Download as pdf or txt
You might also like
- Hand TestDocument131 pagesHand Testnaboog_1000090% (52)
- Illustrated Rheumatology ExaminationDocument4 pagesIllustrated Rheumatology ExaminationHashraf Affendi50% (2)
- Term Protector Product Summary: Important NoteDocument8 pagesTerm Protector Product Summary: Important NotesoxoNo ratings yet
- Right Hemisphere Structures Predict Poststroke Speech FluencyDocument8 pagesRight Hemisphere Structures Predict Poststroke Speech FluencyRafaela SenaNo ratings yet
- Cognition in Friedreich AtaxiaDocument11 pagesCognition in Friedreich AtaxiaAlba PérezNo ratings yet
- Prefrontal Compensatory Mechanism May enDocument6 pagesPrefrontal Compensatory Mechanism May enAyestinNo ratings yet
- After Stroke Fmri and BehaviourDocument12 pagesAfter Stroke Fmri and Behaviourelizabethhanna045No ratings yet
- 2018 Motor and Cognitive Impairments in Spinocerebellar AtaxiaDocument14 pages2018 Motor and Cognitive Impairments in Spinocerebellar AtaxiaJefe de Escuela PsicologiaNo ratings yet
- D Esposito1996Document6 pagesD Esposito1996chuckNo ratings yet
- FABDocument4 pagesFABNadine SmithNo ratings yet
- tmpE48A TMPDocument14 pagestmpE48A TMPFrontiersNo ratings yet
- 2018SC 1 CompressedDocument13 pages2018SC 1 CompressedYolanda Gómez LópezNo ratings yet
- Bathla2019 2Document6 pagesBathla2019 2Manuel PerezNo ratings yet
- Comprehensive Assessment of Gesture Production: A New Test of Upper Limb Apraxia (TULIA)Document8 pagesComprehensive Assessment of Gesture Production: A New Test of Upper Limb Apraxia (TULIA)NoeliaSantosNo ratings yet
- AS144 - 02 Apr Il 3, 20 03 2 1:52 CH Ar Cou NT 0: STEELE Et AlDocument63 pagesAS144 - 02 Apr Il 3, 20 03 2 1:52 CH Ar Cou NT 0: STEELE Et AlTheodore FuscoNo ratings yet
- Imitating: Gestures Quantitative Approach ApraxiaDocument5 pagesImitating: Gestures Quantitative Approach ApraxiaJulian GorositoNo ratings yet
- Ideational Apraxia. A Deficit in Tool Selection and UseDocument4 pagesIdeational Apraxia. A Deficit in Tool Selection and UseAlejandro Israel Garcia EsparzaNo ratings yet
- Skeletal Open Bite-Cephalometric CharacteristicsDocument5 pagesSkeletal Open Bite-Cephalometric CharacteristicsZubair AhmedNo ratings yet
- Bimodal (Auditory and Visual) Left Frontoparietal Circuitry For Sensorimotor Integration and Sensorimotor LearningDocument9 pagesBimodal (Auditory and Visual) Left Frontoparietal Circuitry For Sensorimotor Integration and Sensorimotor LearningcokkyNo ratings yet
- Comparison of Japanese and European Overbite DepthDocument6 pagesComparison of Japanese and European Overbite DepthMirek SzNo ratings yet
- Falgàs 2019 - Comparison Between Visual and Quantitative Hippocampal Atrophy AssessmentDocument7 pagesFalgàs 2019 - Comparison Between Visual and Quantitative Hippocampal Atrophy AssessmentljdNo ratings yet
- 978 FullDocument8 pages978 FullGuisel Barría VargasNo ratings yet
- Raven Prabhakaran1997 PDFDocument21 pagesRaven Prabhakaran1997 PDFargiaescuNo ratings yet
- Can Impairment in Memory, Language and Executive Functions PredictDocument6 pagesCan Impairment in Memory, Language and Executive Functions PredictSebastian LiviuNo ratings yet
- Buxbaum 2018Document15 pagesBuxbaum 2018cah bagusNo ratings yet
- Use of Ultrasonography As A Diagnostic and Therapeutic ToolDocument11 pagesUse of Ultrasonography As A Diagnostic and Therapeutic ToolVojtěch ŠmídNo ratings yet
- Reduced White Matter Integrity in Antisocial Personality Disorder: A Diffusion Tensor Imaging StudyDocument11 pagesReduced White Matter Integrity in Antisocial Personality Disorder: A Diffusion Tensor Imaging StudyYeremias EdwinNo ratings yet
- 1 s2.0 S088761770100124X Main PDFDocument16 pages1 s2.0 S088761770100124X Main PDFFlorina AndreiNo ratings yet
- Effects oftDCS On Naming and e Cortical Exitability in Stoke Patients With AphasiaDocument6 pagesEffects oftDCS On Naming and e Cortical Exitability in Stoke Patients With AphasialabsoneducationNo ratings yet
- CurrOpinNeurol Koski v15p71Document7 pagesCurrOpinNeurol Koski v15p71andreaw80No ratings yet
- Thompson 1997Document1 pageThompson 1997Jocilene Dantas Torres NascimentoNo ratings yet
- Cavaillols1995 PDFDocument10 pagesCavaillols1995 PDFGad AliNo ratings yet
- California Verbal Learning Test: Performance by Patients With Focal Frontal and Non-Frontal LesionsDocument11 pagesCalifornia Verbal Learning Test: Performance by Patients With Focal Frontal and Non-Frontal LesionsAngela Bibiana Cañon OrtizNo ratings yet
- 2014-Criterios de APPDocument8 pages2014-Criterios de APPinternacionsjdNo ratings yet
- Fatigue in People Undergoing HemodialysisDocument5 pagesFatigue in People Undergoing Hemodialysistara rzNo ratings yet
- Asymmetry of The Face in Orthodontic PatientsDocument6 pagesAsymmetry of The Face in Orthodontic PatientsplsssssNo ratings yet
- Pantomime, Praxis, and AphasiaDocument17 pagesPantomime, Praxis, and AphasiadickyNo ratings yet
- Laryngeal Diadochokinesis Across The Adult LifespanDocument6 pagesLaryngeal Diadochokinesis Across The Adult Lifespanmajid mirzaeeNo ratings yet
- Cognitive FXN in PCADocument8 pagesCognitive FXN in PCAVincent OxenhamNo ratings yet
- Muscle Activity and Muscle Strength in Atypical Swallowing: Actividad Muscular y Fuerza Muscular en La Deglución AtípicaDocument12 pagesMuscle Activity and Muscle Strength in Atypical Swallowing: Actividad Muscular y Fuerza Muscular en La Deglución Atípicaalba farran martiNo ratings yet
- QEEG Spectral and Coherence Assessment of Autistic Children in Three Different Experimental ConditionsDocument19 pagesQEEG Spectral and Coherence Assessment of Autistic Children in Three Different Experimental ConditionsFrontiersNo ratings yet
- Construct Validity of The Trail Making Test: Role of Task-Switching, Working Memory, Inhibition/interference Control, and Visuomotor AbilitiesDocument13 pagesConstruct Validity of The Trail Making Test: Role of Task-Switching, Working Memory, Inhibition/interference Control, and Visuomotor AbilitiesPedro AlvesNo ratings yet
- Neuroimage: ClinicalDocument11 pagesNeuroimage: ClinicalPransiska Amabel CaritaNo ratings yet
- Visual Action Therapy For Global Aphasia VATDocument5 pagesVisual Action Therapy For Global Aphasia VATCristina Navarro RuizNo ratings yet
- 1969 Darley FL - Aronson AE, Brown JR - Clusters of Deviant Speech Dimensions in The DysarthriasDocument35 pages1969 Darley FL - Aronson AE, Brown JR - Clusters of Deviant Speech Dimensions in The DysarthriasLeticia LópezNo ratings yet
- Treatment of ApraxiaDocument41 pagesTreatment of ApraxiaanjelikaNo ratings yet
- Working Memory in Clinical Depression: An Experimental StudyDocument5 pagesWorking Memory in Clinical Depression: An Experimental StudysamiNo ratings yet
- Raven 2008Document6 pagesRaven 2008Jerrin JacobNo ratings yet
- Awl 160Document12 pagesAwl 160Hijaz HijaNo ratings yet
- Neurobiology of AgingDocument11 pagesNeurobiology of AgingLuis GómezNo ratings yet
- A Whole-Brain Computational Modeling Approach To Explain The AlterationsDocument12 pagesA Whole-Brain Computational Modeling Approach To Explain The AlterationsANTONIO REYES MEDINANo ratings yet
- An Acute Assessment of Post Stroke Aphasia-A Novel Tool For Bengali PopulationDocument6 pagesAn Acute Assessment of Post Stroke Aphasia-A Novel Tool For Bengali PopulationajmrdNo ratings yet
- Posters (Third Part) : SciencedirectDocument2 pagesPosters (Third Part) : SciencedirectshewaleakhileshNo ratings yet
- Detecting Neuronal Dysfunction of Hand Motor Cortex in ALS A MRSI StudyDocument7 pagesDetecting Neuronal Dysfunction of Hand Motor Cortex in ALS A MRSI StudyAri SamadNo ratings yet
- Anomia and ADDocument9 pagesAnomia and ADDaniel Londoño GuzmánNo ratings yet
- Electrophysiology in The Assessment of Fluency DisorderDocument13 pagesElectrophysiology in The Assessment of Fluency DisorderVijayNo ratings yet
- Study of Right Unilateral Spatial Neglect in Left Hemispheric Lesions: The Difference Between Right-Handed and Non-Right-Handed Post-Stroke PatientsDocument7 pagesStudy of Right Unilateral Spatial Neglect in Left Hemispheric Lesions: The Difference Between Right-Handed and Non-Right-Handed Post-Stroke Patientspokharelriwaj82No ratings yet
- ACEbajaeducacionDocument7 pagesACEbajaeducacionEuge López RuizNo ratings yet
- Treating Limb Apraxia Via Action SemanticsDocument19 pagesTreating Limb Apraxia Via Action SemanticsKryssiaNo ratings yet
- PAPER (ENG) - (Damasio A. R., 1983) The Anatomic Basis of Pure AlexiaDocument12 pagesPAPER (ENG) - (Damasio A. R., 1983) The Anatomic Basis of Pure AlexiaAldo Hip NaranjoNo ratings yet
- Defining Shoulder Function and Dysplasia in PatienDocument10 pagesDefining Shoulder Function and Dysplasia in PatienJoe ANo ratings yet
- Stevens' Handbook of Experimental Psychology and Cognitive Neuroscience, Sensation, Perception, and AttentionFrom EverandStevens' Handbook of Experimental Psychology and Cognitive Neuroscience, Sensation, Perception, and AttentionNo ratings yet
- Modelosd e LenguajeDocument5 pagesModelosd e LenguajeJulian GorositoNo ratings yet
- 2001 DaDocument9 pages2001 DaJulian GorositoNo ratings yet
- STIMA: A Short Screening Test For Ideo-Motor Apraxia, Selective For Action Meaning and Bodily DistrictDocument8 pagesSTIMA: A Short Screening Test For Ideo-Motor Apraxia, Selective For Action Meaning and Bodily DistrictJulian GorositoNo ratings yet
- A Cognitive Neuropsychological Model of LimbDocument16 pagesA Cognitive Neuropsychological Model of LimbJulian GorositoNo ratings yet
- Imitating: Gestures Quantitative Approach ApraxiaDocument5 pagesImitating: Gestures Quantitative Approach ApraxiaJulian GorositoNo ratings yet
- Deficient Body Structural DescriptionDocument10 pagesDeficient Body Structural DescriptionJulian GorositoNo ratings yet
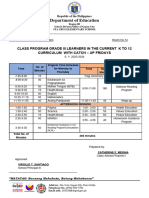
- Catch Up CLASS PROGRAM 2023 2024 1Document1 pageCatch Up CLASS PROGRAM 2023 2024 1Catherine Fajardo MesinaNo ratings yet
- Your Guide To Home Care Package ServicesDocument44 pagesYour Guide To Home Care Package ServicesSimran SekhonNo ratings yet
- 4 Ways of Creating and Ingesting MMS-CLO2 in A Nutshell, Ver. 2.0 (Based On 20 Drops Per ML) 30 Aug 2020Document2 pages4 Ways of Creating and Ingesting MMS-CLO2 in A Nutshell, Ver. 2.0 (Based On 20 Drops Per ML) 30 Aug 2020Scott McRaeNo ratings yet
- Concept MapDocument6 pagesConcept Mapmenickel3100% (1)
- Form - InternationalStudent - UMI - UNDERGRADUATE-SCHOLARSHIPDocument2 pagesForm - InternationalStudent - UMI - UNDERGRADUATE-SCHOLARSHIPRAHMAT ULLAHNo ratings yet
- 1.1 What Is Hum-WPS OfficeDocument7 pages1.1 What Is Hum-WPS OfficeJesie Bell Balaba BuroNo ratings yet
- MCQs On Disability 5 With AnswersDocument22 pagesMCQs On Disability 5 With AnswersAmee EdemNo ratings yet
- Hypothalamus, Limbic System, Emotion & MotivationDocument18 pagesHypothalamus, Limbic System, Emotion & MotivationdevdsantoshNo ratings yet
- Kierran Recorded Performance EvaluationDocument1 pageKierran Recorded Performance Evaluationapi-210660791No ratings yet
- Laboratory Activity No 2 - GLOVA-NDDocument4 pagesLaboratory Activity No 2 - GLOVA-NDandreyou99No ratings yet
- Case ReportDocument16 pagesCase ReportSabbir ThePsychoExpressNo ratings yet
- Project Proposal:: "Gas & Smoke/Fire Detector and Alarm"Document4 pagesProject Proposal:: "Gas & Smoke/Fire Detector and Alarm"Ihtisham HassanNo ratings yet
- Sun Pharmaceutical Industries LTD Vs DWD PharmaceuticalsDocument13 pagesSun Pharmaceutical Industries LTD Vs DWD PharmaceuticalsDeon FernandesNo ratings yet
- Holistic HealthDocument4 pagesHolistic HealthrodezaNo ratings yet
- Eating Disorders (All)Document11 pagesEating Disorders (All)Quỳnh LùnNo ratings yet
- 2019-09-01 Mens Health Singapore PDFDocument84 pages2019-09-01 Mens Health Singapore PDFaman singhNo ratings yet
- Basic Occupational Safety and Health TrainingDocument5 pagesBasic Occupational Safety and Health TrainingAUST BNo ratings yet
- Cognitive Behavioral TherapyDocument10 pagesCognitive Behavioral TherapySean Flanderhijn100% (2)
- Meddra Coding Basics WebinarDocument31 pagesMeddra Coding Basics WebinarAlexandraTomoiuNo ratings yet
- Controversias en La Insuficiencia Renal Aguda - Conclusiones Conferencia KDIGODocument29 pagesControversias en La Insuficiencia Renal Aguda - Conclusiones Conferencia KDIGOnanreNo ratings yet
- Eng CV Gabriella G - V1Document1 pageEng CV Gabriella G - V1Gabriella Gosling FantoniNo ratings yet
- Stop Remote Work Burnout British English TeacherDocument10 pagesStop Remote Work Burnout British English TeacherFiliberto ColamoreaNo ratings yet
- Detailed Procedure of Thematic Apperception Test - PsychestudyDocument1 pageDetailed Procedure of Thematic Apperception Test - PsychestudyShahab khalid MalikNo ratings yet
- Annual Gender and Development (Gad) Plan and Budget FY - : Lack of A Child Minding AreaDocument2 pagesAnnual Gender and Development (Gad) Plan and Budget FY - : Lack of A Child Minding AreaRojen YuriNo ratings yet
- Assertiveness Formative Questionnaire Technical Report: What This Questionnaire MeasuresDocument4 pagesAssertiveness Formative Questionnaire Technical Report: What This Questionnaire MeasuresKuldeep singh0% (1)
- Marketing Plan Project: Submitted To: Prof. Joydeep BiswasDocument15 pagesMarketing Plan Project: Submitted To: Prof. Joydeep Biswassubham chakrabortyNo ratings yet
- Unit 3 Facility Layout PlanningDocument31 pagesUnit 3 Facility Layout Planningnagpal0384No ratings yet