Download as pdf or txt
You might also like
- Secret Magic Spells of The Romany GypsiesDocument28 pagesSecret Magic Spells of The Romany Gypsiesakenaton4089% (66)
- Exercise Rehabilitation Assessment - Achilles Tendinopathy-1Document33 pagesExercise Rehabilitation Assessment - Achilles Tendinopathy-1GordonHessellNo ratings yet
- Chiropractic Treatment PlanDocument40 pagesChiropractic Treatment Planapi-542121685No ratings yet
- Manual Therapy: Ottar Vasseljen, Anne Margrethe FladmarkDocument8 pagesManual Therapy: Ottar Vasseljen, Anne Margrethe FladmarkSara AguiarNo ratings yet
- Le Exc PDFDocument6 pagesLe Exc PDFAshari Fisio18No ratings yet
- The Use of Kinesio Tape For Carpal Tunnel Syndrome: Mindy (Ming-Yao) Lou and Pou-Yu LeeDocument4 pagesThe Use of Kinesio Tape For Carpal Tunnel Syndrome: Mindy (Ming-Yao) Lou and Pou-Yu LeeAna Lu LoboNo ratings yet
- Muscular Pain & Kinesio® Taping: The Effect of Kinesio Taping® On Muscular Micro-Damage Following Eccentric ExercisesDocument7 pagesMuscular Pain & Kinesio® Taping: The Effect of Kinesio Taping® On Muscular Micro-Damage Following Eccentric ExercisesAna Lu LoboNo ratings yet
- Effectiveness of Eccentric Exercise in Tennis Elbow - A Single CaseDocument2 pagesEffectiveness of Eccentric Exercise in Tennis Elbow - A Single Caseirfan setiadiNo ratings yet
- Cervical StretchingDocument6 pagesCervical StretchingSulthan PhysioNo ratings yet
- Phreash Kosomak HospitalDocument3 pagesPhreash Kosomak Hospitalខៃសិញ- KhaisinhNo ratings yet
- Calmette HospitalDocument3 pagesCalmette Hospitalខៃសិញ- KhaisinhNo ratings yet
- Effects of the cervical flexion angle duringDocument3 pagesEffects of the cervical flexion angle duringl.cepeda01No ratings yet
- Sprain Ankle JurnalDocument9 pagesSprain Ankle JurnalRahmadanii RahmadaniiNo ratings yet
- Elektromigorafija Biomehanika Ozljeda EnglDocument8 pagesElektromigorafija Biomehanika Ozljeda EnglBorna MarinkovićNo ratings yet
- The Management of Tennis ElbowDocument6 pagesThe Management of Tennis ElbowPutu OkaNo ratings yet
- International Journal of Health Sciences and ResearchDocument8 pagesInternational Journal of Health Sciences and Researchrizk86No ratings yet
- Delayed Onset Muscle Soreness FSMDocument8 pagesDelayed Onset Muscle Soreness FSMmymar2400No ratings yet
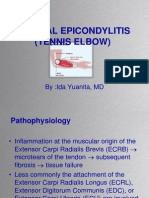
- Lateral Epicondylitis (Tennis Elbow) : By:Ida Yuanita, MDDocument37 pagesLateral Epicondylitis (Tennis Elbow) : By:Ida Yuanita, MDAnang FajarNo ratings yet
- Ankle&Foot TraumaDocument57 pagesAnkle&Foot TraumaJainil ParmarNo ratings yet
- Francis 2020 AchillesDocument10 pagesFrancis 2020 AchillespremtimNo ratings yet
- KINESIOTAPINGDocument130 pagesKINESIOTAPINGLiza Perez- PagatpatanNo ratings yet
- TableIssuID KG 18024ResMilitary005032403 - 231122 - 051611Document11 pagesTableIssuID KG 18024ResMilitary005032403 - 231122 - 051611diyamaan04No ratings yet
- ScaphoidhandoutDocument7 pagesScaphoidhandoutapi-282339623No ratings yet
- Clinical Case Studies ApoorvDocument47 pagesClinical Case Studies ApoorvApoorvNo ratings yet
- medip,+IJRMS-9044+O 240207 222626Document4 pagesmedip,+IJRMS-9044+O 240207 222626Rupanshi JaiswalNo ratings yet
- 11 (2) Effectiveness of Therapeutic Ultrasound and Kinesiotape in Treatment of Tennis Elbow (Jusmaniar) IIDocument9 pages11 (2) Effectiveness of Therapeutic Ultrasound and Kinesiotape in Treatment of Tennis Elbow (Jusmaniar) IIainunNo ratings yet
- Aquatic MyofascialDocument8 pagesAquatic MyofascialNaomiNo ratings yet
- Shruti RamekarDocument6 pagesShruti RamekarShruti RamekarNo ratings yet
- Effects of Tendon An Nerve Gliding Exercises and Instructions in Activities of Daily Livin Following Endoscopic Carpal Tunnel ReleaseDocument7 pagesEffects of Tendon An Nerve Gliding Exercises and Instructions in Activities of Daily Livin Following Endoscopic Carpal Tunnel ReleaseYimena JoyNo ratings yet
- Kinesio TapingDocument6 pagesKinesio TapingRJLeddaNo ratings yet
- Musculoskeletal Disorders Among Dentists and Variation in Dental WorkDocument7 pagesMusculoskeletal Disorders Among Dentists and Variation in Dental WorkHEMACHANDRAN GNo ratings yet
- 10 Jpts 27 1455Document3 pages10 Jpts 27 1455mustafasacarNo ratings yet
- Pectoralis Major Muscle Rupture Repair TechniqueDocument7 pagesPectoralis Major Muscle Rupture Repair Techniquedngt68w4z2No ratings yet
- Outpatients: Progress ReportDocument2 pagesOutpatients: Progress ReportemanNo ratings yet
- Pulsed Shortwave Diathermy and Joint Mobilizations Restore A Twice Fractured Elbow With Metal Implants To Full Range of MotionDocument7 pagesPulsed Shortwave Diathermy and Joint Mobilizations Restore A Twice Fractured Elbow With Metal Implants To Full Range of MotionIndah YulantariNo ratings yet
- Ulkus DekubitusDocument3 pagesUlkus DekubitusNanda RiftantiNo ratings yet
- Adaptação Do Tecido Tendíneo Ao Treinamento de Força de Contração Explosiva vs. SustentadaDocument17 pagesAdaptação Do Tecido Tendíneo Ao Treinamento de Força de Contração Explosiva vs. Sustentadaleal thiagoNo ratings yet
- ACL Rehabilitation Program Using A Combined Isokinetic and Isotonic Strengthening ProtocolDocument9 pagesACL Rehabilitation Program Using A Combined Isokinetic and Isotonic Strengthening Protocolchris waddleNo ratings yet
- Immediate and Short Term Effects of Short And.99146 PDFDocument6 pagesImmediate and Short Term Effects of Short And.99146 PDFAndy CrawfordNo ratings yet
- Effect of Mcconnell Taping On Pain, Rom & Grip Strength in Patients With Triangular Fibrocartilage Complex InjuryDocument9 pagesEffect of Mcconnell Taping On Pain, Rom & Grip Strength in Patients With Triangular Fibrocartilage Complex InjuryDr. Krishna N. SharmaNo ratings yet
- Colles's Fracture: B (Hons.) PhysiotherapyDocument36 pagesColles's Fracture: B (Hons.) PhysiotherapySafwan Idham RamlanNo ratings yet
- European J App Phys - Effectiveness of Using Wearable Vibration Therapy T PDFDocument9 pagesEuropean J App Phys - Effectiveness of Using Wearable Vibration Therapy T PDFFrancisco Javier Medina CaballeroNo ratings yet
- Elbow CasesDocument2 pagesElbow CasesBatool AliNo ratings yet
- Meniscopexy For Internal Derangement of Temporomandibular JointDocument5 pagesMeniscopexy For Internal Derangement of Temporomandibular Jointmehak malhotraNo ratings yet
- DenisaDocument7 pagesDenisaAmazonia clinicaNo ratings yet
- Epicondylitis Cyriax Physiotherapy For Tennis Elbow/lateral: Br. J. Sports MedDocument4 pagesEpicondylitis Cyriax Physiotherapy For Tennis Elbow/lateral: Br. J. Sports MedJohana Huichaqueo CurinNo ratings yet
- Isokinetic Strength Training of Kinetic Chain Exercises of A Professional Tennis Player With A Minor Partial Internal Abdominal Oblique Muscle TearDocument7 pagesIsokinetic Strength Training of Kinetic Chain Exercises of A Professional Tennis Player With A Minor Partial Internal Abdominal Oblique Muscle Tear壮No ratings yet
- Lateral Epicondylitis PresentationDocument16 pagesLateral Epicondylitis Presentationapi-317395769No ratings yet
- 29 - Jpts 2017 341Document4 pages29 - Jpts 2017 341Rafii KhairuddinNo ratings yet
- ESWT - For Myositis Ossificans CaseDocument13 pagesESWT - For Myositis Ossificans CaseSienriesta NovianaNo ratings yet
- PO reconstrução biceps distalDocument4 pagesPO reconstrução biceps distalricardo.albuquerque443No ratings yet
- PTH 890 - Case Report Poster 1Document1 pagePTH 890 - Case Report Poster 1api-551757456No ratings yet
- Kim Et. Al (2015)Document2 pagesKim Et. Al (2015)Mariana Oliveira e SilvaNo ratings yet
- Case Study - TrapeziectomyDocument14 pagesCase Study - Trapeziectomyapi-682945765No ratings yet
- Muscle Energy Technique: Concepts & MethodsDocument24 pagesMuscle Energy Technique: Concepts & MethodssandipandassarmaNo ratings yet
- Medical Engineering and PhysicsDocument5 pagesMedical Engineering and PhysicsValen ValenciaNo ratings yet
- Dynamic Splinting For Knee Flexion Contracture Following TKA A Case ReportDocument4 pagesDynamic Splinting For Knee Flexion Contracture Following TKA A Case ReportAdi WesnawaNo ratings yet
- An Adherent Nerve Root - Classification and Exercise Therapy in A PatientDocument4 pagesAn Adherent Nerve Root - Classification and Exercise Therapy in A PatientPablo Zamora MillanNo ratings yet
- Tibia Bone AnalysisDocument14 pagesTibia Bone AnalysisVasudev BansalNo ratings yet
- Short Versus Long Outcome RadiologisDocument7 pagesShort Versus Long Outcome Radiologisandy ardiansyahNo ratings yet
- Lilith Info PrayerDocument8 pagesLilith Info PrayerCarl MacCord100% (1)
- Trilateral Commission - Task Force On Global Capitalism in Transiiton - Report - June 2022 - FINALDocument56 pagesTrilateral Commission - Task Force On Global Capitalism in Transiiton - Report - June 2022 - FINALCarl MacCordNo ratings yet
- Easy Definition Spleen DeficiencyDocument19 pagesEasy Definition Spleen DeficiencyCarl MacCordNo ratings yet
- Binding and Separating PrayerDocument2 pagesBinding and Separating PrayerCarl MacCordNo ratings yet
- 8 Effective Acupressure Points For Lungs Recommended by TCM Practitioners - TCM TipsDocument25 pages8 Effective Acupressure Points For Lungs Recommended by TCM Practitioners - TCM TipsCarl MacCordNo ratings yet
- Market Research Small Business Development CorporationDocument6 pagesMarket Research Small Business Development CorporationCarl MacCordNo ratings yet
- Expel Mucus, Fight Respiratory Irritation With Mighty Mullein & GingerDocument8 pagesExpel Mucus, Fight Respiratory Irritation With Mighty Mullein & GingerCarl MacCordNo ratings yet
- Children in State Care Commission Inquiry 2004 2008Document5 pagesChildren in State Care Commission Inquiry 2004 2008Carl MacCordNo ratings yet
- Wind-Heat - Acupuncture PointsDocument19 pagesWind-Heat - Acupuncture PointsCarl MacCordNo ratings yet
- Poses To Expel Mucus From Your LungsDocument4 pagesPoses To Expel Mucus From Your LungsCarl MacCordNo ratings yet
- Phlegm in Chinese Medicine An Important Tale Teller - Acupuncture PointsDocument46 pagesPhlegm in Chinese Medicine An Important Tale Teller - Acupuncture PointsCarl MacCord100% (1)
- How To Treat Coughs by TCM and Acupuncture: Art of WellnessDocument12 pagesHow To Treat Coughs by TCM and Acupuncture: Art of WellnessCarl MacCordNo ratings yet
- How To Treat Increased Mucus in The LungsDocument15 pagesHow To Treat Increased Mucus in The LungsCarl MacCord100% (1)
- Liver Qi Stagnation Depression of Qi of Liver - Acupuncture PointsDocument26 pagesLiver Qi Stagnation Depression of Qi of Liver - Acupuncture PointsCarl MacCordNo ratings yet
- Using Herbs To Expel Parasite InfestationDocument5 pagesUsing Herbs To Expel Parasite InfestationCarl MacCordNo ratings yet
- Leaky Gut SyndromeDocument12 pagesLeaky Gut SyndromeCarl MacCordNo ratings yet
- Understanding Leaky Gut, Causes and TreatmentDocument4 pagesUnderstanding Leaky Gut, Causes and TreatmentCarl MacCordNo ratings yet
- The Gut and Parkinson's Disease Hype or Hope - PMCDocument14 pagesThe Gut and Parkinson's Disease Hype or Hope - PMCCarl MacCordNo ratings yet
- What To Know About Leaky Gut Syndrome.Document24 pagesWhat To Know About Leaky Gut Syndrome.Carl MacCordNo ratings yet
- Leaky Gut Causes and SolutionsDocument11 pagesLeaky Gut Causes and SolutionsCarl MacCordNo ratings yet
- The Brain Book Leaky Gut DietDocument4 pagesThe Brain Book Leaky Gut DietCarl MacCordNo ratings yet
- Heart Blood Stagnation or 'Stasis' - Acupuncture PointsDocument16 pagesHeart Blood Stagnation or 'Stasis' - Acupuncture PointsCarl MacCordNo ratings yet
- Qi Stagnation Foods - and Herbs - To Help or Avoid - Acupuncture PointsDocument37 pagesQi Stagnation Foods - and Herbs - To Help or Avoid - Acupuncture PointsCarl MacCordNo ratings yet
- Does Parkinson's Begin in The Gut - Scientific AmericanDocument5 pagesDoes Parkinson's Begin in The Gut - Scientific AmericanCarl MacCordNo ratings yet
- Leaky Gut Syndrome Symptoms, Diet, Tests & TreatmentDocument12 pagesLeaky Gut Syndrome Symptoms, Diet, Tests & TreatmentCarl MacCordNo ratings yet
- The Benefits of Red and Near-Infrared Light TherapyDocument10 pagesThe Benefits of Red and Near-Infrared Light TherapyCarl MacCordNo ratings yet
- Blood Stasis and What Does That MeanDocument2 pagesBlood Stasis and What Does That MeanCarl MacCordNo ratings yet
- Survey of Ticks of Companion AnimalsDocument10 pagesSurvey of Ticks of Companion AnimalsCarl MacCordNo ratings yet
- There Are Biophotons in The Brain. Is Something Light-Based Going On - Big ThinkDocument2 pagesThere Are Biophotons in The Brain. Is Something Light-Based Going On - Big ThinkCarl MacCordNo ratings yet
- Biophoton - WikipediaDocument6 pagesBiophoton - WikipediaCarl MacCordNo ratings yet
- Listening Test 11-16Document31 pagesListening Test 11-16Tuệ MinhNo ratings yet
- Bachelor of Science in Geodetic Engineering: First YearDocument2 pagesBachelor of Science in Geodetic Engineering: First YearRyleEmmanuelRaagasNo ratings yet
- Islamic WorldviewDocument74 pagesIslamic Worldviewvera290690100% (1)
- Chapter 2 Static and Dynamic Characteristics of SignalsDocument18 pagesChapter 2 Static and Dynamic Characteristics of SignalsDiyaa AhmedNo ratings yet
- Tech Guide To Filling MachinesDocument12 pagesTech Guide To Filling MachinesLatifani Ayu Chaerunnisa100% (1)
- Waves Solved QuestionsDocument27 pagesWaves Solved Questionscolorado wildernessNo ratings yet
- IQ SIL Option: IQ Actuators For Use in Applications Up To SIL 3Document12 pagesIQ SIL Option: IQ Actuators For Use in Applications Up To SIL 3Bolivar SuarezNo ratings yet
- CRV Led Spec SheetDocument3 pagesCRV Led Spec SheetGabrielGrecoNo ratings yet
- The Evolution of Water Reverse Osmosis TechnologyDocument35 pagesThe Evolution of Water Reverse Osmosis TechnologyQassim LaouiraNo ratings yet
- Silage Pile Sizing Documentation 5 12 2016 3Document9 pagesSilage Pile Sizing Documentation 5 12 2016 3Zaqueu Ferreira RodriguesNo ratings yet
- Fa 5541Document46 pagesFa 5541Ricardo Nicolau WerlangNo ratings yet
- Barang 3Document12 pagesBarang 3Sujoko SkinzNo ratings yet
- AC Adaptor For Blood Pressure Monitor / Nebulizer: - US VersionDocument1 pageAC Adaptor For Blood Pressure Monitor / Nebulizer: - US VersionJosé Carmelo Perales PecinaNo ratings yet
- Odontogenic Maxillary Sinusitis. Etiology, Anatomy, Pathogenesis, Classification, Clinical Picture, Diagnostics, Treatment and ComplicationsDocument36 pagesOdontogenic Maxillary Sinusitis. Etiology, Anatomy, Pathogenesis, Classification, Clinical Picture, Diagnostics, Treatment and ComplicationsАлександр ВолошанNo ratings yet
- What Is Price Skimming?: First MoverDocument9 pagesWhat Is Price Skimming?: First MoverDiya MukherjeeNo ratings yet
- Tea & TebDocument2 pagesTea & TebHadjer ZitouneNo ratings yet
- 9th Science Unit 01 Mcqs PTBDocument2 pages9th Science Unit 01 Mcqs PTBAsad IqbalNo ratings yet
- Presentation of Food Processing (FSSAI)Document32 pagesPresentation of Food Processing (FSSAI)Naincy Chhabra100% (1)
- Released FOR Manufacturing: 2509 ANTAMINA PERU SMC 100/14400 Truck Bridge Assembly Truck Bridge Steel Structure - RightDocument1 pageReleased FOR Manufacturing: 2509 ANTAMINA PERU SMC 100/14400 Truck Bridge Assembly Truck Bridge Steel Structure - RightCarlos ParedesNo ratings yet
- 2012 01 20 - Twogether32 EDocument76 pages2012 01 20 - Twogether32 Enivan009sku9645No ratings yet
- A Fatigue Damage Model of Composite MaterialsDocument4 pagesA Fatigue Damage Model of Composite MaterialsPrathamesh BilgundeNo ratings yet
- Playground Arduino CC Code NewPingDocument11 pagesPlayground Arduino CC Code NewPingimglobaltraders100% (1)
- Lab1 - ArrayDocument6 pagesLab1 - Arrayezz AymanNo ratings yet
- Bulwer-Lytton Edward - Vril The Power of The Coming RaceDocument128 pagesBulwer-Lytton Edward - Vril The Power of The Coming RaceMarcel PirardNo ratings yet
- Productsheet DionisosflowDocument1 pageProductsheet Dionisosflowabhishekmoharana5412No ratings yet
- 1SNC160001C0205 Cha1Document144 pages1SNC160001C0205 Cha1Nelson SilvaNo ratings yet
- The Indian School CLASS XI (2021-22) English Core (301) Worksheet 2Document2 pagesThe Indian School CLASS XI (2021-22) English Core (301) Worksheet 2Aakif RazaNo ratings yet
- 7 TH Biology Worksheets Ls 8 Weather, Climate Animal AdaptationsDocument7 pages7 TH Biology Worksheets Ls 8 Weather, Climate Animal AdaptationsAysha Muhammad ShahzadNo ratings yet
- Wastage of Food in Indian WeddingsDocument9 pagesWastage of Food in Indian WeddingsThe United IndianNo ratings yet