Download as pdf or txt
You might also like
- Cópia de Principles and Management of Pediatric Foot and Ankle Deformities and MalformationsDocument304 pagesCópia de Principles and Management of Pediatric Foot and Ankle Deformities and MalformationsJose Antonio PintoNo ratings yet
- Lower Limb: Muscle Charts: Cheat Sheet (Latin Terminology)Document9 pagesLower Limb: Muscle Charts: Cheat Sheet (Latin Terminology)ali reza khatibiNo ratings yet
- Gerbert Text Study GuideDocument54 pagesGerbert Text Study GuideAndrea RaeNo ratings yet
- Path StudyGuideDocument17 pagesPath StudyGuidehoatbuiNo ratings yet
- Clinical ExaminationDocument6 pagesClinical Examinationarvind appNo ratings yet
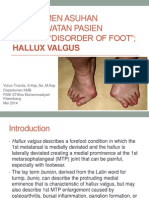
- Manajemen Asuhan Keperawatan Pasien Dengan Disorder of Foot Hammer Toe and Hallux Valgus FREEDocument29 pagesManajemen Asuhan Keperawatan Pasien Dengan Disorder of Foot Hammer Toe and Hallux Valgus FREENovita DamaiyantiNo ratings yet
- Foot Orthotics - FDLDocument19 pagesFoot Orthotics - FDLDiamoniq AyuningtiaNo ratings yet
- Leg and Ankle Problems in Primary Care: Briant W. Smith, MD Orthopedic Surgery TPMGDocument50 pagesLeg and Ankle Problems in Primary Care: Briant W. Smith, MD Orthopedic Surgery TPMGArmiya RamliNo ratings yet
- PPRP of Foot and Ankle: by Dr. Giridhar Boyapati PG Dept. of OrthopaedicsDocument62 pagesPPRP of Foot and Ankle: by Dr. Giridhar Boyapati PG Dept. of OrthopaedicsvaishnaviNo ratings yet
- TECH 524 - Palpation II (Castellucci) 9 2015Document12 pagesTECH 524 - Palpation II (Castellucci) 9 2015Robert StraubNo ratings yet
- 0 - Knee Joint AssessmentDocument4 pages0 - Knee Joint AssessmentAndrei MariusNo ratings yet
- Ankle Sprain TreatmentDocument5 pagesAnkle Sprain TreatmentTushar GajjarNo ratings yet
- Chapter 25 Pes Cavus: Complete Definition - Pes Cavus Is Primarily Sagittal Plane Deformity Consisting ofDocument11 pagesChapter 25 Pes Cavus: Complete Definition - Pes Cavus Is Primarily Sagittal Plane Deformity Consisting ofpoddataNo ratings yet
- Differential Diagnosis IIDocument32 pagesDifferential Diagnosis IIRaymondNo ratings yet
- Ankle&fEET Written Procedure-MagsombolDocument2 pagesAnkle&fEET Written Procedure-Magsombolhazell_aseronNo ratings yet
- Clinical Examination of The KneeDocument6 pagesClinical Examination of The KneeraniNo ratings yet
- Lauge Hansen1950Document29 pagesLauge Hansen1950DavidNo ratings yet
- Chapter 21: Surgery of The Congenital FootDocument30 pagesChapter 21: Surgery of The Congenital FootpoddataNo ratings yet
- Healing by Direct Union (Primary Bone Healing)Document6 pagesHealing by Direct Union (Primary Bone Healing)Cakradenta YPNo ratings yet
- Chapter14 MageeDocument32 pagesChapter14 Mageehis.thunder122100% (1)
- Presentor-Dr. Momin Mohammad Farhan Moderator-Dr. M. A. Q. AnsariDocument48 pagesPresentor-Dr. Momin Mohammad Farhan Moderator-Dr. M. A. Q. Ansarimohammad farhanNo ratings yet
- PrinciplesofOsteopathicMedicine PDFDocument5 pagesPrinciplesofOsteopathicMedicine PDFsuso73No ratings yet
- Hip PT AssessmentDocument57 pagesHip PT Assessmentkrissh20No ratings yet
- AMPUTATION Et ORTHOSISDocument6 pagesAMPUTATION Et ORTHOSISNysm NydNo ratings yet
- Malunion and Non-UnionDocument12 pagesMalunion and Non-UnionHengkai NeoNo ratings yet
- Concave Convex RulesDocument11 pagesConcave Convex RulesVénnì D Väliènt TámizhànNo ratings yet
- Knee Case Study 2Document3 pagesKnee Case Study 2superhoofy7186No ratings yet
- Lower Limb Neurological Examination OSCE GuideDocument15 pagesLower Limb Neurological Examination OSCE GuideLeen abusarhanNo ratings yet
- FroDocument5 pagesFrochinmayghaisasNo ratings yet
- ClubfootDocument30 pagesClubfootdrusmanjamilhcmdNo ratings yet
- BFO-Biomechanics of The FootDocument5 pagesBFO-Biomechanics of The FootnovitaNo ratings yet
- Ankle Fractures: Winda Alviranisa/20204010293 Pembimbing: Dr. Muhammad Pandu Nugraha, SP - OTDocument28 pagesAnkle Fractures: Winda Alviranisa/20204010293 Pembimbing: Dr. Muhammad Pandu Nugraha, SP - OTwinda alviraNo ratings yet
- Pes Cavus and Hereditary Neuropathies When A Relationship Should Be SuspectedDocument5 pagesPes Cavus and Hereditary Neuropathies When A Relationship Should Be SuspectedSuhar Tomi100% (1)
- Pelvic SwayDocument2 pagesPelvic SwaywalterNo ratings yet
- Foot and Ankle BiomechanicsDocument25 pagesFoot and Ankle BiomechanicsSanh NguyễnNo ratings yet
- Exam 1 PathomehanicsDocument43 pagesExam 1 Pathomehanics8jm6dhjdcpNo ratings yet
- Ankle:: The Two Most Important Ankle Motions (Dorsiflexion and Plantarflexion) Are Assessed and TreatedDocument6 pagesAnkle:: The Two Most Important Ankle Motions (Dorsiflexion and Plantarflexion) Are Assessed and TreatedGuillaumeBanvilleNo ratings yet
- Fraktur Humerus EnglishDocument12 pagesFraktur Humerus EnglishAzizah Mutiara RosdianiNo ratings yet
- GALS Examination OSCE GuideDocument10 pagesGALS Examination OSCE GuideSandarekha PereraNo ratings yet
- Evidence Based Management of Plantar FasciitisDocument40 pagesEvidence Based Management of Plantar FasciitisMohamed ElMeligieNo ratings yet
- Ankle and FootDocument31 pagesAnkle and FootmetoNo ratings yet
- Special Test of The Lower ExtremitiesDocument7 pagesSpecial Test of The Lower ExtremitiesElijah QuianoNo ratings yet
- 2023 Cavus Foot SurgeryDocument83 pages2023 Cavus Foot SurgerysaragNo ratings yet
- Resident Ortho RotationDocument18 pagesResident Ortho RotationRuth PoeryNo ratings yet
- Orthotics and Prosthetics LectureDocument40 pagesOrthotics and Prosthetics LectureRock Obaidat100% (1)
- 01 Body Conformation of HorseDocument32 pages01 Body Conformation of HorseDrSagar Mahesh Sonwane100% (3)
- Pediatric Hallux ValgusDocument9 pagesPediatric Hallux ValgusJairo GuevaraNo ratings yet
- BFO - Review of Pathology KAFODocument6 pagesBFO - Review of Pathology KAFOnovitaNo ratings yet
- Knee&Foot Part2Document26 pagesKnee&Foot Part2SarkawtNo ratings yet
- The Failed Hallux ValgusDocument127 pagesThe Failed Hallux ValgusFlorin MacarieNo ratings yet
- Hip ExaminationDocument43 pagesHip ExaminationJayakrishnu tjNo ratings yet
- Foot and Ankle Injuries and Pain: Indranil Neel' Kushare, MDDocument55 pagesFoot and Ankle Injuries and Pain: Indranil Neel' Kushare, MDrizwan.mughal1997No ratings yet
- Ankle Foot OrthosisDocument4 pagesAnkle Foot Orthosis楊畯凱No ratings yet
- Case #5: Reagan Buie Parrish Amie Lehman HaraczDocument33 pagesCase #5: Reagan Buie Parrish Amie Lehman HaraczbaoNo ratings yet
- Biomechanics of Ankle and FootDocument40 pagesBiomechanics of Ankle and FootNujella BalajiNo ratings yet
- Proeve Van Bekwaamheid Van Standaard Orthopaedische Behandeling (Sob)Document9 pagesProeve Van Bekwaamheid Van Standaard Orthopaedische Behandeling (Sob)A.B.No ratings yet
- Ankle SprainDocument6 pagesAnkle Sprainshifali guptaNo ratings yet
- wk-10 pcp1 Study Guide Ques-AnsDocument8 pageswk-10 pcp1 Study Guide Ques-Ansapi-453771787No ratings yet
- 4 - Ankle and FootDocument65 pages4 - Ankle and Footxj74fr4ddxNo ratings yet
- Richard Ogden, DO, FACOFP, FAAFP Kansas Association of Osteopathic MedicineDocument38 pagesRichard Ogden, DO, FACOFP, FAAFP Kansas Association of Osteopathic MedicineMjidKarimNo ratings yet
- Improving Ankle and Knee Joint Stability: Proprioceptive Balancefit Discs DrillsFrom EverandImproving Ankle and Knee Joint Stability: Proprioceptive Balancefit Discs DrillsNo ratings yet
- Hallux Valgus (Bunion), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHallux Valgus (Bunion), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Morton's NeuromaDocument11 pagesMorton's NeuromaLikhit NayakNo ratings yet
- Medscimonit 25 7746Document9 pagesMedscimonit 25 7746sina dabiriNo ratings yet
- FootDocument59 pagesFootAnmar Hamid Abd AlmageedNo ratings yet
- Military Fitness and Injury RisksDocument21 pagesMilitary Fitness and Injury RiskskzxvmznxcnzZNo ratings yet
- Anatomical TermsDocument1 pageAnatomical TermsPhybe leeeNo ratings yet
- Toe DisarticulationDocument4 pagesToe Disarticulationadel santosNo ratings yet
- Catalogo COMFORSIL SiliconasDocument51 pagesCatalogo COMFORSIL SiliconasTalquipen DbzapNo ratings yet
- Laser Therapy ProtocolsDocument89 pagesLaser Therapy ProtocolsSYED ALI HUSSAINNo ratings yet
- Diabetic Foot Ulcer Prevention: An Evidence Based PracticeDocument6 pagesDiabetic Foot Ulcer Prevention: An Evidence Based PracticeHarismaPratamaNo ratings yet
- OpstDocument5 pagesOpstNEIL NETTE S. REYNALDONo ratings yet
- Barefoot Transition GuideDocument2 pagesBarefoot Transition GuideNath TVNo ratings yet
- Types of Beak and FeetDocument7 pagesTypes of Beak and FeetSheetal SahuNo ratings yet
- Callosities, Corns, and Calluses: BMJ Clinical Research July 1996Document5 pagesCallosities, Corns, and Calluses: BMJ Clinical Research July 1996dewiswahyu100% (1)
- Forefoot Study GuideDocument22 pagesForefoot Study GuideArchibald J. Loch83% (6)
- Musculoskeletal Examination Under GraduatesDocument98 pagesMusculoskeletal Examination Under GraduatesEsraa SalemNo ratings yet
- Skill Labs, Clinical History Taking, and ExaminationDocument84 pagesSkill Labs, Clinical History Taking, and ExaminationJoo Se HyukNo ratings yet
- By: Christya Lorena G Tutor: Dr. Dewi / Dr. Evan Supervisor: Dr. Jainal Arifin, SP - OTDocument9 pagesBy: Christya Lorena G Tutor: Dr. Dewi / Dr. Evan Supervisor: Dr. Jainal Arifin, SP - OTkacaacdhgjhlkNo ratings yet
- Top of The Foot Pain and Swelling TreatmentDocument13 pagesTop of The Foot Pain and Swelling TreatmentNyanLinKyawNo ratings yet
- Patient AssessmentDocument5 pagesPatient AssessmentMary Janine Joy RimanoNo ratings yet
- QX 56Document76 pagesQX 56Carolina OspinaNo ratings yet
- Uriel Foot Care ProductsDocument16 pagesUriel Foot Care ProductsIsrael ExporterNo ratings yet
- DGMS Circulars 1935-2016 PDFDocument1,095 pagesDGMS Circulars 1935-2016 PDFtridev kant tripathi100% (2)
- Ya2017.the Effect of Foot Type On The Foot Morphology and Plantar Pressure Distributions of Obese ChildrenDocument8 pagesYa2017.the Effect of Foot Type On The Foot Morphology and Plantar Pressure Distributions of Obese Childrentania martinezNo ratings yet
- Lower Extremity Amputation PreventionDocument1 pageLower Extremity Amputation PreventionEvaNo ratings yet
- Leprosy Case ProformaDocument4 pagesLeprosy Case Proforma127 Shruthik Patel Thota100% (1)
- Criminalistic SDocument137 pagesCriminalistic SSheila Mae CaballaNo ratings yet
- How To Evaluate A Case of LeprosyDocument35 pagesHow To Evaluate A Case of LeprosyBarath Kumar SinghNo ratings yet
- Price List EuroDocument6 pagesPrice List Euromnegrilam2002No ratings yet