Download as docx, pdf, or txt
You might also like
- Evening PrimroseDocument1 pageEvening PrimroseMeranie Tiglao AlfonsoNo ratings yet
- Phenylketonuria (PKU) : PH Arn, Nemours Children's Clinic, Jacksonville, FL, USADocument3 pagesPhenylketonuria (PKU) : PH Arn, Nemours Children's Clinic, Jacksonville, FL, USAHappy612No ratings yet
- Munyame 2018Document6 pagesMunyame 2018kemoNo ratings yet
- PhenylketonuriaDocument17 pagesPhenylketonuriamovies villa hit hai broNo ratings yet
- Phenylketonuria: Symposium: Inborn Errors of MetabolismDocument5 pagesPhenylketonuria: Symposium: Inborn Errors of MetabolismIntan RizanaNo ratings yet
- Biochemistry - METABOLISM OF PROTEINDocument44 pagesBiochemistry - METABOLISM OF PROTEINrebeccaNo ratings yet
- PkuDocument6 pagesPkuAlbertEscanoNo ratings yet
- Resin UptakeDocument4 pagesResin UptakeCome BackNo ratings yet
- Inborn Errors of MetabolismDocument40 pagesInborn Errors of MetabolismajjaNo ratings yet
- PhenylketonuriaDocument7 pagesPhenylketonuriaAnny AlvrzNo ratings yet
- PhenylketonuriaDocument7 pagesPhenylketonuriaReham QueNo ratings yet
- Phenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeDocument24 pagesPhenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeAsfoor gake1No ratings yet
- Phenylketonuria (PKU) : (Metabolic Condition: Amino Acid Disorder)Document1 pagePhenylketonuria (PKU) : (Metabolic Condition: Amino Acid Disorder)reriti2008No ratings yet
- NTN EssayDocument13 pagesNTN Essaymohammed alrubaiaanNo ratings yet
- Biochemical IndividualityDocument3 pagesBiochemical IndividualityPhysis.HolisticNo ratings yet
- Phenylketonuria: An Inborn Error of Phenylalanine MetabolismDocument11 pagesPhenylketonuria: An Inborn Error of Phenylalanine MetabolismAndreea StefanNo ratings yet
- DR Kumar Ponnusamy Biochemistry-Genetics USMLE Preparatory Course BIOGEN Reusable On-Line Resources For Large Group Teaching-Learning in Relatively Short TimeDocument1 pageDR Kumar Ponnusamy Biochemistry-Genetics USMLE Preparatory Course BIOGEN Reusable On-Line Resources For Large Group Teaching-Learning in Relatively Short TimeDr Kumar Ponnusamy100% (1)
- What Is PKU?: That Humans Obtain From Their Diet and Cannot Produce On Their Own.)Document2 pagesWhat Is PKU?: That Humans Obtain From Their Diet and Cannot Produce On Their Own.)SelliEfridaSiahaanNo ratings yet
- Group 4 - Pku (BSN 1-A)Document11 pagesGroup 4 - Pku (BSN 1-A)oluanah13No ratings yet
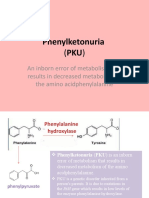
- Phenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino AcidphenylalanineDocument8 pagesPhenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino Acidphenylalanineელენე ბუჩუკურიNo ratings yet
- MCH Group 8Document12 pagesMCH Group 8nafisatmuhammed452No ratings yet
- PKU-giovannini 2007 JimdDocument9 pagesPKU-giovannini 2007 JimdajjaNo ratings yet
- Pku Consens SUA 2000Document17 pagesPku Consens SUA 2000beloshita_88No ratings yet
- PhenylketonuriaDocument8 pagesPhenylketonuriaAmberlee PetiNo ratings yet
- NCMA219Document11 pagesNCMA219Angelina Mei BenitezNo ratings yet
- PHENYLKETONURIADocument22 pagesPHENYLKETONURIAIvy Ann AguirreNo ratings yet
- Common IEM Solaf M Elsayed 2021Document13 pagesCommon IEM Solaf M Elsayed 2021anas barakahNo ratings yet
- FenilcetonuriaDocument6 pagesFenilcetonuriaM.C. Verónica Yazmin Mejía GarcíaNo ratings yet
- DR Kumar Ponnusamy Biochemistry Genetics USMLE Preparatory Course BIOGEN Reusable On Line Resources For Large Group Teaching Learning in Relatively SHDocument2 pagesDR Kumar Ponnusamy Biochemistry Genetics USMLE Preparatory Course BIOGEN Reusable On Line Resources For Large Group Teaching Learning in Relatively SHPonnusamy KumarNo ratings yet
- Nufd 255 Midterm Paper - No ReferencesDocument7 pagesNufd 255 Midterm Paper - No Referencesapi-305349012No ratings yet
- Inborn Error of Metabolism and Introduction To Cancer GeneticsDocument9 pagesInborn Error of Metabolism and Introduction To Cancer GeneticsviancaNo ratings yet
- The Complete European Guidelines On Phenylketonuria Diagnosis and TreatmentDocument56 pagesThe Complete European Guidelines On Phenylketonuria Diagnosis and TreatmentI'Jaz Farritz MuhammadNo ratings yet
- Impaired Neurotransmission in Early-Treated Phenylketonuria PatientsDocument9 pagesImpaired Neurotransmission in Early-Treated Phenylketonuria PatientsAndreea StefanNo ratings yet
- Case 9: Phenylketonuria: Group 1C: Obligado, Ervin Panibon, Lindsy Que, Reham Remitar, Jaira Dizza Salang, Marie NicholeDocument12 pagesCase 9: Phenylketonuria: Group 1C: Obligado, Ervin Panibon, Lindsy Que, Reham Remitar, Jaira Dizza Salang, Marie NicholeReham QueNo ratings yet
- PhenylketonuriaDocument14 pagesPhenylketonuriaMonica MoralesNo ratings yet
- Case3 PhenylketunuriaDocument2 pagesCase3 PhenylketunuriaKath BoniolNo ratings yet
- Inborn Errors of Metabolism: Albinism, Cystinuria, Pentosuria And, of Course, AlkaptonuriaDocument19 pagesInborn Errors of Metabolism: Albinism, Cystinuria, Pentosuria And, of Course, AlkaptonuriaSubhi MishraNo ratings yet
- PHENYLKETONURIADocument3 pagesPHENYLKETONURIAMiwa IshiiNo ratings yet
- Phenyl Keto NuriaDocument3 pagesPhenyl Keto NuriawawawawaNo ratings yet
- American Academy of Pediatrics Metabolic Disorders 2014 Practice TestDocument43 pagesAmerican Academy of Pediatrics Metabolic Disorders 2014 Practice TestPrabu KumarNo ratings yet
- Inborn Errors of Amino Acid Metabolism: (Advanced Nutrition)Document8 pagesInborn Errors of Amino Acid Metabolism: (Advanced Nutrition)Deepshikha PatelNo ratings yet
- Biochemical Basis of Phenylketonuria and Maple Syrup SyndromeDocument5 pagesBiochemical Basis of Phenylketonuria and Maple Syrup SyndromeLauraTomicNo ratings yet
- Phenylketonuria ReviewDocument3 pagesPhenylketonuria Reviewapi-334247133No ratings yet
- Genetics of Metabolic Disorders IDocument17 pagesGenetics of Metabolic Disorders IGagan DhaliwalNo ratings yet
- PHENYLKETONURIADocument4 pagesPHENYLKETONURIAmarsiel03No ratings yet
- Phenylketonuria: A Hallmark Disease For SocietyDocument8 pagesPhenylketonuria: A Hallmark Disease For SocietyMonyet...No ratings yet
- Pku GRP 1Document19 pagesPku GRP 1Jersey MariNo ratings yet
- Phenyl Keto NuriaDocument1 pagePhenyl Keto NuriamucwcburdwanNo ratings yet
- Pku - 2Document14 pagesPku - 2dwi adiNo ratings yet
- Inborn Errors of MetabolismDocument60 pagesInborn Errors of MetabolismPyneandy KimberlyNo ratings yet
- AAV-Mediated CRISPR/Cas9 Gene Editing in Murine PhenylketonuriaDocument12 pagesAAV-Mediated CRISPR/Cas9 Gene Editing in Murine PhenylketonuriaSpaceCadetNo ratings yet
- Response of Phenylketonuria To TetrahydrobiopterinDocument4 pagesResponse of Phenylketonuria To Tetrahydrobiopterinbeloshita_88No ratings yet
- Wikipedia: 3.1.-Una Patologia On Està Implicada. Modificació Estructural I Funcional (100 Paraules) (Jose)Document4 pagesWikipedia: 3.1.-Una Patologia On Està Implicada. Modificació Estructural I Funcional (100 Paraules) (Jose)jcasanovas1995No ratings yet
- Update of Newborn Screening and Therapy For Congenital HypothyroidismDocument14 pagesUpdate of Newborn Screening and Therapy For Congenital HypothyroidismMauricio HurtadoNo ratings yet
- Intoxicación Por AcetaminofenDocument4 pagesIntoxicación Por AcetaminofenGibsyVillacisMarriottNo ratings yet
- PSYE504a: Figure 1. Proofreading ProcessDocument7 pagesPSYE504a: Figure 1. Proofreading ProcessBianca Isabelle LariosaNo ratings yet
- Guidelines of AsDocument9 pagesGuidelines of AsLIZA2627428BNo ratings yet
- Articulo Final Verdadero!!!!Document6 pagesArticulo Final Verdadero!!!!lapzsssNo ratings yet
- PhenylketonuriaDocument1 pagePhenylketonuriaHolly SevillanoNo ratings yet
- A Simple Guide to Pseudohypoparathyroidism, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Pseudohypoparathyroidism, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Title 1 The Weight Loss Beast-Keto VibeDocument4 pagesTitle 1 The Weight Loss Beast-Keto VibeAgostina MiniNo ratings yet
- MS ObgyDocument18 pagesMS ObgySushantaNo ratings yet
- NCM 118 - Lesson 13 (DKA and HHNS)Document3 pagesNCM 118 - Lesson 13 (DKA and HHNS)Bobby Christian DuronNo ratings yet
- Pcol Cover To CoverDocument214 pagesPcol Cover To CoverJec OcampoNo ratings yet
- Tackling Obesity in The Western WorldDocument8 pagesTackling Obesity in The Western Worlditachi pandeyNo ratings yet
- JURNAL - Aspart InsulinDocument8 pagesJURNAL - Aspart InsulinTazkiyatan IsriaNo ratings yet
- Bioassay 5th SemDocument66 pagesBioassay 5th Semraj royel100% (10)
- Jaundice: Checklist For HistoryDocument17 pagesJaundice: Checklist For HistoryMustafa H. KadhimNo ratings yet
- A Successful Case Study On Ayurvedic Management of HypothyroidismDocument6 pagesA Successful Case Study On Ayurvedic Management of HypothyroidismIJRASETPublicationsNo ratings yet
- Medical Surgical Nursing Module 9Document8 pagesMedical Surgical Nursing Module 9weissNo ratings yet
- Burs Lem 2021Document13 pagesBurs Lem 2021ERINSONNo ratings yet
- Atlanta ClassificationDocument20 pagesAtlanta ClassificationAkreditasi Prodi BedahNo ratings yet
- Bio Ninth Mcqs by Naveed ButtDocument22 pagesBio Ninth Mcqs by Naveed ButtNaveed Ahmed ButtNo ratings yet
- HLTAAP001 Recognise Healthy Body System SAB v3.3 - TheORYDocument38 pagesHLTAAP001 Recognise Healthy Body System SAB v3.3 - TheORYboldguy222No ratings yet
- ENERGY SYSTEMS - Analyse The 3 Different Energy Systems - 1.2Document9 pagesENERGY SYSTEMS - Analyse The 3 Different Energy Systems - 1.2Ben Jenkins100% (4)
- Healthy Properties of Green and White Teas An Update Author S Pastoriza, M Mesias, C CabreraDocument20 pagesHealthy Properties of Green and White Teas An Update Author S Pastoriza, M Mesias, C CabreraTrázerNándorNo ratings yet
- CHAPTER 14 The Digestive SystemDocument116 pagesCHAPTER 14 The Digestive Systemteu doongieNo ratings yet
- Bspha C1 Las 1Document41 pagesBspha C1 Las 1Muhammad Haroon RazaNo ratings yet
- Polycystic Ovarian Syndrome (PCOS)Document119 pagesPolycystic Ovarian Syndrome (PCOS)Jasani JayrajNo ratings yet
- Congenital Hypothyroidism: Screening, Diagnosis, Management, and OutcomeDocument7 pagesCongenital Hypothyroidism: Screening, Diagnosis, Management, and OutcomeIbrahim Abdul KareemNo ratings yet
- CH19 2 Biology WsDocument5 pagesCH19 2 Biology Ws陳詩淇No ratings yet
- Primolut N NorethisteroneDocument2 pagesPrimolut N NorethisteroneSarathyTDNo ratings yet
- 8.1 (2.5 HL)Document21 pages8.1 (2.5 HL)SudeNo ratings yet
- Gce As/A Level: Friday, 20 May 2022 - Afternoon Basic Biochemistry and Cell OrganisationDocument32 pagesGce As/A Level: Friday, 20 May 2022 - Afternoon Basic Biochemistry and Cell OrganisationJ JNo ratings yet
- Year 7 Human Biology. All Yellow Answers Lesson 1Document3 pagesYear 7 Human Biology. All Yellow Answers Lesson 1Vinston ÅsénNo ratings yet
- Beta Adrenergic Blockers: SympatholyticDocument12 pagesBeta Adrenergic Blockers: SympatholyticAbdullah asadNo ratings yet
- Ak 17121723Document1 pageAk 17121723raghavremNo ratings yet
- Endocrine System NCM116 Midterm - XCDocument4 pagesEndocrine System NCM116 Midterm - XCXia CabilloNo ratings yet
- Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in Adults Clinical Features, Evaluation, and DiagnosisDocument17 pagesDiabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in Adults Clinical Features, Evaluation, and DiagnosisAhraxazel Galicia ReynaNo ratings yet