Download as pdf or txt
You might also like
- Accp 2021 P 1Document584 pagesAccp 2021 P 1Sarra HassanNo ratings yet
- Sanaa PDFDocument68 pagesSanaa PDFLjiljana Pucelj50% (4)
- Halil İnalcık - The Ottoman Economic Mind and Aspects of The Ottoman Economy PDFDocument10 pagesHalil İnalcık - The Ottoman Economic Mind and Aspects of The Ottoman Economy PDFA Seven HasdemirNo ratings yet
- 1 s2.0 S2666679022000040 MainDocument14 pages1 s2.0 S2666679022000040 MainRahmayantiYuliaNo ratings yet
- Stis in SwazilandDocument12 pagesStis in SwazilandMuhammad FansyuriNo ratings yet
- Risk of Leukemia After DengueDocument7 pagesRisk of Leukemia After DengueJoão Marcos Germano SouzaNo ratings yet
- Fatema Alzahraa Samy Amin Molecular Markers PredictingDocument10 pagesFatema Alzahraa Samy Amin Molecular Markers PredictingtomniucNo ratings yet
- Review ArticleDocument12 pagesReview ArticleNoka YogaNo ratings yet
- Jurnal 3 KA inggDocument7 pagesJurnal 3 KA inggMardika Wulandari 20 XII IPS3No ratings yet
- Human Papillomavirus and Cervical Cancer: Journal of Obstetrics and GynaecologyDocument8 pagesHuman Papillomavirus and Cervical Cancer: Journal of Obstetrics and GynaecologyMS WORLDNo ratings yet
- 244 FullDocument23 pages244 FullNur Ghaliyah SandraNo ratings yet
- Sexuallytransmittedhuman Papillomavirus: Update in Epidemiology, Prevention, and ManagementDocument22 pagesSexuallytransmittedhuman Papillomavirus: Update in Epidemiology, Prevention, and Managementerikglu2796No ratings yet
- Chlamydia Trachomatis Infection in Female Partners of Circumcised and Uncircumcised Adult MenDocument10 pagesChlamydia Trachomatis Infection in Female Partners of Circumcised and Uncircumcised Adult MenJuan Andre' MarquinezNo ratings yet
- Human Papillomavirus in The HIV-Infected Host - EpidemiologyDocument10 pagesHuman Papillomavirus in The HIV-Infected Host - EpidemiologyRenan RodriguesNo ratings yet
- Global Burden of CancersDocument8 pagesGlobal Burden of CancersMartinaNo ratings yet
- 1 s2.0 S2050052119301015 MainDocument10 pages1 s2.0 S2050052119301015 MainELSA DÍAZ LÓPEZNo ratings yet
- Assessment of Knowledge, Awareness About Cervical Cancer, Human PapillomavirusDocument4 pagesAssessment of Knowledge, Awareness About Cervical Cancer, Human PapillomavirusA HNo ratings yet
- Genotypes and Associated Risk Levels of Human Papilloma Virus Among Female Patients Attending Rabuor Sub County Hospital, KisumuDocument13 pagesGenotypes and Associated Risk Levels of Human Papilloma Virus Among Female Patients Attending Rabuor Sub County Hospital, KisumuMJBAS JournalNo ratings yet
- HHS Public Access: HIV-associated Malignancies in ChildrenDocument13 pagesHHS Public Access: HIV-associated Malignancies in Childrenmiss betawiNo ratings yet
- 4 5915746627611529826Document4 pages4 5915746627611529826A HNo ratings yet
- Papillomavirus Research: SciencedirectDocument17 pagesPapillomavirus Research: SciencedirectIvanes IgorNo ratings yet
- The Risk Factors For Cervical Cytological Abnormalities Among Women Infected With Non-16/18 High-Risk Human Papillomavirus: Cross-Sectional StudyDocument14 pagesThe Risk Factors For Cervical Cytological Abnormalities Among Women Infected With Non-16/18 High-Risk Human Papillomavirus: Cross-Sectional StudyAli HNo ratings yet
- Ali2019 Article BurdenAndGenotypeDistributionO PDFDocument9 pagesAli2019 Article BurdenAndGenotypeDistributionO PDFDhimas MuhammadNo ratings yet
- WA0054mmmDocument4 pagesWA0054mmmA HNo ratings yet
- Clamidia TrachomatisDocument13 pagesClamidia TrachomatisAnisha PutryNo ratings yet
- Pap IntroductionDocument390 pagesPap IntroductionAnish VeettiyankalNo ratings yet
- Prevalence and Incidence of Genital Warts and Cervical Human Papillomavirus Infections in Nigerian WomenDocument10 pagesPrevalence and Incidence of Genital Warts and Cervical Human Papillomavirus Infections in Nigerian WomenRiszki_03No ratings yet
- Prostate Cancer and Human Papillomavirus InfectionDocument9 pagesProstate Cancer and Human Papillomavirus InfectionRosana Ramirez SerranoNo ratings yet
- Historia Natural Del HPVDocument5 pagesHistoria Natural Del HPVpatologiacervicalupcNo ratings yet
- Prevention of Inection Related Tumor Bgr054Document9 pagesPrevention of Inection Related Tumor Bgr054heruNo ratings yet
- J Ijid 2014 07 029Document6 pagesJ Ijid 2014 07 029Mostafa SalahNo ratings yet
- VPH NegativoDocument20 pagesVPH NegativomilequeveditoNo ratings yet
- Human Papillomavirus Disease: EpidemiologyDocument30 pagesHuman Papillomavirus Disease: EpidemiologyGabriela LemNo ratings yet
- 244 Full PDFDocument23 pages244 Full PDFNur Ghaliyah SandraNo ratings yet
- PRD 12015Document13 pagesPRD 12015aletonatiuNo ratings yet
- Improvement of Therapy in Cervical CancerDocument1 pageImprovement of Therapy in Cervical CancerFree Escort ServiceNo ratings yet
- Cervical Cancer - An Overview of Pathophysiology and ManagementDocument9 pagesCervical Cancer - An Overview of Pathophysiology and ManagementIndah 15No ratings yet
- Human PapilomaDocument6 pagesHuman PapilomaatharNo ratings yet
- Human Papilloma Virus Vaccine For Cervical Cancer PreventionDocument9 pagesHuman Papilloma Virus Vaccine For Cervical Cancer Preventionsayeef khanNo ratings yet
- Fruits and Vegetables and Cervical Cancer: A Systematic Review and Meta-AnalysisDocument14 pagesFruits and Vegetables and Cervical Cancer: A Systematic Review and Meta-AnalysisSf AkhadiyatiNo ratings yet
- HPV: Infection, Prevention and Vaccination in India: Ritesh KumarDocument6 pagesHPV: Infection, Prevention and Vaccination in India: Ritesh Kumarsandeep raiNo ratings yet
- Article: Hepatitis B Infection in The Rural Area of Dschang, Cameroon: Seroprevalence and Associated FactorsDocument9 pagesArticle: Hepatitis B Infection in The Rural Area of Dschang, Cameroon: Seroprevalence and Associated FactorsSonyNo ratings yet
- RH Fs Risk FactorsDocument2 pagesRH Fs Risk FactorsfentroispNo ratings yet
- 1 s2.0 S0304383519306044 MainDocument15 pages1 s2.0 S0304383519306044 MainZulma madeline libny Gutarra ticaNo ratings yet
- Jurnal Condyloma AcuminataDocument11 pagesJurnal Condyloma Acuminataperussi pranadiptaNo ratings yet
- Worldwide Burden of Cancer Attributable To HPV by Site, Country and HPV TypeDocument7 pagesWorldwide Burden of Cancer Attributable To HPV by Site, Country and HPV Typeaselecz345No ratings yet
- Cancer de PeneDocument12 pagesCancer de PeneAndelcass DellNo ratings yet
- Role of Viruses in The Development of Breast CancerDocument6 pagesRole of Viruses in The Development of Breast CancerАйгуль ШарипNo ratings yet
- Frequency of HR-HPV Types in Patients With High Grade Cervical Intraepithelial Neoplasia (CIN)Document6 pagesFrequency of HR-HPV Types in Patients With High Grade Cervical Intraepithelial Neoplasia (CIN)ghaffari.eli5912No ratings yet
- Nejmcp 2108502Document9 pagesNejmcp 2108502Manuel GilNo ratings yet
- Cancer CervicalDocument16 pagesCancer CervicalSilvia Cerda RodríguezNo ratings yet
- 2011 ArticleDocument14 pages2011 Articleyongky sugandaNo ratings yet
- Project Title High Risk HPV Genotyping in Patient With Clinically Suspected Precancerous and Cancerous Lesions of CervixDocument16 pagesProject Title High Risk HPV Genotyping in Patient With Clinically Suspected Precancerous and Cancerous Lesions of CervixEmam MursalinNo ratings yet
- Cervical CA Proposal Jan152010Document21 pagesCervical CA Proposal Jan152010redblade_88100% (2)
- Gynaecologic and Breast Cancers in Women Living With HIVin South Africa: A Record Linkage StudyDocument13 pagesGynaecologic and Breast Cancers in Women Living With HIVin South Africa: A Record Linkage StudyDaniel TurudicNo ratings yet
- Human Papilloma VirusDocument9 pagesHuman Papilloma Virusema 274No ratings yet
- El Riesgo Relativo de Neoplasias (Pre) Malignas Relacionadas Con El Virus Del Papiloma Humano de Alto Riesgo No Cervical Después de Una Neoplasia Intraepitelial Cervical Recidivante de Grado 3 Un Estudio PoblacionalDocument4 pagesEl Riesgo Relativo de Neoplasias (Pre) Malignas Relacionadas Con El Virus Del Papiloma Humano de Alto Riesgo No Cervical Después de Una Neoplasia Intraepitelial Cervical Recidivante de Grado 3 Un Estudio PoblacionalLucero MedranoNo ratings yet
- 46-Article Text-138-2-10-20180220Document11 pages46-Article Text-138-2-10-20180220Anonymous nErkwtXnuSNo ratings yet
- Keywords: Human Papillomavirus Vaccine, Efficacy, Safety, Phase III Randomized TrialsDocument10 pagesKeywords: Human Papillomavirus Vaccine, Efficacy, Safety, Phase III Randomized TrialsBassment MixshowNo ratings yet
- Jurnal CZ CX 4Document10 pagesJurnal CZ CX 4Netty FransiskaNo ratings yet
- 23 - Cancer Risk in Patients With Candidiasis - A NationwideDocument12 pages23 - Cancer Risk in Patients With Candidiasis - A NationwideRenan RodriguesNo ratings yet
- Cervical Cancer Research 1Document9 pagesCervical Cancer Research 1tivaNo ratings yet
- Molecular TechniquesDocument4 pagesMolecular TechniquesMulatuNo ratings yet
- Seroepidemiological TrachomatisDocument5 pagesSeroepidemiological TrachomatisMulatuNo ratings yet
- Biological Characterization of Chlamydia TrachomatisDocument9 pagesBiological Characterization of Chlamydia TrachomatisMulatuNo ratings yet
- Similarities and Differences of Nucleic Acids and ProtiensDocument13 pagesSimilarities and Differences of Nucleic Acids and ProtiensMulatuNo ratings yet
- Molecular Analysis of Antimicrobial Resistance Mechanisms in N-GonoDocument11 pagesMolecular Analysis of Antimicrobial Resistance Mechanisms in N-GonoMulatuNo ratings yet
- Installation Manual of The Solar Weather Monitoring StationDocument40 pagesInstallation Manual of The Solar Weather Monitoring Stationsamwel kariukiNo ratings yet
- DC SimpDocument3 pagesDC SimpNikhil HiremathNo ratings yet
- TubosDocument12 pagesTubosASHIK TNo ratings yet
- Gyane MCQS 6, 7, 9 Chapter Irfan Masood PDFDocument16 pagesGyane MCQS 6, 7, 9 Chapter Irfan Masood PDFJansher Ali Chohan100% (1)
- Leather Goods - Sialkot 2020Document12 pagesLeather Goods - Sialkot 2020Sanchita GuptaNo ratings yet
- MD (BD) - Lst-Cep-In-1001 Control System Io List Rev0 PDFDocument17 pagesMD (BD) - Lst-Cep-In-1001 Control System Io List Rev0 PDFKook PengNo ratings yet
- ChirdsDocument5 pagesChirdsWise FidelityNo ratings yet
- 01 Final Technical Specification For 63 100 KVA 110-4Document42 pages01 Final Technical Specification For 63 100 KVA 110-4Prasad RajendraNo ratings yet
- Q1.Starch and Cellulose Are Two Important Plant PolysaccharidesDocument15 pagesQ1.Starch and Cellulose Are Two Important Plant PolysaccharidesafshinNo ratings yet
- Tumor Necrosis Factor Methods and ProtocolsDocument265 pagesTumor Necrosis Factor Methods and ProtocolsDario GomezNo ratings yet
- Circulatory SystemDocument14 pagesCirculatory Systemsmbdy tbhhhNo ratings yet
- Corrosion Probe TypeDocument26 pagesCorrosion Probe TypeFirman MuttaqinNo ratings yet
- NetworkingDocument20 pagesNetworkingJaspreetSingh0% (1)
- 3-4. SST3005. Rocks and Minerals. KHMYDocument40 pages3-4. SST3005. Rocks and Minerals. KHMYFARAH HIDAYAHNo ratings yet
- Rencana Anggaran Biaya Coffee Shop 2022Document5 pagesRencana Anggaran Biaya Coffee Shop 2022Maulana MalikNo ratings yet
- Color Monitor: Service ManualDocument33 pagesColor Monitor: Service ManualtongshadowNo ratings yet
- An Analysis of Consumption in The Fast Fashion IndustryDocument9 pagesAn Analysis of Consumption in The Fast Fashion IndustryFulbright L.No ratings yet
- 6.5mm GrendelDocument3 pages6.5mm GrendelErich EshelmanNo ratings yet
- Quotation-LT Switchgear Panel & DCDB-Lubrizol Dahej ProjectDocument3 pagesQuotation-LT Switchgear Panel & DCDB-Lubrizol Dahej ProjectSharafat AliNo ratings yet
- Case Study Real Estate Sector: Shubham SainiDocument4 pagesCase Study Real Estate Sector: Shubham Sainishubham sainiNo ratings yet
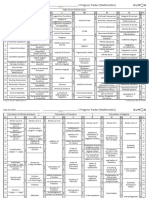
- Kumon Mathematics Progress Tracker Levels C To O PDFDocument2 pagesKumon Mathematics Progress Tracker Levels C To O PDFcharmradeekNo ratings yet
- MedianDocument7 pagesMedianBrian RogersNo ratings yet
- Color in FoodDocument4 pagesColor in FoodHaque Bhai0% (1)
- Summary Safety Data Sheet: 1. Substance NameDocument2 pagesSummary Safety Data Sheet: 1. Substance NameAchraf Ben DhifallahNo ratings yet
- Asme-B18.13.1m (1998)Document28 pagesAsme-B18.13.1m (1998)Sergio Rodriguez CamberosNo ratings yet
- SM 25Document144 pagesSM 25Jan Svein HammerNo ratings yet
- Embedded SystemDocument75 pagesEmbedded SystemDnyaneshwar KarhaleNo ratings yet