Download as pdf or txt
You might also like
- Ebook PDF Child Development An Active Learning Approach 3rd Edition PDFDocument41 pagesEbook PDF Child Development An Active Learning Approach 3rd Edition PDFmike.casteel80798% (45)
- Physiotherapy Assessment For Orthopedic ConditionsDocument6 pagesPhysiotherapy Assessment For Orthopedic ConditionsSHAIK SHABEENA100% (3)
- Cardio-Respiratory Assessment ChartDocument3 pagesCardio-Respiratory Assessment ChartVishal Patle100% (3)
- Case Taking ProformaDocument7 pagesCase Taking ProformaDr Dushyant Kamal Dhari50% (2)
- ROS ChecklistDocument3 pagesROS ChecklistPAschoolstuff100% (4)
- Postnatal Assessment FormatDocument16 pagesPostnatal Assessment FormatValarmathi92% (13)
- Musculoskeletal Physical Therapy AssessmentDocument6 pagesMusculoskeletal Physical Therapy Assessmentlecturio100% (1)
- Pharyngitis. NCPDocument2 pagesPharyngitis. NCPbiancaNo ratings yet
- Answers To Workbook Exercises: Unit 4 Variation and Classification Exercise 4.1 Horses, Donkeys and MulesDocument2 pagesAnswers To Workbook Exercises: Unit 4 Variation and Classification Exercise 4.1 Horses, Donkeys and MulesZied EzzaouiaNo ratings yet
- Full Assessment ToolDocument13 pagesFull Assessment ToolBrandy JaffarNo ratings yet
- General Assessment Surgical WardDocument10 pagesGeneral Assessment Surgical Wardwisdumb rantsNo ratings yet
- FCA QuestionnaireDocument8 pagesFCA QuestionnaireAevah QuinnNo ratings yet
- Case Study FormatDocument15 pagesCase Study FormatLavie GangwarNo ratings yet
- Bedside Med HX Maker PDFDocument2 pagesBedside Med HX Maker PDFjustinryanNo ratings yet
- TIPPS Psychiatric Evaluation ProformaDocument7 pagesTIPPS Psychiatric Evaluation Proformaknvr2001100% (1)
- FormatDocument3 pagesFormatwarnerNo ratings yet
- History Taking ChecklistDocument4 pagesHistory Taking Checklistalnoooor38100% (1)
- Standard Is Ed Case FormatDocument2 pagesStandard Is Ed Case FormatDipti RamiNo ratings yet
- Fulton-Montgomery Community College Nursing ProgramDocument13 pagesFulton-Montgomery Community College Nursing ProgramNate StevesNo ratings yet
- Patient HistoryDocument7 pagesPatient HistoryFrance PalNo ratings yet
- Cardiorespiratory Assessment ChartDocument3 pagesCardiorespiratory Assessment Chartphysiovipin100% (3)
- Orthopedic Physiotherapy AssessmentDocument2 pagesOrthopedic Physiotherapy AssessmentVijaya KrishnaNo ratings yet
- Cardiac System AssessmentDocument14 pagesCardiac System AssessmentValarmathi100% (1)
- Antenatal Assessment FormatDocument9 pagesAntenatal Assessment FormatPalaniswami Palaniswami67% (3)
- Electronic Health Record (EHR) of Click Health Services Care Receiver (CR)Document10 pagesElectronic Health Record (EHR) of Click Health Services Care Receiver (CR)Himel Baidya HimuNo ratings yet
- Electronic Health Record (EHR) of Click Health Services Care Receiver (CR)Document10 pagesElectronic Health Record (EHR) of Click Health Services Care Receiver (CR)Himel Baidya HimuNo ratings yet
- History and Physical Exam TemplateDocument7 pagesHistory and Physical Exam TemplateJonathan A SalamatNo ratings yet
- Leprosy Case ProformaDocument4 pagesLeprosy Case Proforma127 Shruthik Patel Thota100% (1)
- GITDocument4 pagesGITDarawan MirzaNo ratings yet
- CSC Proforma - FeverDocument6 pagesCSC Proforma - Fever127 Shruthik Patel ThotaNo ratings yet
- Adult and Elder I. Nursing Care PlanDocument6 pagesAdult and Elder I. Nursing Care PlanteresapazNo ratings yet
- History Taking List Origin Copy 2Document7 pagesHistory Taking List Origin Copy 2Sudhakaŕ KolluNo ratings yet
- History Taking in SurgeryDocument40 pagesHistory Taking in Surgeryasher masoodNo ratings yet
- Antenatal AssessmentDocument7 pagesAntenatal Assessmentmohapatra devNo ratings yet
- Antenatal History FormatDocument9 pagesAntenatal History FormatBincy Jilo90% (21)
- Unit 829 Level 3 Provide Spa Treatments Treatment Evidence FormDocument4 pagesUnit 829 Level 3 Provide Spa Treatments Treatment Evidence FormJowie SooNo ratings yet
- Full OSCE (Medicine) - 1Document85 pagesFull OSCE (Medicine) - 1Mimo HemadNo ratings yet
- History and Examinatoin of The Resp. SystemDocument37 pagesHistory and Examinatoin of The Resp. Systemmawada abdallaNo ratings yet
- History Taking in SurgeryDocument40 pagesHistory Taking in SurgerymiftahulNo ratings yet
- Prosthesis in Below Knee Amputation and Gait TrainingDocument34 pagesProsthesis in Below Knee Amputation and Gait TrainingSonal Khera100% (1)
- Survival in Long CaseDocument7 pagesSurvival in Long CaseRapid MedicineNo ratings yet
- Nursing Assessment New 1Document10 pagesNursing Assessment New 1smithapsNo ratings yet
- GUTDocument4 pagesGUTDarawan MirzaNo ratings yet
- HistoryDocument4 pagesHistoryAhmed ExaminationNo ratings yet
- Diagnosis in OrthopedicsDocument214 pagesDiagnosis in OrthopedicsMr. question100% (1)
- Report GordonsDocument23 pagesReport Gordonsdgreat16No ratings yet
- Gynec Ward Nursing Care PlanDocument8 pagesGynec Ward Nursing Care Plansuman guptaNo ratings yet
- Biodata of The PatientDocument8 pagesBiodata of The PatientRuchika KaushalNo ratings yet
- PaediatricsDocument8 pagesPaediatricsjhalakNo ratings yet
- Assessment Sheet Rev 2Document2 pagesAssessment Sheet Rev 2meghanNo ratings yet
- Physiotherapy Patient AssesementDocument4 pagesPhysiotherapy Patient AssesementsarikaNo ratings yet
- ThyroidDocument7 pagesThyroidTushar SahooNo ratings yet
- PPGMedical History FormDocument2 pagesPPGMedical History Formmb344617No ratings yet
- Orthopedics MalunionDocument4 pagesOrthopedics MalunionPravinNo ratings yet
- History Taking TemplateDocument6 pagesHistory Taking TemplateNooredin JomaaNo ratings yet
- GuideDocument4 pagesGuideMia Grace GarciaNo ratings yet
- History & Examination - FullDocument65 pagesHistory & Examination - FullCharithe Lakshithe ChandanayakeNo ratings yet
- Orthopedic Case Proformas-1Document19 pagesOrthopedic Case Proformas-1md maaz100% (1)
- History Taking FormatDocument10 pagesHistory Taking FormatMuskaan Deep100% (1)
- Anti Inflammatory Diet Cookbook: Inflammation Be Gone! - Complete Clean Eating Meal Plans To Reduce Inflammation and Promote Gut Healing With Healthy Keto Air Fryer RecipesFrom EverandAnti Inflammatory Diet Cookbook: Inflammation Be Gone! - Complete Clean Eating Meal Plans To Reduce Inflammation and Promote Gut Healing With Healthy Keto Air Fryer RecipesNo ratings yet
- The Arthritis Bible: A Comprehensive Guide to Alternative Therapies and Conventional Treatments for Arthritic Diseases Including Osteoarthrosis, Rheumatoid Arthritis, Gout, Fibromyalgia, and MoreFrom EverandThe Arthritis Bible: A Comprehensive Guide to Alternative Therapies and Conventional Treatments for Arthritic Diseases Including Osteoarthrosis, Rheumatoid Arthritis, Gout, Fibromyalgia, and MoreNo ratings yet
- Patellofemoral Pain Syndrome (Runner'S Knee)Document2 pagesPatellofemoral Pain Syndrome (Runner'S Knee)Dewi IrfanNo ratings yet
- 1 SMDocument9 pages1 SMMichael SiburianNo ratings yet
- Chapter-2 Review of Related LiteratureDocument36 pagesChapter-2 Review of Related LiteratureSumit SinghNo ratings yet
- Best Sports Bra (Category Relaxation and Wellness)Document21 pagesBest Sports Bra (Category Relaxation and Wellness)Iqra 2000No ratings yet
- Market Segmentation: Marketing PlanDocument5 pagesMarket Segmentation: Marketing PlanEll ElyanaNo ratings yet
- Geo Academic LiteracyDocument8 pagesGeo Academic LiteracyMOHAMMAD HADZRUL HASNAN BIN ABU HASSANNo ratings yet
- (Download PDF) A Treasury of Success Unlimited An Official Publication of The Napoleon Hill Foundation Og Mandino Editor Full Chapter PDFDocument69 pages(Download PDF) A Treasury of Success Unlimited An Official Publication of The Napoleon Hill Foundation Og Mandino Editor Full Chapter PDFnosdeouzzwal100% (12)
- Nichq Vanderbilt Parent Teacher SpanishDocument8 pagesNichq Vanderbilt Parent Teacher SpanishcolectivoeulaliazNo ratings yet
- Deloitte 2023 Genz Millennial Survey Mental HealthDocument25 pagesDeloitte 2023 Genz Millennial Survey Mental Healthdothu.ninhthuanNo ratings yet
- Cerebral Amyloid AngiopathyDocument2 pagesCerebral Amyloid AngiopathyPaolo Giordano100% (1)
- Safola PDFDocument7 pagesSafola PDFVibhuti BatraNo ratings yet
- CowspiracyDocument3 pagesCowspiracyNisah MacaronsingNo ratings yet
- Nursing Care of The Community CHP 7Document20 pagesNursing Care of The Community CHP 7marissaNo ratings yet
- IELTS Writing Task 2 2015 - 2016Document90 pagesIELTS Writing Task 2 2015 - 2016Khaing khant AungNo ratings yet
- Reflection No.7Document2 pagesReflection No.7Aldrin PabloNo ratings yet
- Defibrillation & DC Shock: Ns. Retno Setyawati, M.Kep., SP - KMBDocument34 pagesDefibrillation & DC Shock: Ns. Retno Setyawati, M.Kep., SP - KMBdanur ciyeeNo ratings yet
- Ed-Kidney StonesDocument2 pagesEd-Kidney StonesPearl NardoNo ratings yet
- PEBC Qualifying Exam References and Resources ListDocument5 pagesPEBC Qualifying Exam References and Resources ListAnkit ShahNo ratings yet
- Stretches - MenDocument2 pagesStretches - MenBahak AkbaNo ratings yet
- Drlee - Restless Leg SyndromeDocument1 pageDrlee - Restless Leg SyndromeSouheila MniNo ratings yet
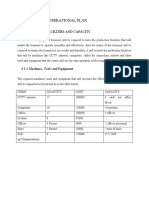
- Chapter Four: Operational Plan: 4.1 Production, Facilities and CapacityDocument4 pagesChapter Four: Operational Plan: 4.1 Production, Facilities and CapacityMonicah MuthokaNo ratings yet
- Introductory Lecture On Environment and HealthDocument18 pagesIntroductory Lecture On Environment and HealthDenmar GarciaNo ratings yet
- Safety Training Plan ExampleDocument2 pagesSafety Training Plan ExampleBilly Billy100% (1)
- Traditional BSN Degree Plan 2022 2023 202220Document1 pageTraditional BSN Degree Plan 2022 2023 202220Edgar MartínezNo ratings yet
- 26071-JO-HSE-020 Random Alcohol & Drug Test Form Rev1Document1 page26071-JO-HSE-020 Random Alcohol & Drug Test Form Rev1medicdaeah pkg3100% (1)
- Assessment of Knowledge and Attitude of Pharmacists Toward The Side Effects of Anesthetics in Patients With Hypertension: A Cross-Sectional StudyDocument9 pagesAssessment of Knowledge and Attitude of Pharmacists Toward The Side Effects of Anesthetics in Patients With Hypertension: A Cross-Sectional StudyMediterr J Pharm Pharm SciNo ratings yet
- Correlation Between Language Development and Motor Skills (Mulé Et Al., 2022)Document16 pagesCorrelation Between Language Development and Motor Skills (Mulé Et Al., 2022)Alberto I. Cruz FloresNo ratings yet