Download as pdf or txt
You might also like
- Rise of The Runelords (RotRL) D&D 5e ConversionDocument12 pagesRise of The Runelords (RotRL) D&D 5e Conversionhmareid100% (2)
- Case Scenario For Community Health NursingDocument5 pagesCase Scenario For Community Health Nursinghemihema100% (1)
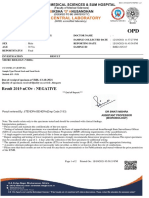
- Patient Name Doctor Name Pat Reg Id Sample Collected Date SEX Reporting Date AGE Sample Id ReportstatusDocument2 pagesPatient Name Doctor Name Pat Reg Id Sample Collected Date SEX Reporting Date AGE Sample Id ReportstatusThushar P kumarNo ratings yet
- Ayurveda On The Cusp of ChangeDocument24 pagesAyurveda On The Cusp of ChangeHemal Majithia100% (2)
- Feline Pancreatitis: ProfileDocument5 pagesFeline Pancreatitis: ProfileMiruna ChiriacNo ratings yet
- Chapter 31 - Nausea and VomitingDocument7 pagesChapter 31 - Nausea and Vomitingjonalyn.mejellanoNo ratings yet
- Understanding Medical Surgical Nursing - 0831-0831Document1 pageUnderstanding Medical Surgical Nursing - 0831-0831Anas TasyaNo ratings yet
- Causes and Treatment of Nausea and Vomiting: Aaron Bhakta and Rishi GoelDocument7 pagesCauses and Treatment of Nausea and Vomiting: Aaron Bhakta and Rishi GoelVini SasmitaNo ratings yet
- Disorder of The Pancreas and DMDocument27 pagesDisorder of The Pancreas and DMJoshoua MalanaNo ratings yet
- By DR.: Haitham Mokhtar Mohamed Abd AllahDocument101 pagesBy DR.: Haitham Mokhtar Mohamed Abd AllahMohamed ElkadyNo ratings yet
- Esophageal DisordersDocument37 pagesEsophageal DisordersDanielle FosterNo ratings yet
- Acute PancreatitisDocument12 pagesAcute Pancreatitissho bartNo ratings yet
- 13 Pancreatisis - FinalDocument34 pages13 Pancreatisis - FinalBrhanu belayNo ratings yet
- Feline Hepatic Lipidosis: How I TreatDocument8 pagesFeline Hepatic Lipidosis: How I TreatDavid OliveraNo ratings yet
- GI ReviewDocument44 pagesGI Reviews129682No ratings yet
- 3rd-Yr Revalida NotesDocument9 pages3rd-Yr Revalida NotesJazel RomanoNo ratings yet
- Pead 3 - Abdominal Pain and VommitingDocument22 pagesPead 3 - Abdominal Pain and Vommitingbbyes100% (1)
- Gastritis: Department of Gastroenterology General Hospital of Ningxia Medical University Si Cen MDDocument82 pagesGastritis: Department of Gastroenterology General Hospital of Ningxia Medical University Si Cen MDAvi Themessy100% (1)
- Lecture 1part 2Document50 pagesLecture 1part 2mashe1No ratings yet
- HematuriaDocument37 pagesHematuriaعبدالحكيم عمر عامر بن الزوعNo ratings yet
- PancreatitisDocument6 pagesPancreatitisreerwrr qeqweNo ratings yet
- Articulo Abdomen AgudoDocument12 pagesArticulo Abdomen AgudoAlejandra VelezNo ratings yet
- Surgery 2014.1Document25 pagesSurgery 2014.1Jayanti Neogi SardarNo ratings yet
- Acute Pancreatitis by Yuvaraj BSC Nursing Sec YearDocument9 pagesAcute Pancreatitis by Yuvaraj BSC Nursing Sec Yearvidhyasagar754No ratings yet
- Acute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CDocument29 pagesAcute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CEdelrose Lapitan100% (1)
- Nursing Care Plan For Inflammatory Bowel DiseaseDocument17 pagesNursing Care Plan For Inflammatory Bowel DiseaseLyka Joy DavilaNo ratings yet
- Case Analysis-Medicine-PancreatitisDocument39 pagesCase Analysis-Medicine-PancreatitisAleks MendozaNo ratings yet
- Pancreatitispptnitinm1st 181229090413Document58 pagesPancreatitispptnitinm1st 181229090413enam professorNo ratings yet
- Acute PancreatitisDocument11 pagesAcute Pancreatitispeter_soósNo ratings yet
- Salmonella, Campylobacter, and Mycobacterium TuberculosisDocument2 pagesSalmonella, Campylobacter, and Mycobacterium TuberculosisMalueth AnguiNo ratings yet
- Disorders of The StomachDocument26 pagesDisorders of The StomachAnnie Rose Dorothy MamingNo ratings yet
- Diarrhoea - MRCEM SuccessDocument7 pagesDiarrhoea - MRCEM SuccessGazi Sareem Bakhtyar AlamNo ratings yet
- Chronic PancreatitisDocument174 pagesChronic Pancreatitisdilekamunasinghe4No ratings yet
- Acute PancreatitisDocument25 pagesAcute PancreatitisSunil YadavNo ratings yet
- NCM 109 Maternal Lecture Lesson: CausesDocument2 pagesNCM 109 Maternal Lecture Lesson: CausesJanelle ArcillaNo ratings yet
- +nephrotic SyndromeDocument22 pages+nephrotic SyndromeDr. SAMNo ratings yet
- ConstipationDocument37 pagesConstipationHero StoreNo ratings yet
- Curs 2-3 2023Document115 pagesCurs 2-3 2023Andreea GuraliucNo ratings yet
- Mesay - Acute PancreatitisDocument67 pagesMesay - Acute PancreatitisMesay AssefaNo ratings yet
- Anorexia: Basic InformationDocument34 pagesAnorexia: Basic InformationcarlosNo ratings yet
- Pancreatitis PresentationDocument41 pagesPancreatitis Presentationak2621829No ratings yet
- Gastro Esophageal Reflux Disease (GERD)Document7 pagesGastro Esophageal Reflux Disease (GERD)MahaNo ratings yet
- Chapter 42: Nursing Management: Upper Gastrointestinal ProblemsDocument10 pagesChapter 42: Nursing Management: Upper Gastrointestinal ProblemsjefrocNo ratings yet
- Askep PankreatitisDocument48 pagesAskep PankreatitisYeni DwiNo ratings yet
- Acute Pancreatitis-A Clinical Update: Review ArticleDocument6 pagesAcute Pancreatitis-A Clinical Update: Review ArticleDương Ngọc DiệpNo ratings yet
- Approach To Vomiting: DR Vivek JhaDocument23 pagesApproach To Vomiting: DR Vivek JhaMukesh ThakurNo ratings yet
- Acute PancreatitisDocument2 pagesAcute PancreatitisChika JonesNo ratings yet
- Diseases of The Stomach:-ObjectivesDocument14 pagesDiseases of The Stomach:-Objectiveshussain AltaherNo ratings yet
- PancreatitisDocument18 pagesPancreatitisDr.Gutale AlmuqdishawiNo ratings yet
- Nur 322 Gi DisordersDocument113 pagesNur 322 Gi DisordersLovelights ZamoraNo ratings yet
- Study Guide 2 Management of Patients With Gastric, Intestinal and Colonic DisordersDocument19 pagesStudy Guide 2 Management of Patients With Gastric, Intestinal and Colonic DisordersKc Cabanilla LizardoNo ratings yet
- Hepatomegaly PDFDocument9 pagesHepatomegaly PDFKhadija IbrahimNo ratings yet
- Esophageal and Stomach Pathology-May+2019Document71 pagesEsophageal and Stomach Pathology-May+2019Karami Brutus0% (1)
- Problem 2 GI - VICKA AZWITADocument65 pagesProblem 2 GI - VICKA AZWITARana RickNo ratings yet
- Approach To The Infant or Child With Nausea and Vomiting - UpToDateDocument47 pagesApproach To The Infant or Child With Nausea and Vomiting - UpToDatemayteveronica1000No ratings yet
- Crohn's DiseaseDocument8 pagesCrohn's DiseaseShannen Madrid Tindugan100% (1)
- The Diseases of The PancreasDocument40 pagesThe Diseases of The PancreasAroosha IbrahimNo ratings yet
- Farmakologi Gastroenterohepatologi S1 FK Umi 09 June 2021Document23 pagesFarmakologi Gastroenterohepatologi S1 FK Umi 09 June 2021Fkumi 2019No ratings yet
- Zollinger-Ellison Syndrome - CASTILLO BELMARKDocument4 pagesZollinger-Ellison Syndrome - CASTILLO BELMARKBelmark CastilloNo ratings yet
- Sa Jun 2018 PDFDocument6 pagesSa Jun 2018 PDFdpcamposhNo ratings yet
- Printout Fever and Abd Pain - Causes and DiagnosiDocument10 pagesPrintout Fever and Abd Pain - Causes and DiagnosiMalar MannanNo ratings yet
- Nurseslabs Gi Diseases Nursing Quiz 4Document6 pagesNurseslabs Gi Diseases Nursing Quiz 4Yenny PepitoNo ratings yet
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Acute Gastrointestinal Bleeding: Diagnosis and TreatmentFrom EverandAcute Gastrointestinal Bleeding: Diagnosis and TreatmentKaren E. KimNo ratings yet
- Hammond Pierce 2023 Treatment of High Output Cardiac Failure Secondary To Anemia in Three CatsDocument5 pagesHammond Pierce 2023 Treatment of High Output Cardiac Failure Secondary To Anemia in Three CatsLorena TomoiagăNo ratings yet
- Sample ID Patient ID Name Test Date & Time 00518 2343 Susi 04 Mar. 2022 14:11 Mode Doctor Sex 360018736 Female LT CatDocument1 pageSample ID Patient ID Name Test Date & Time 00518 2343 Susi 04 Mar. 2022 14:11 Mode Doctor Sex 360018736 Female LT CatLorena TomoiagăNo ratings yet
- Sample ID Patient ID Name Test Date & Time 00514 1958 Smilla 03 Mar. 2022 12:09 Mode Doctor Sex 360018736 Female DogDocument1 pageSample ID Patient ID Name Test Date & Time 00514 1958 Smilla 03 Mar. 2022 12:09 Mode Doctor Sex 360018736 Female DogLorena TomoiagăNo ratings yet
- Sample ID Patient ID Name Test Date & Time 00512 2334 DOM 02 Mar. 2022 21:59 Mode Doctor Sex 360018736 Male Florin B DogDocument1 pageSample ID Patient ID Name Test Date & Time 00512 2334 DOM 02 Mar. 2022 21:59 Mode Doctor Sex 360018736 Male Florin B DogLorena TomoiagăNo ratings yet
- Sample ID Patient ID Name Test Date & Time 00515 2337 Ruru 03 Mar. 2022 13:46 Mode Doctor Sex 360018736 Female LT DogDocument1 pageSample ID Patient ID Name Test Date & Time 00515 2337 Ruru 03 Mar. 2022 13:46 Mode Doctor Sex 360018736 Female LT DogLorena TomoiagăNo ratings yet
- Chemical Coordination and Integration Handwriten Notes For Neet and JeeDocument5 pagesChemical Coordination and Integration Handwriten Notes For Neet and JeetechnosonicindiaNo ratings yet
- My LogDocument229 pagesMy Logsowpij290laslNo ratings yet
- Applying What We Know To Accelerate Cancer PreventionDocument10 pagesApplying What We Know To Accelerate Cancer PreventionSt. Louis Public RadioNo ratings yet
- Group 2 Case Study MergedDocument12 pagesGroup 2 Case Study MergedKobe Bryan GermoNo ratings yet
- Anatomy by DR Naser AlBarbariDocument24 pagesAnatomy by DR Naser AlBarbariTanmay JhulkaNo ratings yet
- Describe An Unpopular Opinion You Hold or HaveDocument4 pagesDescribe An Unpopular Opinion You Hold or Have091945029No ratings yet
- Latest Thesis. Rough Print12Document107 pagesLatest Thesis. Rough Print12Ajmal Hussain100% (1)
- Natural Aromatase InhibitorsDocument69 pagesNatural Aromatase InhibitorsIme Muško OsječkoNo ratings yet
- 2000+ MCQS With Solution: of Physics, Chemistry, Biology, Maths & EnglishDocument169 pages2000+ MCQS With Solution: of Physics, Chemistry, Biology, Maths & EnglishMuhammad UmairNo ratings yet
- Adolescence: Biosocial Development: The Developing Person Through AdolescenceDocument46 pagesAdolescence: Biosocial Development: The Developing Person Through AdolescenceHUMSS 12ANo ratings yet
- Final Research Essay DropboxDocument12 pagesFinal Research Essay Dropboxapi-584319388No ratings yet
- Hello Health, Goodbye Gray: Leslie KennyDocument9 pagesHello Health, Goodbye Gray: Leslie KennyfizzNo ratings yet
- Bronchial Asthma QuestionsDocument44 pagesBronchial Asthma QuestionsguevarrajanelleruthNo ratings yet
- Lecture 29 30 Thyroid TherapeuticsDocument3 pagesLecture 29 30 Thyroid TherapeuticsAhmed MashalyNo ratings yet
- Lesson 3 IncidenceDocument12 pagesLesson 3 IncidenceKaren RamirezNo ratings yet
- Psy 2300 Exam ReviewDocument101 pagesPsy 2300 Exam Reviewerica1960No ratings yet
- Rajiv Gandhi College of Nursing BSC Nursing 1St Year 2020 Fundamental of Nursing Pathology SetbDocument3 pagesRajiv Gandhi College of Nursing BSC Nursing 1St Year 2020 Fundamental of Nursing Pathology SetbNeenu RajputNo ratings yet
- The Anxiety Symptoms Among Chronic Kidney Disease Patients Who Undergo Hemodialysis TherapyDocument5 pagesThe Anxiety Symptoms Among Chronic Kidney Disease Patients Who Undergo Hemodialysis TherapyIJPHSNo ratings yet
- Cervical Cancer in PregnancyDocument21 pagesCervical Cancer in Pregnancymineresearch100% (1)
- Aktiviti Latihan Terapi AirDocument2 pagesAktiviti Latihan Terapi Airas-suhairiNo ratings yet
- StemBook 2011 FinalDocument187 pagesStemBook 2011 Finalskeebs23No ratings yet
- 10 Larva MigransDocument8 pages10 Larva MigransDaniel JohnsonNo ratings yet
- EtatDocument121 pagesEtatBhoja Raj GAUTAMNo ratings yet
- The Stolen Bacillus and Other Incidents by Wells, H. G. (Herbert George), 1866-1946Document127 pagesThe Stolen Bacillus and Other Incidents by Wells, H. G. (Herbert George), 1866-1946Gutenberg.org100% (1)
- English10 q4 CLAS3 Giving The Expanded Extended Definition of Words Final-Carissa-CalalinDocument13 pagesEnglish10 q4 CLAS3 Giving The Expanded Extended Definition of Words Final-Carissa-CalalinSophia Erika LargoNo ratings yet
- (Livestock Health Ii (Livestock Parasites)Document5 pages(Livestock Health Ii (Livestock Parasites)Brian BrianNo ratings yet