragmatic, and masking of participants and nutritional trials in medical inpatients.13 Third, nutrition
personnel was deemed to be impractical. Although the in the control group represented the reality of standard
primary outcome at 30 days was objective and its Swiss hospital food, which might not be unconditionally
assessment was masked, some of the outcomes assessed generalisable to other health-care systems. Fourth, we
during the hospital stay might have been vulnerable to did not yet investigate the costs of the intervention but
observer bias. Second, 215 (21%) of patients in the we have planned to do a future cost-effectiveness
intervention group did not fully reach their caloric goals analysis on the basis of the trial data. Finally, the
and 243 (24%) their protein goals, despite imple registration of the trial was delayed, as we started with
mentation of the nutritional protocol by trained a pilot study to ensure feasibility of the complex
www.thelancet.com Vol 393 June 8, 2019 2319
Descargado para Anonymous User (n/a) en Universidad El Bosque de ClinicalKey.es por Elsevier en junio 30, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Articles
Control group Intervention group Adjusted odds ratio pinteraction
(n/N [%]) (n/N [%]) (95% CI)
All patients 272/1013 (27%) 232/1015 (23%) 0·79 (0·64–0·97)
Age (years)
<65 30/178 (17%) 34/177 (19%) 1·17 (0·68–2·02) 0·27
65–75 93/322 (29%) 82/349 (23%) 0·76 (0·54–1·07)
>75 149/513 (29%) 116/489 (24%) 0·76 (0·57–1·01)
Sex
Male 157/539 (29%) 104/490 (21%) 0·78 (0·60–1·03) 0·74
Female 115/474 (24%) 128/525 (24%) 0·84 (0·62–1·14)
Risk for malnutrition
NRS 3 points 72/314 (23%) 69/310 (22%) 0·96 (0·66–1·40) 0·31
NRS 4 points 103/384 (27%) 83/391 (21%) 0·74 (0·53–1·02)
NRS >4 points 97/315 (31%) 80/314 (25%) 0·77 (0·54–1·09)
Body-mass index
<20 48/198 (24%) 43/176 (24%) 1·01 (0·63–1·62) 0·28
20–25 107/372 (29%) 100/421 (24%) 0·77 (0·56–1·06)
25–30 75/283 (27%) 61/254 (24%) 0·88 (0·59–1·30)
>30 40/156 (26%) 27/157 (17%) 0·60 (0·35–1·04)
Admission diagnosis
Infection 70/315 (22%) 57/298 (19%) 0·83 (0·56–1·23) 0·85
Cardiovascular disease 36/113 (32%) 26/92 (28%) 0·84 (0·46–1·54) 0·90
Renal failure 9/34 (26%) 10/34 (29%) 1·16 (0·40–3·34) 0·50
Gastrointestinal disease 19/68 (28%) 23/96 (24%) 0·81 (0·40–1·65) 0·98
Cancer 62/173 (36%) 71/201 (35%) 0·98 (0·64–1·49) 0·26
Comorbidities
Diabetes 54/213 (25%) 44/215 (20%) 0·76 (0·48–1·19) 0·76
Chronic kidney disease 115/318 (36%) 83/323 (26%) 0·61 (0·44–0·86) 0·045
0·1 1 2 3
Nutritional support Nutritional support
reduces adverse increases adverse
outcome outcome
Figure 5: Odds ratios for adverse outcome in prespecified subgroups
The only significant interactions between group assignment and subgroup were for chronic kidney disease. The body-mass index is the weight (in kg) divided by the
square of the height (in m). NRS=nutritional risk screening.
nutritional intervention and to secure funding for the Contributors
multicentre rollout. However, there was no change in PS was the principal investigator of this trial and was responsible for
obtaining funding, drafting the trial protocol, analysing and interpreting
trial protocol and we thus included all patients in the the data, and writing the final report. RF, VB, MG, MD, PT, NB, SSc,
final analysis. CBe, SM, and CBr were involved in drafting the trial protocol, data
Understanding the optimal use of nutritional support collection, and approval of the final version of the manuscript. FG, AK,
is complex because timing, route of delivery, and the TB, CH, VP, SB, SSi, MB, CH, RT, JR, DA, NR, and JD were involved in
drafting the trial protocol, supervising the study sites, drafting the final
amount and type of nutrients might all affect clinical manuscript, and approval of the final version of the manuscript. ZS and
outcomes. In our trial, we asked the basic question of BM were involved in obtaining funding, drafting the trial protocol,
whether nutritional support during the hospital stay supervising study sites, drafting the final manuscript, and approving the
improves outcomes in medical patients at nutritional final version of the manuscript.
risk, compared with standard hospital food. This trial Declaration of interests
showed that early use of individualised nutritional The study was initiated by the investigator and supported by grants from
the Swiss National Science Foundation to PS and the Research Council
support to reach protein and caloric goals in medical of Kantonsspital Aarau, Switzerland. The Institution of PS has
inpatients at nutritional risk is effective in increasing previously received unrestricted grant money unrelated to this project
energy and protein intakes, and in lowering the risk of from Nesté Health Science and Abbott Nutrition. The institution of ZS
adverse outcomes and mortality within 30 days. Our received speaking honorariums and research support from Nesté Health
Science, Abbott Nutrition, and Fresenius Kabi. All other authors report
findings strongly support the concept of systematically no conflicts of interest.
screening medical inpatients on admission to hospital
Data sharing
for nutritional risk, irrespective of any underlying We intend to make data collected for the study, including anonymised
conditions, followed by a nutritional assessment and individual participant data and a data dictionary defining each field in the
introduction of individualised nutritional support in set, available to others. Related documents will be available, including the
trial protocol and the statistical analysis plan. These data will be available
at-risk patients.
2320 www.thelancet.com Vol 393 June 8, 2019
Descargado para Anonymous User (n/a) en Universidad El Bosque de ClinicalKey.es por Elsevier en junio 30, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Articles
with the publication of our main manuscript and all secondary projects 13 Bally MR, Blaser Yildirim PZ, Bounoure L, et al. Nutritional support
as outlined in our trial protocol on receipt of a letter of intention detailing and outcomes in malnourished medical inpatients: a systematic
the study hypothesis and statistical analysis plan. The steering committee review and meta-analysis. JAMA Intern Med 2016; 176: 43–53.
of this trial will discuss all requests and decide on the basis of the 14 Feinberg J, Nielsen EE, Korang SK, et al. Nutrition support in
scientific rigor of the proposal whether data sharing is appropriate. hospitalised adults at nutritional risk. Cochrane Database Syst Rev
All applicants are asked to sign a data access agreement. Please send any 2017; 5: CD011598.
request to the principal investigator of this trial. 15 Schetz M, Casaer MP, Van den Berghe G. Does artificial nutrition
improve outcome of critical illness? Crit Care 2013; 17: 302.
Acknowledgments 16 Schuetz P, Fehr R, Baechli V, et al. Design and rationale of the effect
We thank all patients and hospital staff for support of our trial. of early nutritional therapy on frailty, functional outcomes and
The Swiss National Science Foundation (SNSF professorship, recovery of malnourished medical inpatients trial (EFFORT):
PP00P3_150531 and and PP00P3_176972) and the Research Council of a pragmatic, multicenter, randomized-controlled trial.
the Kantonsspital Aarau, Switzerland (1410.000.058 and 1410.000.044) Int J Clin Trials 2018; 5: 77.
provided funding for the trial. We are grateful to Jeffrey Greenwald 17 Kondrup J, Johansen N, Plum LM, et al. Incidence of nutritional
(Massachusetts General Hospital, Boston, MA, USA), Ulrich Keller risk and causes of inadequate nutritional care in hospitals.
(EndoNet Praxis, Basel, Switzerland), Peter E Ballmer (Kantonsspital Clin Nutr 2002; 21: 461–68.
Winterthur, Winterthur, Switzerland), Jeannie Wurz (Inselspital, Bern, 18 Kondrup J, Allison SP, Elia M, et al. ESPEN guidelines for nutrition
Switzerland), and C Elizabeth Weekes (Guy’s and St Thomas’ National screening 2002. Clin Nutr 2003; 22: 415–21.
Health Service Foundation Trust, London, UK) for helpful scientific 19 Bounoure L, Gomes F, Stanga Z, et al. Detection and treatment of
discussions. medical inpatients with or at-risk of malnutrition: suggested
procedures based on validated guidelines. Nutrition 2016; 32: 790–98.
References
20 MacDonald A, Hildebrandt L. Comparison of formulaic equations to
1 Casaer MP, Van den Berghe G. Nutrition in the acute phase of
determine energy expenditure in the critically ill patient. Nutrition
critical illness. N Engl J Med 2014; 370: 1227–36.
2003; 19: 233–39.
2 Schutz P, Bally M, Stanga Z, Keller U. Loss of appetite in acutely ill
21 Genton L, Pichard C. Protein catabolism and requirements in
medical inpatients: physiological response or therapeutic target?
severe illness. Int J Vitam Nutr Res 2011; 81: 143–52.
Swiss Med Wkly 2014; 144: w13957.
22 Milne AC, Potter J, Vivanti A, Avenell A. Protein and energy
3 Felder S, Braun N, Stanga Z, et al. Unraveling the link between
supplementation in elderly people at risk from malnutrition.
malnutrition and adverse clinical outcomes: association of acute and
Cochrane Database Syst Rev 2009; 2: CD003288.
chronic malnutrition measures with blood biomarkers from
different pathophysiological states. Ann Nutr Metab 2016; 68: 164–72. 23 Mahoney FI, Barthel DW. Functional evaluation: the Barthel index.
Md State Med J 1965; 14: 61–65.
4 Felder S, Lechtenboehmer C, Bally M, et al. Association of
nutritional risk and adverse medical outcomes across different 24 Friedli N, Stanga Z, Culkin A, et al. Management and prevention of
medical inpatient populations. Nutrition 2015; 31: 1385–93. refeeding syndrome in medical inpatients: an evidence-based and
consensus-supported algorithm. Nutrition 2018; 47: 13–20.
5 Khalatbari-Soltani S, Marques-Vidal P. The economic cost of
hospital malnutrition in Europe; a narrative review. 25 Schuetz P, Hausfater P, Amin D, et al. Optimizing triage and
Clin Nutr ESPEN 2015; 10: e89–94. hospitalization in adult general medical emergency patients:
the triage project. BMC Emerg Med 2013; 13: 12.
6 Imoberdorf R, Meier R, Krebs P, et al. Prevalence of undernutrition
on admission to Swiss hospitals. Clin Nutr 2010; 29: 38–41. 26 Broqvis M, Arnqvist H, Dahlström U, Larsson J, Nylander E,
Permert J. Nutritional assessment and muscle energy metabolism
7 Gomes F, Schuetz P, Bounoure L, et al. ESPEN guidelines on
in severe chronic congestive heart failure—effects of long-term
nutritional support for polymorbid internal medicine patients.
dietary supplementation. Eur Heart J 1994; 15: 1641–50.
Clin Nutr 2018; 37: 336–53.
27 Kalantar-Zadeh K, Fouque D. Nutritional management of chronic
8 Mueller C, Compher C, Ellen DM. ASPEN clinical guidelines:
kidney disease. N Engl J Med 2017; 377: 1765–76.
nutrition screening, assessment, and intervention in adults.
JPEN J Parenter Enteral Nutr 2011; 35: 16–24. 28 Schuetz P. Food for thought: why does the medical community
struggle with research about nutritional therapy in the acute care
9 Deutz NE, Matheson EM, Matarese LE, et al. Readmission and
setting? BMC Med 2017; 15: 38.
mortality in malnourished, older, hospitalized adults treated with a
specialized oral nutritional supplement: a randomized clinical trial. 29 Schuetz P. “Eat your lunch!”—controversies in the nutrition of the
Clin Nutr 2016; 35: 18–26. acutely, non-critically ill medical inpatient. Swiss Med Wkly 2015;
145: w14132.
10 Potter JM, Roberts MA, McColl JH, Reilly JJ. Protein energy
supplements in unwell elderly patients—a randomized controlled 30 Casaer MP, Mesotten D, Hermans G, et al. Early versus late
trial. JPEN J Parenter Enteral Nutr 2001; 25: 323–29. parenteral nutrition in critically ill adults. N Engl J Med 2011;
365: 506–17.
11 Starke J, Schneider H, Alteheld B, Stehle P, Meier R. Short-term
individual nutritional care as part of routine clinical setting 31 Russell RC, Yuan HX, Guan KL. Autophagy regulation by nutrient
improves outcome and quality of life in malnourished medical signaling. Cell Res 2014; 24: 42–57.
patients. Clin Nutr 2011; 30: 194–201. 32 Baumann-Hölzle R, Imoberdorf R, Koblet K, et al.
12 Somanchi M, Tao X, Mullin GE. The facilitated early enteral and Ernährungsautonomie—ethisches Grundsatzpapier zur Ernährung
dietary management effectiveness trial in hospitalized patients with der Patientinnen und Patienten im Akutspital.
malnutrition. JPEN J Parenter Enteral Nutr 2011; 35: 209–16. Schweizerische Ärztezeitung 2006; 87: 33.
www.thelancet.com Vol 393 June 8, 2019 2321
Descargado para Anonymous User (n/a) en Universidad El Bosque de ClinicalKey.es por Elsevier en junio 30, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Special Quadrilaterals: Honors GeometryDocument38 pagesSpecial Quadrilaterals: Honors GeometryMuhammad MirzaNo ratings yet
- Od 1Document2 pagesOd 1Toño ZsucaritasNo ratings yet
- Gutjnl 2020 323371Document14 pagesGutjnl 2020 323371Toño ZsucaritasNo ratings yet
- Cureus 0015 00000035013Document7 pagesCureus 0015 00000035013Toño ZsucaritasNo ratings yet
- Dino World Water RulesDocument2 pagesDino World Water RulesToño ZsucaritasNo ratings yet
- Problems With Adjectives and AdverbsDocument9 pagesProblems With Adjectives and AdverbsSonseungwanNo ratings yet
- The Process of Expository Preaching Sermon Study and Development 1 PDFDocument19 pagesThe Process of Expository Preaching Sermon Study and Development 1 PDFjNo ratings yet
- Gardenia PlantsDocument6 pagesGardenia PlantsyayayayasNo ratings yet
- ERT 426 Food Engineering Semester 1 Academic Session 2017/18Document32 pagesERT 426 Food Engineering Semester 1 Academic Session 2017/18nas radziNo ratings yet
- Inorganic Chemistry 1 - Alkali Metals RevisioDocument7 pagesInorganic Chemistry 1 - Alkali Metals RevisioAshleyn Mary SandersNo ratings yet
- Group Hot TopicDocument40 pagesGroup Hot Topicapi-425561076No ratings yet
- Internal Motivation Infographics by SlidesgoDocument34 pagesInternal Motivation Infographics by Slidesgoyosua tafulyNo ratings yet
- Ch-8 Challeges To DemocracyDocument2 pagesCh-8 Challeges To DemocracySujitnkbpsNo ratings yet
- Cartoon AbetmentDocument12 pagesCartoon AbetmentRabihaNo ratings yet
- Kseeb Class 10 Maths Question Paper Solution 2018Document23 pagesKseeb Class 10 Maths Question Paper Solution 2018Raghav L NaikNo ratings yet
- Ambiguous Character GertrudeDocument3 pagesAmbiguous Character GertrudeAshton MartinNo ratings yet
- Sixth Meeting MinutesDocument4 pagesSixth Meeting MinutesTanvi BakshiNo ratings yet
- HYPACK ECHO Brochure 2022 Nautilus OceanicaDocument2 pagesHYPACK ECHO Brochure 2022 Nautilus OceanicaADOUKONo ratings yet
- Letter To Trainee For Visa Tp-6. Aiesec in ColombiaDocument7 pagesLetter To Trainee For Visa Tp-6. Aiesec in ColombiaLucho MedinaNo ratings yet
- Operazione DoMS IITR IntroDocument1 pageOperazione DoMS IITR IntroSaransh MaheshwariNo ratings yet
- 04 What Is Easement Distinguish Easement From Usufruct 2 Can There Be A An - Course HeroDocument9 pages04 What Is Easement Distinguish Easement From Usufruct 2 Can There Be A An - Course HerojrstockholmNo ratings yet
- Corrosion Prevention and ControlDocument19 pagesCorrosion Prevention and ControlJosa FatyNo ratings yet
- Verge PH Swot AnalysisDocument3 pagesVerge PH Swot AnalysisPamela ApacibleNo ratings yet
- November 2019 (v3) QP - Paper 4 CIE Chemistry IGCSEDocument16 pagesNovember 2019 (v3) QP - Paper 4 CIE Chemistry IGCSEJeevith Soumya SuhasNo ratings yet
- Bungcaras Vs Bravo (Notice of Appeal)Document2 pagesBungcaras Vs Bravo (Notice of Appeal)Ramonbeulaneo RancesNo ratings yet
- Physics Investigatory ProjectDocument18 pagesPhysics Investigatory ProjectMoghanNo ratings yet
- 友谊论文的论点Document6 pages友谊论文的论点gwhjcowlfNo ratings yet
- Haytham Abd Allah Ezbawy ResumeDocument3 pagesHaytham Abd Allah Ezbawy Resumehayssam ezbawyNo ratings yet
- Anth 133 - HUNTERS AND GATHERERS PDFDocument15 pagesAnth 133 - HUNTERS AND GATHERERS PDFAnjelica Pearl NazarenoNo ratings yet
- Eat Lots of Chocolates When Time Gets Tough, and Eat Even More When Times Are Great.Document2 pagesEat Lots of Chocolates When Time Gets Tough, and Eat Even More When Times Are Great.Miruna MocleașăNo ratings yet
- Lectures On The Mechanical Foundations of ThermodynamicsDocument99 pagesLectures On The Mechanical Foundations of ThermodynamicsMarta HerranzNo ratings yet
- Example of A Business Model Canvas Coconut Treat StandDocument2 pagesExample of A Business Model Canvas Coconut Treat StandSabrena FennaNo ratings yet
- Water and Its Forms: Name: - DateDocument2 pagesWater and Its Forms: Name: - DateNutrionist Preet PatelNo ratings yet
- Maerskgroup Evaluatingstrategic TalentmanagementinitiativesDocument22 pagesMaerskgroup Evaluatingstrategic TalentmanagementinitiativesSameer FaisalNo ratings yet