Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Module 5 - Emergency Preparedness - BOSH For SO1Document40 pagesModule 5 - Emergency Preparedness - BOSH For SO1NKH Mega GasNo ratings yet
- Script For Health Talk ShowDocument2 pagesScript For Health Talk ShowJana Jean Ogoc100% (6)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Autism For DummiesDocument11 pagesAutism For Dummiesgocyndigo72yahoocomNo ratings yet
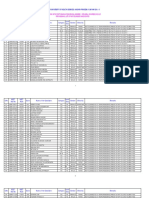
- PG CQ 2022-23 Not Eligible ListDocument3 pagesPG CQ 2022-23 Not Eligible Listsrikanth PosaNo ratings yet
- Herbal Antibiotics: A Review: October 2020Document8 pagesHerbal Antibiotics: A Review: October 2020srikanth PosaNo ratings yet
- Office of The District Medical and Health Officer: Jogulamba Gadwal DistrictDocument2 pagesOffice of The District Medical and Health Officer: Jogulamba Gadwal Districtsrikanth PosaNo ratings yet
- New Aiapget Scorecard AiapgetDocument2 pagesNew Aiapget Scorecard Aiapgetsrikanth PosaNo ratings yet
- Concept of Shad Garbhakara Bhavas in Ayurveda: A Review ArticleDocument2 pagesConcept of Shad Garbhakara Bhavas in Ayurveda: A Review Articlesrikanth PosaNo ratings yet
- All India Ayush Post Graduate Entrance Test - 2021 Admit Card - ProvisionalDocument4 pagesAll India Ayush Post Graduate Entrance Test - 2021 Admit Card - Provisionalsrikanth PosaNo ratings yet
- 1st Round DrntruhsDocument1 page1st Round Drntruhssrikanth PosaNo ratings yet
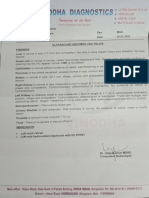
- Scan Report PDFDocument1 pageScan Report PDFsrikanth PosaNo ratings yet
- TS - UG - MBBS - 2021 - CQ - Not Reported - P1 - 08-03-2022Document11 pagesTS - UG - MBBS - 2021 - CQ - Not Reported - P1 - 08-03-2022srikanth PosaNo ratings yet
- Dr. NTR University of Health Sciences:: A.P .Vijayawada - 520 008Document9 pagesDr. NTR University of Health Sciences:: A.P .Vijayawada - 520 008srikanth PosaNo ratings yet
- Diet Chart For West IndiaDocument6 pagesDiet Chart For West Indiasrikanth PosaNo ratings yet
- Maharashtra State Cet Cell Not Eligible: DATED: 25/03/2021Document14 pagesMaharashtra State Cet Cell Not Eligible: DATED: 25/03/2021srikanth PosaNo ratings yet
- 5 6077968598943401080Document45 pages5 6077968598943401080srikanth PosaNo ratings yet
- Post Graduate Diploma in Emergency Medical TechnologyDocument13 pagesPost Graduate Diploma in Emergency Medical Technologysrikanth PosaNo ratings yet
- NT ENT: Ract EMDocument6 pagesNT ENT: Ract EMsrikanth PosaNo ratings yet
- Symbiosis Centre For Health Skills, Pune Post Graduate Diploma in Emergency Medical Services Programme Structure 2021-22Document4 pagesSymbiosis Centre For Health Skills, Pune Post Graduate Diploma in Emergency Medical Services Programme Structure 2021-22srikanth PosaNo ratings yet
- Government of Andhra Pradesh Medical and Health Department Prakasam DistrictDocument7 pagesGovernment of Andhra Pradesh Medical and Health Department Prakasam Districtsrikanth PosaNo ratings yet
- Stress Among Charge NursesDocument10 pagesStress Among Charge NursesRey AllanNo ratings yet
- "Take Off Patient/ Operan Jaga": Tugas Bahasa InggrisDocument3 pages"Take Off Patient/ Operan Jaga": Tugas Bahasa InggrisKurnia anggrainiNo ratings yet
- Artigo Depressão Na TCCDocument21 pagesArtigo Depressão Na TCCLarissa BenderNo ratings yet
- Family Case Study SampleDocument36 pagesFamily Case Study SampleArjay EllaNo ratings yet
- DOH Annual CalendarDocument1 pageDOH Annual CalendarBoni G. PajeNo ratings yet
- Gonorrhea SlidesDocument54 pagesGonorrhea SlidesYonathanHasudunganNo ratings yet
- CastrationDocument22 pagesCastrationಮನೋಜ್ ಭಾರದ್ವಾಜ್No ratings yet
- A Study of Single Parents - Their Stress and Social SupportDocument217 pagesA Study of Single Parents - Their Stress and Social SupportAde AdriiNo ratings yet
- 3.mellennium Development Goals (MDG)Document30 pages3.mellennium Development Goals (MDG)Brave TulaganNo ratings yet
- Managing Encopresis in The Pediatric Setting: The DSM-5 Autism Criteria: A Social Rather - .Document5 pagesManaging Encopresis in The Pediatric Setting: The DSM-5 Autism Criteria: A Social Rather - .Yurizna Almira Nst IINo ratings yet
- Sample BrochureDocument2 pagesSample BrochurealyssamciceroNo ratings yet
- Diabetic NeuropathyDocument4 pagesDiabetic NeuropathyAsish GeiorgeNo ratings yet
- Analysis Aiapget 2018Document4 pagesAnalysis Aiapget 2018arpit sachanNo ratings yet
- TractionDocument11 pagesTractionDenalyn Ann TormoNo ratings yet
- Mapeh 8health q3 Summative TestDocument3 pagesMapeh 8health q3 Summative TestJanmae ImperialNo ratings yet
- TRIAGEDocument55 pagesTRIAGELaveena AswaleNo ratings yet
- Job Stress Work Performance With CommentssssDocument37 pagesJob Stress Work Performance With CommentssssAmen MartzNo ratings yet
- Foundations For Assisting in Home Care 1520419723Document349 pagesFoundations For Assisting in Home Care 1520419723amasrurNo ratings yet
- Analytical Exposition Text: By: Ariful SukronDocument8 pagesAnalytical Exposition Text: By: Ariful SukronAriful SukronNo ratings yet
- 2019 Developmentofthe PMGQand Prevalenceof Mobile Gaming Addiction Among Adolescentsin Taiwan Cyberpsychol Behav Soc NetwDocument8 pages2019 Developmentofthe PMGQand Prevalenceof Mobile Gaming Addiction Among Adolescentsin Taiwan Cyberpsychol Behav Soc NetwJr BagaporoNo ratings yet
- CASR Part 67 Ed. 1 Amdt 0 - Medical Standard and CertificationDocument43 pagesCASR Part 67 Ed. 1 Amdt 0 - Medical Standard and CertificationR SetiawanNo ratings yet
- AQI Bulletin 20221017Document14 pagesAQI Bulletin 20221017Amrish TrivediNo ratings yet
- Medtech Laws and Bioethics MTE 114Document3 pagesMedtech Laws and Bioethics MTE 114Lowin NavarroNo ratings yet
- 7 Fundamentals of Ayurved&SwasthavrittaDocument8 pages7 Fundamentals of Ayurved&SwasthavrittaAnonymous 2gu2TzNo ratings yet
- Cerebro Lys inDocument18 pagesCerebro Lys inKathleen PalomariaNo ratings yet
- Program Pelayanan Lingkungan USAIDDocument313 pagesProgram Pelayanan Lingkungan USAIDioels100% (1)
- Kerala Floods - 2018: A Report by Archbishop Andrews ThazhathDocument31 pagesKerala Floods - 2018: A Report by Archbishop Andrews Thazhathsunil unnithanNo ratings yet