Download as pdf or txt
You might also like
- Fluids Concept MappingDocument1 pageFluids Concept Mappingmariagarcia415100% (1)
- Customer Service Responsibilities of Security GuardsDocument8 pagesCustomer Service Responsibilities of Security GuardsJoseMelarte GoocoJr.No ratings yet
- Clinical Log Term II PDFDocument9 pagesClinical Log Term II PDFPriscilla S100% (1)
- Ba GastrectomyDocument10 pagesBa GastrectomyHope3750% (2)
- STUDENT-Sepsis - Fundamental - Reasoning Fillable-1Document5 pagesSTUDENT-Sepsis - Fundamental - Reasoning Fillable-1Laura PoultneyNo ratings yet
- Open Book Examination: NeboshDocument8 pagesOpen Book Examination: NeboshZahir KhanNo ratings yet
- Hygiene (NCLEX) Flashcards - QuizletDocument5 pagesHygiene (NCLEX) Flashcards - QuizletA.No ratings yet
- VSim SARAH LIN For Nursing - Health Assessment POST QUIZDocument5 pagesVSim SARAH LIN For Nursing - Health Assessment POST QUIZWen RodsaNo ratings yet
- CHF Concept MapDocument4 pagesCHF Concept MapLisaSanders99No ratings yet
- Activity - PT - With - Fluid & Lyte ImbalanceDocument3 pagesActivity - PT - With - Fluid & Lyte ImbalanceAngel Joy CatalanNo ratings yet
- Fundamental Transition Goro Oishi 1Document66 pagesFundamental Transition Goro Oishi 1mp17570% (1)
- Nursing Care PlanDocument2 pagesNursing Care PlanAl RizkyNo ratings yet
- Urosepsis-Sepsis - (KeithRN-Unfolding THIGPEN PDFDocument11 pagesUrosepsis-Sepsis - (KeithRN-Unfolding THIGPEN PDFOLga A. Thigpen100% (4)
- Fluid Volume Deficit Nursing ManagementDocument5 pagesFluid Volume Deficit Nursing ManagementA.No ratings yet
- Hyponatremia, (Low Blood Sodium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHyponatremia, (Low Blood Sodium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Care Plan For Excess Fluid Volume ExampleDocument3 pagesCare Plan For Excess Fluid Volume ExampleVette Angelikka Dela CruzNo ratings yet
- Care Plan Exercise: Cristi Day RN, MSN, FNP-C Texas A&M University - Corpus ChristiDocument19 pagesCare Plan Exercise: Cristi Day RN, MSN, FNP-C Texas A&M University - Corpus ChristiPhyu Lin0% (1)
- CC Concept MapDocument9 pagesCC Concept Mapapi-606252228No ratings yet
- NANDA LIST of N.DiagnosesDocument3 pagesNANDA LIST of N.DiagnosesHasan KasiNo ratings yet
- Nursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Document9 pagesNursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Gayu Patel0% (1)
- Nursing DiagnosisDocument7 pagesNursing DiagnosisMariya Mikaela Garcia SoledadNo ratings yet
- NCP For Dehydration 1Document3 pagesNCP For Dehydration 1Khalid KhanNo ratings yet
- Concept Map Diagnosis and InterventionsDocument3 pagesConcept Map Diagnosis and Interventionsmenickel3No ratings yet
- CHF Cardiomegaly Volume OverloadDocument1 pageCHF Cardiomegaly Volume Overloadnursing concept mapsNo ratings yet
- NursingCare PlanDocument8 pagesNursingCare PlanSunSearra Kennedy RuffinNo ratings yet
- Nursing SkillDocument1 pageNursing SkillMarina Wasem NetzlaffNo ratings yet
- THE Check Principle Applied in Pharmacology: Remember To Take Your Tagamet With Meals!Document35 pagesTHE Check Principle Applied in Pharmacology: Remember To Take Your Tagamet With Meals!helloaNo ratings yet
- Heart Failure Care PlanDocument5 pagesHeart Failure Care PlanJustin StuartNo ratings yet
- Sepsis Is The Consequence of A Dysregulated Inflammatory Response To An Infectious InsultDocument11 pagesSepsis Is The Consequence of A Dysregulated Inflammatory Response To An Infectious InsultShrests SinhaNo ratings yet
- Assessment Dignosis Planning Implementation Evaluation: Nursing Process: What To Do AssessmentDocument5 pagesAssessment Dignosis Planning Implementation Evaluation: Nursing Process: What To Do AssessmentRgn McklNo ratings yet
- Careplan For Sickle Cell DiseaseDocument21 pagesCareplan For Sickle Cell DiseaseEcaroh Hew SmailliwNo ratings yet
- Decreased Cardiac Output RM 7Document9 pagesDecreased Cardiac Output RM 7api-283470660No ratings yet
- Understand Congestive Heart FailureDocument5 pagesUnderstand Congestive Heart FailureOanh HoangNo ratings yet
- Nursing Interventions CHFDocument3 pagesNursing Interventions CHFbanyenye25100% (1)
- Acute PyelonephritisDocument9 pagesAcute Pyelonephritistaekado-1No ratings yet
- SBAR Report To Physician About A Critical SitutionDocument3 pagesSBAR Report To Physician About A Critical SitutionRandolph DjanieNo ratings yet
- Basic Nursing NotesDocument4 pagesBasic Nursing Notesbonggoi100% (1)
- Impaired Physical MobilityDocument2 pagesImpaired Physical MobilityTyisha CharlesNo ratings yet
- HyponatremiaDocument19 pagesHyponatremiaapi-260357356No ratings yet
- Nursing Care Plan Renal FailureDocument18 pagesNursing Care Plan Renal FailureKundan KumarNo ratings yet
- Lewis Heart Failure Care PlanDocument4 pagesLewis Heart Failure Care Plansarahbearcoups100% (1)
- n360 Concept Map Care Plan Week 3 Sheryl SatoDocument15 pagesn360 Concept Map Care Plan Week 3 Sheryl Satoapi-283363983No ratings yet
- Urinary EliminationDocument5 pagesUrinary EliminationClarence ViboraNo ratings yet
- Hyponatremia and Hypernatremia in The ElderlyDocument15 pagesHyponatremia and Hypernatremia in The ElderlyStacey WoodsNo ratings yet
- Waiters Rhabdomyolysis PDFDocument1 pageWaiters Rhabdomyolysis PDFmp1757No ratings yet
- Heart Failure Care Plan LippincottDocument62 pagesHeart Failure Care Plan LippincottDyllano100% (1)
- Concept Map Worksheet Olivia Jones Jasgou1752Document2 pagesConcept Map Worksheet Olivia Jones Jasgou1752Jasmyn Rose100% (1)
- Nursing Care PlanDocument22 pagesNursing Care Planaln00550% (2)
- Acute and Chronic GastritisDocument6 pagesAcute and Chronic GastritisAnn CanNo ratings yet
- HypokalemiaDocument3 pagesHypokalemiaSergeiNo ratings yet
- CellulitisDocument12 pagesCellulitisAlma Bertos-Agub100% (1)
- Nursing Care Plans For UTIDocument2 pagesNursing Care Plans For UTIHannah Pin67% (3)
- Cardiovascular ADocument3 pagesCardiovascular AAutumn AllisonNo ratings yet
- Chronic Heart Failure ExacerbationDocument7 pagesChronic Heart Failure Exacerbationbarbara100% (5)
- End Stage Renal DiseaseDocument2 pagesEnd Stage Renal DiseaseAynie SuriagaNo ratings yet
- Plan of Care For:: Nursing Diagnosis: Excess Fluid VolumeDocument3 pagesPlan of Care For:: Nursing Diagnosis: Excess Fluid VolumeKenji CadizNo ratings yet
- Adult Care Plan Impair Gas ExchangeDocument2 pagesAdult Care Plan Impair Gas ExchangeVic DangNo ratings yet
- Activity Intolerance Care Plan For CFDocument8 pagesActivity Intolerance Care Plan For CFapi-314197645No ratings yet
- NCP On Decrease Cardiac OutputDocument1 pageNCP On Decrease Cardiac OutputHamayun KhanNo ratings yet
- Nursing Care Plan of Client With Fluid and Electrolyte ImbalanceDocument28 pagesNursing Care Plan of Client With Fluid and Electrolyte ImbalanceCj Aguilar50% (2)
- Atrial Fibrillation: Presented by ShehzadiDocument17 pagesAtrial Fibrillation: Presented by ShehzadisamNo ratings yet
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- Bronchospasm: Causes, Symptoms, and DiagnosisDocument8 pagesBronchospasm: Causes, Symptoms, and DiagnosisA.No ratings yet
- Termination During The Counseling Process: Function, Timing & Related IssuesDocument4 pagesTermination During The Counseling Process: Function, Timing & Related IssuesA.100% (1)
- Adult Asthma, Bronchospasm, Albuterol Inhaler: R:asthmaDocument2 pagesAdult Asthma, Bronchospasm, Albuterol Inhaler: R:asthmaA.No ratings yet
- What Does A Bronchospasm Feel Like?: R:asthmaDocument2 pagesWhat Does A Bronchospasm Feel Like?: R:asthmaA.No ratings yet
- What Are The 4 Types of Food Contamination? - Food Safety GuideDocument6 pagesWhat Are The 4 Types of Food Contamination? - Food Safety GuideA.No ratings yet
- What Is An Employee Assistance Program (EAP) ?Document2 pagesWhat Is An Employee Assistance Program (EAP) ?A.No ratings yet
- 5S Lean Methodology & Principles (Lean Manufacturing)Document23 pages5S Lean Methodology & Principles (Lean Manufacturing)A.No ratings yet
- Asthma Attack: Causes, Early Warning Signs, and TreatmentDocument4 pagesAsthma Attack: Causes, Early Warning Signs, and TreatmentA.No ratings yet
- 6.1 The Functions of The Skeletal System - Anatomy & PhysiologyDocument13 pages6.1 The Functions of The Skeletal System - Anatomy & PhysiologyA.No ratings yet
- Termination of Counseling - Syracuse University School of EducationDocument13 pagesTermination of Counseling - Syracuse University School of EducationA.100% (1)
- Termination in Therapy: The Art of Gently Letting Clients GoDocument20 pagesTermination in Therapy: The Art of Gently Letting Clients GoA.100% (1)
- Suspected Chronic RhinosinusitisDocument6 pagesSuspected Chronic RhinosinusitisA.No ratings yet
- 6 Strategies For Ethical Termination of Psychotherapy - Society For The Advancement of PsychotherapyDocument10 pages6 Strategies For Ethical Termination of Psychotherapy - Society For The Advancement of PsychotherapyA.No ratings yet
- Treatment of Chronic Rhinosinusitis With Nasal Polyposis With Oral Steroids Followed by Topical SteroidsDocument37 pagesTreatment of Chronic Rhinosinusitis With Nasal Polyposis With Oral Steroids Followed by Topical SteroidsA.No ratings yet
- International Consensus Statement On Allergy and Rhinology: RhinosinusitisDocument535 pagesInternational Consensus Statement On Allergy and Rhinology: RhinosinusitisA.No ratings yet
- Clinically Relevant Phenotypes in Chronic RhinosinusitisDocument22 pagesClinically Relevant Phenotypes in Chronic RhinosinusitisA.No ratings yet
- Pathogenesis of Chronic Rhinosinusitis With Nasal Polyps: Role of IL-6 in Airway Epithelial Cell DysfunctionDocument30 pagesPathogenesis of Chronic Rhinosinusitis With Nasal Polyps: Role of IL-6 in Airway Epithelial Cell DysfunctionA.No ratings yet
- Frontiers - Pathophysiological and Clinical Aspects of Chronic Rhinosinusitis: Current Concepts - AllergyDocument37 pagesFrontiers - Pathophysiological and Clinical Aspects of Chronic Rhinosinusitis: Current Concepts - AllergyA.No ratings yet
- Personal Hygiene: NCLEX-RNDocument8 pagesPersonal Hygiene: NCLEX-RNA.No ratings yet
- Full Article: Systematic Literature Review of The Epidemiology and Clinical Burden of Chronic Rhinosinusitis With Nasal PolyposisDocument58 pagesFull Article: Systematic Literature Review of The Epidemiology and Clinical Burden of Chronic Rhinosinusitis With Nasal PolyposisA.No ratings yet
- Postpartum Perineal Care (Aftercare Instructions) - What You Need To KnowDocument3 pagesPostpartum Perineal Care (Aftercare Instructions) - What You Need To KnowA.No ratings yet
- Personal Care - Foundations For Assisting in Home CareDocument104 pagesPersonal Care - Foundations For Assisting in Home CareA.No ratings yet
- Who Is Volodymyr Zelensky? What To Know About Ukraine's President - WSJDocument6 pagesWho Is Volodymyr Zelensky? What To Know About Ukraine's President - WSJA.0% (1)
- Who Is Volodymyr Zelenskyy, Europe's Most Vulnerable President? - Russia-Ukraine Crisis News - Al JazeeraDocument11 pagesWho Is Volodymyr Zelenskyy, Europe's Most Vulnerable President? - Russia-Ukraine Crisis News - Al JazeeraA.No ratings yet
- Assisting Patients With Personal Hygiene - StatPearls - NCBI BookshelfDocument7 pagesAssisting Patients With Personal Hygiene - StatPearls - NCBI BookshelfA.No ratings yet
- In Video, A Defiant President Zelensky Says, We Are Here' - The New York TimesDocument6 pagesIn Video, A Defiant President Zelensky Says, We Are Here' - The New York TimesA.No ratings yet
- How Ukraine's Volodymyr Zelensky Went From An Actor Playing President On TV To Defiant Wartime Leader - CNNDocument5 pagesHow Ukraine's Volodymyr Zelensky Went From An Actor Playing President On TV To Defiant Wartime Leader - CNNA.No ratings yet
- Ukraine's Volodymyr Zelensky: The Comedian President Who Is Rising To The Moment - BBC NewsDocument11 pagesUkraine's Volodymyr Zelensky: The Comedian President Who Is Rising To The Moment - BBC NewsA.No ratings yet
- Volodymyr Zelensky - Biography, Facts, Presidency, & Russian Invasion of Ukraine - BritannicaDocument10 pagesVolodymyr Zelensky - Biography, Facts, Presidency, & Russian Invasion of Ukraine - BritannicaA.No ratings yet
- COVID-19 Response Toolkit For New Mexico's Public SchoolsDocument29 pagesCOVID-19 Response Toolkit For New Mexico's Public SchoolsErika EsquivelNo ratings yet
- Chapter 2 - Market Analysis - Group 2Document26 pagesChapter 2 - Market Analysis - Group 2Allan AntonioNo ratings yet
- Sample SyllabusDocument9 pagesSample SyllabusRolalen Joyce C PaitonNo ratings yet
- Image Registration Pluim2003Document3 pagesImage Registration Pluim2003Fatemeh NaseriNo ratings yet
- Medical Surgical Nursing Care 3rd Edition Burke Test BankDocument8 pagesMedical Surgical Nursing Care 3rd Edition Burke Test BankMatthew Song100% (43)
- Lesson Plan Death CareDocument19 pagesLesson Plan Death CareLoma Waghmare (Jadhav)No ratings yet
- Journal Reading: "A Case of Hanging With Creeper in Secluded Place: Suicide or Homicide?"Document21 pagesJournal Reading: "A Case of Hanging With Creeper in Secluded Place: Suicide or Homicide?"Azam alausyNo ratings yet
- Unit 5 Teaching MethodologyDocument61 pagesUnit 5 Teaching MethodologyCeciliaNo ratings yet
- A. A. A. Abdel-KareemDocument17 pagesA. A. A. Abdel-KareemDRHAMADA ELWANNo ratings yet
- Presentation: Submitted To Ma'am Ayesha Sadaf Subject Media & SocietyDocument23 pagesPresentation: Submitted To Ma'am Ayesha Sadaf Subject Media & Societylaiba asadNo ratings yet
- Computer Hardware Servicing Detailed Lesson Plan FINALDocument13 pagesComputer Hardware Servicing Detailed Lesson Plan FINALWen AmbosNo ratings yet
- Textbook Harmal The Genus Peganum 1St Edition Ephraim Shmaya Lansky Ebook All Chapter PDFDocument53 pagesTextbook Harmal The Genus Peganum 1St Edition Ephraim Shmaya Lansky Ebook All Chapter PDFannette.hides846100% (15)
- HSG A12 721Document8 pagesHSG A12 721thuba71No ratings yet
- Egyptian Stories - Egypt Bottled Water - UNSAFEDocument4 pagesEgyptian Stories - Egypt Bottled Water - UNSAFEtefovNo ratings yet
- Textbook Gen64 125Document76 pagesTextbook Gen64 125Jiraporn AekkhamphanNo ratings yet
- Republic of The Philippines Region VII Central Visayas Division of Cebu Province Tambongon, San Remegio, CebuDocument7 pagesRepublic of The Philippines Region VII Central Visayas Division of Cebu Province Tambongon, San Remegio, CebuLenie PelegrinNo ratings yet
- Root Caries-From Prevalence To TherapyDocument150 pagesRoot Caries-From Prevalence To TherapyGeorgiana Ilinca100% (1)
- UntitledDocument2 pagesUntitledMerizah VillagraciaNo ratings yet
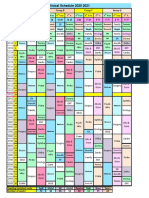
- R Schedule 2020 2021Document1 pageR Schedule 2020 2021Mohammed AhmedNo ratings yet
- Cat ReproductionDocument22 pagesCat ReproductionKatrina Ponce100% (1)
- Pediatric - Neuropsychology Cases LD PDFDocument27 pagesPediatric - Neuropsychology Cases LD PDFPsiho PupelNo ratings yet
- Principles of Topical Therapy: Presented By: DR .Anjali Singh Junior Resident Department of DermatologyDocument25 pagesPrinciples of Topical Therapy: Presented By: DR .Anjali Singh Junior Resident Department of DermatologyRiyaSinghNo ratings yet
- MSDS For 70% Isopropyl AlcoholDocument9 pagesMSDS For 70% Isopropyl AlcoholKiran ChakravarthulaNo ratings yet
- Twin Block LDDocument45 pagesTwin Block LDRahul Gote100% (1)
- Health Clinic Floor PlanDocument1 pageHealth Clinic Floor PlanSt_defalco5943No ratings yet
- Oxford Handbook of Rehabilitation Medicine 3rd Edition 2019Document689 pagesOxford Handbook of Rehabilitation Medicine 3rd Edition 2019suzzixx100% (1)
- CV - Mohamed Eltahhan-PDF - 2022-1Document3 pagesCV - Mohamed Eltahhan-PDF - 2022-1Mohamed EltahhanNo ratings yet
- Project PrimaryDocument7 pagesProject PrimaryLisanwork HonseboNo ratings yet