Download as pdf or txt
You might also like
- ArizonaDocument2 pagesArizonaJesus SaenzNo ratings yet
- GCash Merchant Application Form v2Document2 pagesGCash Merchant Application Form v2Erwil Angelo Bangco Sanico100% (1)
- Casual Automobile (Non-Dealer) Purchase Agreement and Seller Proof-of-Ownership InformationDocument2 pagesCasual Automobile (Non-Dealer) Purchase Agreement and Seller Proof-of-Ownership InformationValiciaNo ratings yet
- Langkawi Auto Express SDN BHD: Vehicle Details FormDocument1 pageLangkawi Auto Express SDN BHD: Vehicle Details Formgnaners0% (1)
- Umbana Maria Christma Case Study - ProteinDocument3 pagesUmbana Maria Christma Case Study - ProteinGrace Umbaña YangaNo ratings yet
- Arizona - AZ-DMV-Form-96-0236Document2 pagesArizona - AZ-DMV-Form-96-0236Supratik MukhotiNo ratings yet
- Accident Report FormDocument3 pagesAccident Report FormJohn Matthew Ongoco RaymundoNo ratings yet
- Arkansas Crash ReportDocument6 pagesArkansas Crash Reportjdp135No ratings yet
- Reliancegeneral - Co.in 1800 3009 4890 3009: Motor Claim FormDocument4 pagesReliancegeneral - Co.in 1800 3009 4890 3009: Motor Claim FormAL SHEIKHNo ratings yet
- VSA 14 Application For Registration PDFDocument2 pagesVSA 14 Application For Registration PDFRoman JanjuliaNo ratings yet
- Here Fold Report of Motor Vehicle Accident: Reset/clearDocument2 pagesHere Fold Report of Motor Vehicle Accident: Reset/clearWashington IrvingNo ratings yet
- DTOP-776 SOL FOR MOTOR VEHICLE REGISTRATION Rev. June 14, 2010Document2 pagesDTOP-776 SOL FOR MOTOR VEHICLE REGISTRATION Rev. June 14, 2010ScribdTranslationsNo ratings yet
- Delaware - Applicatio For Title mv212 - Application - For - TitleDocument2 pagesDelaware - Applicatio For Title mv212 - Application - For - TitleSupratik MukhotiNo ratings yet
- Certificate of Title and Registration: Application ForDocument2 pagesCertificate of Title and Registration: Application ForGlendaNo ratings yet
- HDFC ERGO General Insurance Company Limited: Motor Insurance Claim FormDocument4 pagesHDFC ERGO General Insurance Company Limited: Motor Insurance Claim FormNìkhíl HonêyNo ratings yet
- Motor Accident Report FormDocument4 pagesMotor Accident Report FormLidia MagureanuNo ratings yet
- Customer Application FormDocument4 pagesCustomer Application Formoeruel bautistaNo ratings yet
- XTRAPOWER Application FormDocument5 pagesXTRAPOWER Application FormbiswajitNo ratings yet
- ITD 3738 (RevDocument1 pageITD 3738 (Revthornockjoe84No ratings yet
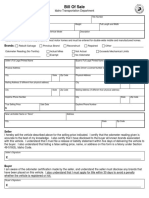
- Bill of Sale Template 05Document1 pageBill of Sale Template 05أديلسون الفاماNo ratings yet
- MV 359Document4 pagesMV 359Shawn StevensNo ratings yet
- 1799 - Vehicle Application (R0118)Document2 pages1799 - Vehicle Application (R0118)sarapreppyhandbookNo ratings yet
- Louisiana DuplicateDocument2 pagesLouisiana Duplicateperezhola287No ratings yet
- QM8273-0422 Motorcycle Claim Non Theft - WebDocument5 pagesQM8273-0422 Motorcycle Claim Non Theft - WebMichaelNo ratings yet
- Please Attach An Clear Copy of Licence: Claim FormDocument3 pagesPlease Attach An Clear Copy of Licence: Claim FormMpho Daniel PuleNo ratings yet
- JPSA Complete Electronically JMPD DateOKDocument2 pagesJPSA Complete Electronically JMPD DateOKYasmin CotwalNo ratings yet
- Department of State Growth: Application For RegistrationDocument1 pageDepartment of State Growth: Application For Registrationdibesh dhakalNo ratings yet
- 420001Document1 page420001DjNo ratings yet
- DMV Form 1799 0805Document2 pagesDMV Form 1799 0805darkhorse35No ratings yet
- Education Loan Application FormDocument6 pagesEducation Loan Application FormJap KhambholiyaNo ratings yet
- INVOICE For Car RepairDocument1 pageINVOICE For Car RepaircplNo ratings yet
- Js by Ms PDFDocument202 pagesJs by Ms PDFMultan Singh BhatiNo ratings yet
- Motor Claim FormDocument2 pagesMotor Claim FormMultan Singh BhatiNo ratings yet
- PR22005 Car Shield - Private Car Package Policy Proposal Form - Set 1Document4 pagesPR22005 Car Shield - Private Car Package Policy Proposal Form - Set 1Rajiv SethNo ratings yet
- Auto Claim FormDocument3 pagesAuto Claim FormdawnNo ratings yet
- Claim Form - Motor Insurance - 2021Document2 pagesClaim Form - Motor Insurance - 2021RavichandranMuthuswamyNo ratings yet
- Application For Texas Cerificate of TitleDocument2 pagesApplication For Texas Cerificate of TitleRobert CookNo ratings yet
- MSME Loan Application Form - Partnership - 1 PagerDocument2 pagesMSME Loan Application Form - Partnership - 1 Pagernambi2rajanNo ratings yet
- Spot survey report formatDocument6 pagesSpot survey report formatdeven gcNo ratings yet
- Spot Survey Report FormatDocument6 pagesSpot Survey Report FormatPankaj GuptaNo ratings yet
- Request For InvestigationDocument1 pageRequest For Investigationlane.moreau29No ratings yet
- 2 - Accident - Incident Report FormsDocument4 pages2 - Accident - Incident Report Formsantorcha0226No ratings yet
- Export Invoice Format 04Document2 pagesExport Invoice Format 04khund sayeedNo ratings yet
- Secure Finance Application - IndividualDocument1 pageSecure Finance Application - Individualdon.omar199028100% (1)
- HERCOPNFRM01-Account ApplicationDocument4 pagesHERCOPNFRM01-Account ApplicationMurad HassanNo ratings yet
- Diagram C A NorthwindDocument1 pageDiagram C A NorthwindAn KhangNo ratings yet
- Consolidated Application FormDocument9 pagesConsolidated Application FormPSC.CLAIMS1No ratings yet
- Consolidated Application Form 2023Document11 pagesConsolidated Application Form 2023Charlie CharlieNo ratings yet
- Personal Loan Form Form New To Bdo Client Jul 2022Document7 pagesPersonal Loan Form Form New To Bdo Client Jul 2022delmontecarlofNo ratings yet
- Vehicle Registration: Applicant DetailsDocument2 pagesVehicle Registration: Applicant DetailsAlyssa LNo ratings yet
- South Carolina Department of Motor Vehicles: Title ApplicationDocument2 pagesSouth Carolina Department of Motor Vehicles: Title Applicationbweaver700No ratings yet
- Motor Claim FormDocument4 pagesMotor Claim FormYash SharmaNo ratings yet
- Vehicle Certificate of Ownership (Title) ApplicationDocument1 pageVehicle Certificate of Ownership (Title) ApplicationBranden FieldNo ratings yet
- Proforma Invoice With Delivery ChargesDocument1 pageProforma Invoice With Delivery Chargesakunkosongfirst01No ratings yet
- Business License ApplicationDocument2 pagesBusiness License ApplicationmieNo ratings yet
- Application Form PDFDocument4 pagesApplication Form PDFTushar RathoreNo ratings yet
- Loan Application Form of DMI Housing Finance Pvt. Ltd.Document4 pagesLoan Application Form of DMI Housing Finance Pvt. Ltd.DMI HousingNo ratings yet
- Application Form DMIDocument5 pagesApplication Form DMIRohit KumarNo ratings yet
- Everthing You Need To Know To Start An Auto DealershipFrom EverandEverthing You Need To Know To Start An Auto DealershipRating: 5 out of 5 stars5/5 (1)
- Nepal Macroeconomic Update 202209 PDFDocument30 pagesNepal Macroeconomic Update 202209 PDFRajendra NeupaneNo ratings yet
- Mla EssayDocument6 pagesMla Essayapi-534405877No ratings yet
- Polymer Materials From Recycled Plastic in Road ConstructionDocument7 pagesPolymer Materials From Recycled Plastic in Road ConstructionYuv RajNo ratings yet
- Push Up GuideDocument11 pagesPush Up GuideRafaela NarbaesNo ratings yet
- 3rd Year-Cblm-AutoDocument163 pages3rd Year-Cblm-Autoapi-240274945100% (5)
- Research Report On Safai Karamcharis PDFDocument40 pagesResearch Report On Safai Karamcharis PDFAshish PansareNo ratings yet
- Common Pediatric Fractures Common Pediatric FracturesDocument67 pagesCommon Pediatric Fractures Common Pediatric FracturesJeane SuyantoNo ratings yet
- MCCB Catalogue PDFDocument84 pagesMCCB Catalogue PDFSudipta ChatterjeeNo ratings yet
- Dent MatDocument8 pagesDent MatBea YmsnNo ratings yet
- Analysis of The Effects of Broken Family On Ourl Lady of Fatima UniversityDocument10 pagesAnalysis of The Effects of Broken Family On Ourl Lady of Fatima UniversityMark Angelo MacedaNo ratings yet
- Basics of Voice CultureDocument3 pagesBasics of Voice CultureNehaDesaiNo ratings yet
- Worksheet 25 - 26 - 3rd - MSP - EDocument8 pagesWorksheet 25 - 26 - 3rd - MSP - EMelissaNo ratings yet
- Conscientious Objector Info Pack Part 2Document194 pagesConscientious Objector Info Pack Part 2Shot_infoNo ratings yet
- Consumer Buying Behaviours Towards Organised Retail OutletsDocument97 pagesConsumer Buying Behaviours Towards Organised Retail OutletsAMITAVA ROY86% (22)
- ICA Electrochemical finaLLLLLLLLLDocument8 pagesICA Electrochemical finaLLLLLLLLLTehmasipNo ratings yet
- Catalogo SiouxDocument13 pagesCatalogo Siouxdef2009100% (1)
- Mrs. Annapurna TiwariDocument15 pagesMrs. Annapurna Tiwarikuruvagadda sagarNo ratings yet
- Masters of The House (Fitch 8 June 2005) A Review of UK RMBS Master Trusts PDFDocument32 pagesMasters of The House (Fitch 8 June 2005) A Review of UK RMBS Master Trusts PDFfodriscollNo ratings yet
- Gender Based CounsellingDocument5 pagesGender Based CounsellingUnnimaya M SNo ratings yet
- IPC (White Spirit Assignment)Document7 pagesIPC (White Spirit Assignment)Humaira AtharNo ratings yet
- Vehicle Inspection Checklist PDFDocument9 pagesVehicle Inspection Checklist PDFSampahNo ratings yet
- Singer BangladeshDocument16 pagesSinger BangladeshMahbubur RahmanNo ratings yet
- Presentation No. 2 - Sensory ImageryDocument8 pagesPresentation No. 2 - Sensory Imageryandie hinchNo ratings yet
- Principles of Electric Circuits, Conventional Flow, 9 EdDocument24 pagesPrinciples of Electric Circuits, Conventional Flow, 9 EdYodel RamírezNo ratings yet
- The Therapist Within You: A Handbook of Kinesiology Self-Therapy With The Pendulum - Jonathan LivingstoneDocument5 pagesThe Therapist Within You: A Handbook of Kinesiology Self-Therapy With The Pendulum - Jonathan LivingstonegihasaryNo ratings yet
- Cementitious Slurries From CeresitDocument7 pagesCementitious Slurries From CeresitMostafa Hussein AbdouNo ratings yet
- De Jong 2013 ACS Catalysis Catalysts For Production of Lower Olefins From Synthesis Gas - A Review PDFDocument20 pagesDe Jong 2013 ACS Catalysis Catalysts For Production of Lower Olefins From Synthesis Gas - A Review PDFSohail FarooqNo ratings yet
- Psychological First Aid Field Operations Guide - 2nd Edition (2007)Document189 pagesPsychological First Aid Field Operations Guide - 2nd Edition (2007)api-279694446No ratings yet
- Eng 1 - PPT 11Document20 pagesEng 1 - PPT 11Kimberly CastilloNo ratings yet