Download as pdf or txt
You might also like
- Biology Essay 1 - How Energy Is Transferred Within and Between OrganismsDocument3 pagesBiology Essay 1 - How Energy Is Transferred Within and Between OrganismsEva Dewsbury100% (3)
- CRH Cellular Respiration (Principles) - Measure Energy Consumption During Exercise Lab ManualDocument6 pagesCRH Cellular Respiration (Principles) - Measure Energy Consumption During Exercise Lab ManualVanesha AnesNo ratings yet
- Insulin in DiabetesDocument19 pagesInsulin in Diabeteseki_herawatiNo ratings yet
- Biochemical Importance of Carbohydrate (2015)Document38 pagesBiochemical Importance of Carbohydrate (2015)Agnes Treyssia SandewaNo ratings yet
- Nutrients 03 00735Document21 pagesNutrients 03 00735Yvett HorváthNo ratings yet
- DykensDocument5 pagesDykensy.lteifNo ratings yet
- BCH 220 - DR ErhunseDocument6 pagesBCH 220 - DR ErhunseSuccess OlamideNo ratings yet
- SooleandSweetman 2021 PlantMitochondria-SubstratesInhibitorsUncouplersDocument10 pagesSooleandSweetman 2021 PlantMitochondria-SubstratesInhibitorsUncouplersIsabelle_BebelleNo ratings yet
- 10 Catabolism Reading ModuleDocument33 pages10 Catabolism Reading ModuleSebastian SmytheNo ratings yet
- CHP 5 Major Metabolic PathwaysDocument53 pagesCHP 5 Major Metabolic PathwaysAmrNo ratings yet
- Cellular MetabolismDocument4 pagesCellular Metabolismjanenathaneattl1No ratings yet
- Fot 247Document26 pagesFot 247Malini KolekarNo ratings yet
- HHS Public Access: Mitochondrial Energetics in The KidneyDocument40 pagesHHS Public Access: Mitochondrial Energetics in The KidneyDe La Torre Corral UrielNo ratings yet
- Carbohydrates Metabolism1Document61 pagesCarbohydrates Metabolism1Santino MajokNo ratings yet
- Detection of Hypoxia at Cellular LevelDocument13 pagesDetection of Hypoxia at Cellular LevelapippasaNo ratings yet
- Student Book 2Document101 pagesStudent Book 2helena coelho odaNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument25 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For Scientistsmuhammad irwanNo ratings yet
- Bio Final SRWRDocument7 pagesBio Final SRWRgdapbbbsybsuusrgnwNo ratings yet
- Retrotope - Deuterated Polyunsaturated Fatty Acids - RT001Document13 pagesRetrotope - Deuterated Polyunsaturated Fatty Acids - RT001crackintheshatNo ratings yet
- Hsslive-xi-botany-RESPIRATION IN PLANTS-8Document7 pagesHsslive-xi-botany-RESPIRATION IN PLANTS-8diyakozhimalaNo ratings yet
- GENERAL BIOLOGY Q2 WEEK 6 Glycolysis and Kreb CycleDocument14 pagesGENERAL BIOLOGY Q2 WEEK 6 Glycolysis and Kreb CycleAryan Jovic DomingoNo ratings yet
- Neurochemistry Lecture IDocument40 pagesNeurochemistry Lecture Iniyutns3005No ratings yet
- Đề sinh hóa vấn đápDocument2 pagesĐề sinh hóa vấn đápNghĩa Bùi Lê QuangNo ratings yet
- UntitledDocument14 pagesUntitledSyafrianda PanggabeanNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument41 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsArya ChowdhuryNo ratings yet
- Carcinogenesis - Arno HelmbergDocument4 pagesCarcinogenesis - Arno HelmbergHafsah ShoaibNo ratings yet
- The Effects of Metabolic Toxins On The Process of Cellular RespirationDocument9 pagesThe Effects of Metabolic Toxins On The Process of Cellular RespirationMar RiahNo ratings yet
- BIOCHEMISTRY_LECTURES-CHO_MetabolismDocument71 pagesBIOCHEMISTRY_LECTURES-CHO_Metabolismowotiajoshua7No ratings yet
- Metabolism, Ubiquinone SynthesisDocument9 pagesMetabolism, Ubiquinone Synthesisfranciscrick69No ratings yet
- Review: Running Head: Nitric Oxide and Energy Balance in HypoxiaDocument70 pagesReview: Running Head: Nitric Oxide and Energy Balance in HypoxiaAprilihardini LaksmiNo ratings yet
- Plant MetabolismDocument15 pagesPlant Metabolismnegiineha2No ratings yet
- Tabken UwiwnDocument5 pagesTabken UwiwnquirkymaeeNo ratings yet
- Cemical Energy and ATP: ATP Is A Molecule With Three Phosphate Groups Attached To The EndDocument12 pagesCemical Energy and ATP: ATP Is A Molecule With Three Phosphate Groups Attached To The EndMhimi ViduyaNo ratings yet
- Lecture 13. Introduction To Metabolism: - Catabolism - Degradation - Anabolism (Aka Biosynthesis) - EnergyDocument20 pagesLecture 13. Introduction To Metabolism: - Catabolism - Degradation - Anabolism (Aka Biosynthesis) - EnergyAnonymous Bh9NrU77No ratings yet
- Revision List - HL Topic 8: 8.1 MetabolismgDocument3 pagesRevision List - HL Topic 8: 8.1 MetabolismgFULYA YALDIZNo ratings yet
- Mitochondrial Respiration and Redox Coupling in Articular ChondrocytesDocument14 pagesMitochondrial Respiration and Redox Coupling in Articular ChondrocytesndsjNo ratings yet
- Biology 2nd QRTR Exam - OutlineDocument5 pagesBiology 2nd QRTR Exam - OutlineLouie Joice MartinezNo ratings yet
- Nutritional Support in Intensive Care Unit (ICU) PatientsDocument20 pagesNutritional Support in Intensive Care Unit (ICU) PatientssarahNo ratings yet
- Elemental Composition of BacteriaDocument11 pagesElemental Composition of Bacteriaishmist04No ratings yet
- 2-Energy and RespirationDocument34 pages2-Energy and RespirationLisa DentonNo ratings yet
- Ori Hofmekler - Warrior NewsletterDocument49 pagesOri Hofmekler - Warrior NewsletterBigNat7774100% (2)
- Role of Uncoupling Proteins in CancerDocument25 pagesRole of Uncoupling Proteins in CancerkpsantanaNo ratings yet
- Glucose As A Major Antioxidant - When, What For and Why It FailsDocument20 pagesGlucose As A Major Antioxidant - When, What For and Why It FailsDaniel GilbertoNo ratings yet
- Biology Unit 4 TOPIC 5: PhotosynthesisDocument8 pagesBiology Unit 4 TOPIC 5: PhotosynthesisSamara HusainNo ratings yet
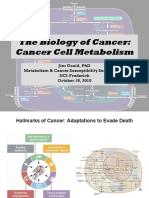
- The Biology of Cancer: Cancer Cell MetabolismDocument33 pagesThe Biology of Cancer: Cancer Cell MetabolismSYED RAZVINo ratings yet
- Approved BiochemDocument4 pagesApproved BiochemTempo RaryNo ratings yet
- Briefly Summarize The Involving Steps in The ATP SynthesisDocument7 pagesBriefly Summarize The Involving Steps in The ATP SynthesisXuân ViNo ratings yet
- Role of MitochondriaDocument57 pagesRole of MitochondriaPrecious AdeshinaNo ratings yet
- Cell Bio1Document11 pagesCell Bio1ghadiabdallah135No ratings yet
- Biology The Essentials 1st Edition Hoefnagels Solutions Manual DownloadDocument15 pagesBiology The Essentials 1st Edition Hoefnagels Solutions Manual DownloadGraham Hissem100% (26)
- Cell MetabolismDocument10 pagesCell Metabolismbenishgulzar50No ratings yet
- Molecules 27 07052Document20 pagesMolecules 27 07052Chris SmithNo ratings yet
- Module 8 Metabolic Pathways Final 1Document56 pagesModule 8 Metabolic Pathways Final 1Susana N peNo ratings yet
- tmpC00F TMPDocument7 pagestmpC00F TMPFrontiersNo ratings yet
- HanooDocument8 pagesHanoomr samoNo ratings yet
- The Human Bodys Energy MetabolismDocument39 pagesThe Human Bodys Energy MetabolismMasturina MarsyaNo ratings yet
- AlmostDocument7 pagesAlmostLumiereNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument24 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsEcaterina Borovic-PavlovschiNo ratings yet
- A-level Biology Revision: Cheeky Revision ShortcutsFrom EverandA-level Biology Revision: Cheeky Revision ShortcutsRating: 5 out of 5 stars5/5 (5)
- 26-1966-Dowsil-51-Additive - 3298Document5 pages26-1966-Dowsil-51-Additive - 3298Zhan FangNo ratings yet
- PP Compound 4Document2 pagesPP Compound 4Aparesh GantaitNo ratings yet
- Regulations of The International Chemistry Olympiad (Icho) : General StatementDocument16 pagesRegulations of The International Chemistry Olympiad (Icho) : General StatementKiệt LýNo ratings yet
- Cell Membrane StructureDocument9 pagesCell Membrane StructureBeyhNo ratings yet
- Carbonated Hydroxyapatite - Materials, Synthesis, and Applications-Pan Stanford Publishing (2015) PDFDocument272 pagesCarbonated Hydroxyapatite - Materials, Synthesis, and Applications-Pan Stanford Publishing (2015) PDFKENAN ABBARANo ratings yet
- Pointers To Review in ScienceDocument2 pagesPointers To Review in ScienceButterNo ratings yet
- Usp-Nf - 661.1 - Materiales Plásticos de Construcción PDFDocument32 pagesUsp-Nf - 661.1 - Materiales Plásticos de Construcción PDFEliza LosadaNo ratings yet
- Aircraft CleaningDocument3 pagesAircraft CleaningNoorul QuamarNo ratings yet
- Past PaperDocument16 pagesPast PaperGuna VallabhNo ratings yet
- Saponification Practical ReportDocument6 pagesSaponification Practical ReportGilbert NdibeNo ratings yet
- Periodic Table Theory - EDocument24 pagesPeriodic Table Theory - EthinkiitNo ratings yet
- CHM100 Practice Exam 2Document8 pagesCHM100 Practice Exam 2Abdullah AltwirqiNo ratings yet
- Pilot Test: ScientificDocument12 pagesPilot Test: ScientificHomam MohammadNo ratings yet
- Elements of Construct-1Document6 pagesElements of Construct-1osangeo76No ratings yet
- BS en 12878 2014 Pigments For ColoringDocument34 pagesBS en 12878 2014 Pigments For ColoringPeter MohabNo ratings yet
- Plastic University MCQ MergedDocument13 pagesPlastic University MCQ MergedChota ChatriNo ratings yet
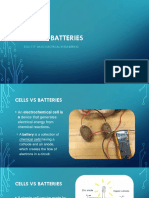
- Cells & BatteriesDocument37 pagesCells & BatteriesEsteban EroNo ratings yet
- Fine-tuning of the Stability of Β-strands by Y181 in Perfringolysin ODocument44 pagesFine-tuning of the Stability of Β-strands by Y181 in Perfringolysin OGeorgeNo ratings yet
- Chemistry Project 4Document25 pagesChemistry Project 4Aditi SinghNo ratings yet
- 2 - Principles of CorrosionDocument31 pages2 - Principles of CorrosionEngr. KafilNo ratings yet
- Presentation FTIR SpectDocument62 pagesPresentation FTIR SpectYogi IndrawanNo ratings yet
- Encyclopedia of Physical Science and TechnologyDocument495 pagesEncyclopedia of Physical Science and TechnologySomethingNo ratings yet
- STP ShaliFloor-SL-TC-4EDocument3 pagesSTP ShaliFloor-SL-TC-4ERana MahatoNo ratings yet
- Preparation and Study On Spectrum Characteristics of Sro.9, Ceosol Hf03 NanopowdersDocument4 pagesPreparation and Study On Spectrum Characteristics of Sro.9, Ceosol Hf03 NanopowdersIlse ArreolaNo ratings yet
- Substitution and EliminationDocument79 pagesSubstitution and Eliminationjana srutiNo ratings yet
- 64ecc6943427510018731934 - ## - Chemical Bonding Short NotesDocument2 pages64ecc6943427510018731934 - ## - Chemical Bonding Short NotesShlok MishraNo ratings yet
- Encapsulation in Food Industry With Emerging ElectrohydrodynamicDocument11 pagesEncapsulation in Food Industry With Emerging ElectrohydrodynamicRayito HernándezNo ratings yet
- Waukesha Digester GasDocument13 pagesWaukesha Digester GasA2 BhaskarNo ratings yet
- Test 34 - Redox Reactions - Middle of PyramidDocument6 pagesTest 34 - Redox Reactions - Middle of PyramidJay PatelNo ratings yet
- Nelson Mandela Secondary School Science Syllabus 5124 OutlineDocument4 pagesNelson Mandela Secondary School Science Syllabus 5124 OutlineMapalo Chirwa100% (1)