Download as pdf or txt
You might also like
- LS Magazine Ls Models Ls Land Issue Video LSM lsm09 08 02 Mega PDFDocument4 pagesLS Magazine Ls Models Ls Land Issue Video LSM lsm09 08 02 Mega PDFPaul25% (4)
- The Lean Product Design and Development Journey: Marcus Vinicius Pereira Pessôa Luís Gonzaga TrabassoDocument319 pagesThe Lean Product Design and Development Journey: Marcus Vinicius Pereira Pessôa Luís Gonzaga Trabassormfdiniz100% (2)
- Air Sampling Procedures To Evaluate Microbial ContaminationDocument6 pagesAir Sampling Procedures To Evaluate Microbial Contaminationsusana.duarte.1979No ratings yet
- American Journal of Infection ControlDocument3 pagesAmerican Journal of Infection ControlIdier Javier Benavides AyalaNo ratings yet
- Microbial Air ContaminationDocument16 pagesMicrobial Air Contaminationsabir21No ratings yet
- Characteristics in HospitalDocument8 pagesCharacteristics in HospitalwilsonNo ratings yet
- Contaminated Air Conditioners As Potential Source For Contaminating Operation Theatre EnvironmentDocument4 pagesContaminated Air Conditioners As Potential Source For Contaminating Operation Theatre EnvironmentGarai SzabolcsNo ratings yet
- Air Quality - OR - TaiwanDocument6 pagesAir Quality - OR - TaiwanKanokwan BorwornphiphattanachaiNo ratings yet
- Pathogens 07 00071Document9 pagesPathogens 07 00071newnse2008No ratings yet
- Air SanitationDocument8 pagesAir SanitationVignesh ReddyNo ratings yet
- 3 Curtis Reductionof Particlesinthe ORusing CUVCJOA2017Document7 pages3 Curtis Reductionof Particlesinthe ORusing CUVCJOA2017hendraNo ratings yet
- Pemeriksaan Kualitas Udara Ruang Yang Berhubungan Dengan Angka Kuman Di Ruang Operasi Rumah Sakit Sumber Hidup Di Kota Ambon 2020Document9 pagesPemeriksaan Kualitas Udara Ruang Yang Berhubungan Dengan Angka Kuman Di Ruang Operasi Rumah Sakit Sumber Hidup Di Kota Ambon 2020tedilevinrarianNo ratings yet
- Limitations of Microbial Environmental Monitoring Methods in CleanroomsDocument13 pagesLimitations of Microbial Environmental Monitoring Methods in Cleanroomshealing hopeNo ratings yet
- Bactericidal Effects of Ozone in AirDocument15 pagesBactericidal Effects of Ozone in AirJose BecerrilNo ratings yet
- Research Proposal (Final)Document16 pagesResearch Proposal (Final)Martin ClydeNo ratings yet
- Building and Environment: Chien-Cheng Jung, Pei-Chih Wu, Chao-Heng Tseng, Huey-Jen SuDocument6 pagesBuilding and Environment: Chien-Cheng Jung, Pei-Chih Wu, Chao-Heng Tseng, Huey-Jen SuEmanuel RodriguesNo ratings yet
- Air SamplingDocument10 pagesAir SamplingBudiawan PramonoNo ratings yet
- A Cleaning and Calibration Method For The Spiropro Portable Spirometer'S Pneumotachometer Tube in A Remote Field StudyDocument10 pagesA Cleaning and Calibration Method For The Spiropro Portable Spirometer'S Pneumotachometer Tube in A Remote Field StudyMihai PetrescuNo ratings yet
- Commissioning of OTDocument4 pagesCommissioning of OTSandhya100% (1)
- Airborne Bacterial Dispersal During and After Dressing and Bed Changes On Burns PatientsDocument10 pagesAirborne Bacterial Dispersal During and After Dressing and Bed Changes On Burns Patientsicehorizon88No ratings yet
- Overview of Inhalation ToxicologyDocument8 pagesOverview of Inhalation ToxicologySneha KadamNo ratings yet
- Development of An Automated Wet Cyclone System For Rapid 2019 Sensors and ADocument9 pagesDevelopment of An Automated Wet Cyclone System For Rapid 2019 Sensors and Asunil kumarNo ratings yet
- Environmental SamplingDocument5 pagesEnvironmental Samplings01223145725No ratings yet
- Closed Vs Open SuctionDocument5 pagesClosed Vs Open SuctionKhushboo DurejaNo ratings yet
- Analysis of Volatile Organic Compounds From Deep Airway in The Lung Through Intubation SamplingDocument12 pagesAnalysis of Volatile Organic Compounds From Deep Airway in The Lung Through Intubation SamplingmoubarginNo ratings yet
- Dingemans 2018Document9 pagesDingemans 2018angelica barrazaNo ratings yet
- Jurnal Nebulizer VentilatorDocument10 pagesJurnal Nebulizer VentilatorDessyani WulandariNo ratings yet
- Microbiological Commissioning and MonitoringDocument28 pagesMicrobiological Commissioning and MonitoringSungkakNo ratings yet
- Hospital Diffusers EngineeringDocument26 pagesHospital Diffusers Engineeringamechmar5935100% (1)
- Byssinosis and Other Respiratory Symptoms Among Factory Workers in Akaki Textile Factory, EthiopiaDocument7 pagesByssinosis and Other Respiratory Symptoms Among Factory Workers in Akaki Textile Factory, EthiopiaBunga RamadhaniNo ratings yet
- Indoor Air Quality Varies With Ventilation Types and Working Areasin HospitalsDocument7 pagesIndoor Air Quality Varies With Ventilation Types and Working Areasin HospitalsosaidsrourNo ratings yet
- ASHRAE D RP397 198507 Airbone Bacteria in SchoolsDocument26 pagesASHRAE D RP397 198507 Airbone Bacteria in SchoolsWalterNo ratings yet
- Sterilization and Surveillance of Operation Theatres in Developing WorldDocument5 pagesSterilization and Surveillance of Operation Theatres in Developing Worldtummalapalli venkateswara raoNo ratings yet
- Syed Moied Ahmed, Et AlDocument5 pagesSyed Moied Ahmed, Et AlAnca Ignat-SâncrăianNo ratings yet
- JHI Laminar Airflow Versus Turbulent Airflow in Simulated Total Hip Arthroplasty PIIS0195670121002425Document7 pagesJHI Laminar Airflow Versus Turbulent Airflow in Simulated Total Hip Arthroplasty PIIS0195670121002425Anders ENo ratings yet
- Ventilation Rates and Airflow Pathways in Patient Rooms: A Case Study of Bioaerosol Containment and RemovalDocument11 pagesVentilation Rates and Airflow Pathways in Patient Rooms: A Case Study of Bioaerosol Containment and RemovalPatricia TungpalanNo ratings yet
- Effect of Closed Suctioning On Reducing The Contamination Released Into The EnvironmentDocument4 pagesEffect of Closed Suctioning On Reducing The Contamination Released Into The EnvironmentM.Ichwan RijaniNo ratings yet
- A Numerical Investigation About The Air Quality in A Surgical Room at A HospitalDocument135 pagesA Numerical Investigation About The Air Quality in A Surgical Room at A HospitalHoàn LộcNo ratings yet
- Fluorescent Reconstitution On Deposition of PM2.5 inDocument6 pagesFluorescent Reconstitution On Deposition of PM2.5 inAD DNo ratings yet
- 10067-Article Text-35882-1-10-20200527Document8 pages10067-Article Text-35882-1-10-20200527MeryNo ratings yet
- Technical Performance Analysis of Different TypesDocument8 pagesTechnical Performance Analysis of Different Typesjuliocesar.ecNo ratings yet
- 3013 11254 1 PB PDFDocument6 pages3013 11254 1 PB PDFRenanda PrihastinaNo ratings yet
- Endotoxinas 1Document9 pagesEndotoxinas 1Carlos Israel Esparza AndradeNo ratings yet
- Inactivation of Airborne Microorganisms Using Novel Ultraviolet Radiation Sources in Reflective Flow Through Control DevicesDocument11 pagesInactivation of Airborne Microorganisms Using Novel Ultraviolet Radiation Sources in Reflective Flow Through Control DevicesMeduNo ratings yet
- Ventilation Performance in The Operating Theatre Against Airborne Infection Numerical Study On An Ultra-Clean SystemDocument10 pagesVentilation Performance in The Operating Theatre Against Airborne Infection Numerical Study On An Ultra-Clean SystemVL KohNo ratings yet
- Effect of Laminar Air Flow and Door Openings On Operating Room ContaminationDocument4 pagesEffect of Laminar Air Flow and Door Openings On Operating Room ContaminationAbed NaemNo ratings yet
- Air Cleaning TechnologiesDocument40 pagesAir Cleaning TechnologiesMichael LagundinoNo ratings yet
- 1 s2.0 S0195670118305425 MainDocument4 pages1 s2.0 S0195670118305425 MainMuhammad Cholid AlfahroziNo ratings yet
- UntitledDocument3 pagesUntitledShobha KunduNo ratings yet
- Building and Environment: Minki Sung, Shinsuke KatoDocument7 pagesBuilding and Environment: Minki Sung, Shinsuke KatoImran AzizNo ratings yet
- Aspergillus Fumigatus During COPD Exacerbation: A Pair-Matched Retrospective StudyDocument8 pagesAspergillus Fumigatus During COPD Exacerbation: A Pair-Matched Retrospective StudyJames 'jps' SimanjuntakNo ratings yet
- Analysis of The Microbiota of The Physiotherapist's EnvironmentDocument7 pagesAnalysis of The Microbiota of The Physiotherapist's EnvironmentmarychelNo ratings yet
- Pengaruh Kualitas Udara Dalam RuanganDocument10 pagesPengaruh Kualitas Udara Dalam RuanganYusTika KusumawardaniNo ratings yet
- Laminar Flow in Orthopaedic Operations - Essential If You CanDocument15 pagesLaminar Flow in Orthopaedic Operations - Essential If You CanSamiYousifNo ratings yet
- Revision Literaria ComparativaDocument11 pagesRevision Literaria ComparativaGeral FonsecaNo ratings yet
- In Vitro Evaluation of Aerosol Delivery - Complementaria - Semana 3Document7 pagesIn Vitro Evaluation of Aerosol Delivery - Complementaria - Semana 3natalia muñozNo ratings yet
- Komesaroff 1996 Disposable and Autoclavable Anaesthetic Circuits The Future Is NowDocument3 pagesKomesaroff 1996 Disposable and Autoclavable Anaesthetic Circuits The Future Is Nows01223145725No ratings yet
- Laboratory For Air Sterilization: Equipment FilteringDocument3 pagesLaboratory For Air Sterilization: Equipment Filteringredwan_rnNo ratings yet
- Anae 15542Document8 pagesAnae 15542Ervin SeborgaNo ratings yet
- 3D Lung Models for Regenerating Lung TissueFrom Everand3D Lung Models for Regenerating Lung TissueGunilla Westergren-ThorssonNo ratings yet
- Lung Function Testing in the 21st Century: Methodologies and Tools Bridging Engineering to Clinical PracticeFrom EverandLung Function Testing in the 21st Century: Methodologies and Tools Bridging Engineering to Clinical PracticeNo ratings yet
- Nontuberculous Mycobacteria (NTM): Microbiological, Clinical and Geographical DistributionFrom EverandNontuberculous Mycobacteria (NTM): Microbiological, Clinical and Geographical DistributionNo ratings yet
- 19 Cheese As A Food IngredientDocument32 pages19 Cheese As A Food IngredientEduardo MendozaNo ratings yet
- ENV ISO 13843 (2001) - (E) - CodifiedDocument8 pagesENV ISO 13843 (2001) - (E) - CodifiedEduardo MendozaNo ratings yet
- 22 Whey and Whey ProductsDocument9 pages22 Whey and Whey ProductsEduardo MendozaNo ratings yet
- Ilnas-En Iso 14698-2:2003Document6 pagesIlnas-En Iso 14698-2:2003Eduardo MendozaNo ratings yet
- 7 Post CoagulationDocument15 pages7 Post CoagulationEduardo MendozaNo ratings yet
- 21 Nutritional Aspects of CheeseDocument10 pages21 Nutritional Aspects of CheeseEduardo MendozaNo ratings yet
- 6 Enzymatic Coagulation of Milk Part IIDocument18 pages6 Enzymatic Coagulation of Milk Part IIEduardo MendozaNo ratings yet
- 6 Enzymatic Coagulation of Milk Part IDocument23 pages6 Enzymatic Coagulation of Milk Part IEduardo MendozaNo ratings yet
- 8 Salting of Cheese CurdDocument16 pages8 Salting of Cheese CurdEduardo MendozaNo ratings yet
- Actinomycetes: Source, Identification, and Their ApplicationsDocument33 pagesActinomycetes: Source, Identification, and Their ApplicationsEduardo MendozaNo ratings yet
- NIWAtr 121Document63 pagesNIWAtr 121Eduardo MendozaNo ratings yet
- Nauplii Counting ProcedureDocument1 pageNauplii Counting ProcedureEduardo MendozaNo ratings yet
- 2 STR ArtifactsDocument6 pages2 STR ArtifactsEduardo MendozaNo ratings yet
- Multiplex PCR Critical Parameters and Step-By-step ProtocolDocument8 pagesMultiplex PCR Critical Parameters and Step-By-step ProtocolVerônica Duda100% (1)
- Uncertainty in Most Probable Number Calculations FDocument6 pagesUncertainty in Most Probable Number Calculations FEduardo MendozaNo ratings yet
- 385 FullDocument8 pages385 FullEduardo MendozaNo ratings yet
- Margo Lanagan - Sea Hearts (Extract)Document7 pagesMargo Lanagan - Sea Hearts (Extract)Allen & UnwinNo ratings yet
- Cat C32 ACERT Spec Sheet - Pleasure CraftDocument8 pagesCat C32 ACERT Spec Sheet - Pleasure CraftSteven Wong100% (1)
- A320 Standardization FLOWSDocument24 pagesA320 Standardization FLOWSAlex SilvestreNo ratings yet
- A Playwriting Technique To Engage On A Shared Reflective Enquiry PDFDocument10 pagesA Playwriting Technique To Engage On A Shared Reflective Enquiry PDFEduardo orozco oteroNo ratings yet
- Tascam Us2400 ManualDocument24 pagesTascam Us2400 ManualDiego Guirado JimenezNo ratings yet
- Samsung SH09xWH SH12xWH SERVICE MANUALDocument46 pagesSamsung SH09xWH SH12xWH SERVICE MANUALIoannis Perperis100% (1)
- Smart System For Potholes Detection Using Computer Vision With Transfer LearningDocument9 pagesSmart System For Potholes Detection Using Computer Vision With Transfer LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Endocrain Systm Question 1 ST DayDocument15 pagesEndocrain Systm Question 1 ST DayJohn AjishNo ratings yet
- Module Week 9Document3 pagesModule Week 9Hanz Kirby Reyes FranciaNo ratings yet
- Abruptio PlacentaDocument20 pagesAbruptio PlacentaHizkia Mangaraja Hasiholan LimNo ratings yet
- A Review On AI Vision Robotic Arm Using Raspberry PiDocument7 pagesA Review On AI Vision Robotic Arm Using Raspberry PiIJRASETPublicationsNo ratings yet
- D4 InfanciaDocument3 pagesD4 InfanciaPedroPocasNo ratings yet
- Spec Sheet Scania R730la4x2mnaDocument4 pagesSpec Sheet Scania R730la4x2mnaRoman PopulikNo ratings yet
- Michael Ruse - Evolutionary Biology and The Question of TeleologyDocument7 pagesMichael Ruse - Evolutionary Biology and The Question of TeleologyradichoNo ratings yet
- Principles and Interpretation of CardiotocographyDocument9 pagesPrinciples and Interpretation of CardiotocographyCKNo ratings yet
- The 10 Biggest Business Trends For 2021 Everyone Must Be Ready ForDocument1 pageThe 10 Biggest Business Trends For 2021 Everyone Must Be Ready ForJUAN SEBASTIAN ARTEAGA MUÑOZNo ratings yet
- Pre Loading Condition SurveyDocument16 pagesPre Loading Condition Surveymax.pitchiah100% (1)
- Cambridge Secondary 1 Checkpoint: Cambridge Assessment International EducationDocument7 pagesCambridge Secondary 1 Checkpoint: Cambridge Assessment International Educationigloo79No ratings yet
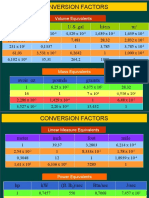
- Conversion Factors: in FT U.S. Gal Liters MDocument8 pagesConversion Factors: in FT U.S. Gal Liters MSamuel MahendraNo ratings yet
- European Standard Norme Européenne Europäische Norm: Final Draft Fpren 15316-4-5Document30 pagesEuropean Standard Norme Européenne Europäische Norm: Final Draft Fpren 15316-4-5raduvlasaNo ratings yet
- GY 112 Lecture NotesDocument13 pagesGY 112 Lecture NotesSyed Jabed Miadad AliNo ratings yet
- Assessment and Transportation Risk-1Document7 pagesAssessment and Transportation Risk-1TanzeemNo ratings yet
- ASPRI ForecastDocument17 pagesASPRI Forecastavs2020No ratings yet
- 1250 Red MSDSDocument4 pages1250 Red MSDSkwerwaNo ratings yet
- Live Pig MarketsDocument25 pagesLive Pig MarketsKoffee FarmerNo ratings yet
- BSC 116 SyllabusDocument8 pagesBSC 116 SyllabussahanchemNo ratings yet
- Reality Shifting ResearchDocument7 pagesReality Shifting ResearchMc Cruzt KristoferNo ratings yet
- Stem 2c-Music On Plant Growth FinalDocument91 pagesStem 2c-Music On Plant Growth FinalYonaNo ratings yet