
Gorucu Coskuner2017
Gorucu Coskuner2017
You might also like
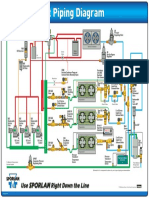
- HVACR Supermarket Piping DiagramDocument1 pageHVACR Supermarket Piping DiagramAngel sandovalNo ratings yet
- Short-And Long-Term Evaluation of Mandibular Dental Arch Dimensional Changes in Patients Treated With A Lip Bumper During Mixed Dentition Followed by Fixed AppliancesDocument8 pagesShort-And Long-Term Evaluation of Mandibular Dental Arch Dimensional Changes in Patients Treated With A Lip Bumper During Mixed Dentition Followed by Fixed AppliancesGABRIELA NIETO GONZALEZNo ratings yet
- Long-Term Effects of Rapid Maxillary Expansion Followed by Fixed AppliancesDocument5 pagesLong-Term Effects of Rapid Maxillary Expansion Followed by Fixed AppliancesFourthMolar.comNo ratings yet
- Stability of Orthodontic Treatment Outcome in Relation To Retention Status: An 8-Year Follow-UpDocument7 pagesStability of Orthodontic Treatment Outcome in Relation To Retention Status: An 8-Year Follow-UpNeeraj AroraNo ratings yet
- Strability of Orhodontic Treatment Outcome in Relation To Retention Status A 8 Year Follow UpDocument7 pagesStrability of Orhodontic Treatment Outcome in Relation To Retention Status A 8 Year Follow UpBraulio CaroNo ratings yet
- Fixed Versus Removable Orthodontic Appliances To Correct Anterior Crossbite in The Mixed Dentition-A Randomized Controlled Trial PDFDocument6 pagesFixed Versus Removable Orthodontic Appliances To Correct Anterior Crossbite in The Mixed Dentition-A Randomized Controlled Trial PDFJejeNo ratings yet
- Deguchi, 2011Document9 pagesDeguchi, 2011Laiana LarussaNo ratings yet
- ART - EXP.MAND.7.Postretention Changes in Mandibular CrowdingDocument11 pagesART - EXP.MAND.7.Postretention Changes in Mandibular CrowdingDiana Paola FontechaNo ratings yet
- Original Research Article: Burhan Showkat, Jayesh S. Rahalkar, Sandeep Jethe, Ravindra ManerikarDocument5 pagesOriginal Research Article: Burhan Showkat, Jayesh S. Rahalkar, Sandeep Jethe, Ravindra ManerikarjaslinshalinNo ratings yet
- CJN 079Document199 pagesCJN 079SelvaArockiamNo ratings yet
- Cju 005Document5 pagesCju 005gifar ihsanNo ratings yet
- Stalpers Am JOrthod Dentofac Orthop 2007132316323Document8 pagesStalpers Am JOrthod Dentofac Orthop 2007132316323thomas QuilangNo ratings yet
- Mandibular Incisor Recrowding Is It Different in Extraction and Nonextraction Cases 2247 2452.1000649Document7 pagesMandibular Incisor Recrowding Is It Different in Extraction and Nonextraction Cases 2247 2452.1000649monicaordonezNo ratings yet
- Stability of Class II Malocclusion Treatment With The Distal Jet Followed by Fixed AppliancesDocument8 pagesStability of Class II Malocclusion Treatment With The Distal Jet Followed by Fixed AppliancesFabian BarretoNo ratings yet
- 10 1067@mpr 2000 107113Document7 pages10 1067@mpr 2000 107113gbaez.88No ratings yet
- Implant-Supported Removable Partial Dentures in The Mandible A 3-16 Year Retrospective StudyDocument8 pagesImplant-Supported Removable Partial Dentures in The Mandible A 3-16 Year Retrospective StudyMohammad Fadyl YunizarNo ratings yet
- Predictors of Postretention Stability of Mandibular Dental Arch Dimensions in Patients Treated With A Lip Bumper During Mixed Dentition Followed by Fixed AppliancesDocument6 pagesPredictors of Postretention Stability of Mandibular Dental Arch Dimensions in Patients Treated With A Lip Bumper During Mixed Dentition Followed by Fixed AppliancesGABRIELA NIETO GONZALEZNo ratings yet
- A Longitudinal Study of Incremental Expansion Using A Mandibular Lip BumperDocument5 pagesA Longitudinal Study of Incremental Expansion Using A Mandibular Lip Bumperapi-26468957No ratings yet
- Stability of Unilateral Posterior Crossbite Correction in The Mixed Dentition: A Randomized Clinical Trial With A 3-Year Follow-UpDocument9 pagesStability of Unilateral Posterior Crossbite Correction in The Mixed Dentition: A Randomized Clinical Trial With A 3-Year Follow-UpPae Anusorn AmtanonNo ratings yet
- Mandibular Incisor Alignment in Untreated Subjects Compared With Long-Term Changes After OrthodonticDocument9 pagesMandibular Incisor Alignment in Untreated Subjects Compared With Long-Term Changes After OrthodonticPAOLA IVETTE MARTINEZ RODRIGUEZNo ratings yet
- Cone-Beam Computed Tomography Evaluation of Periodontal and Bone Support Loss in Extraction CasesDocument8 pagesCone-Beam Computed Tomography Evaluation of Periodontal and Bone Support Loss in Extraction CasesAlla MushkeyNo ratings yet
- Anterior Tooth Alignment A Comparison of Orthodontic Retention Regimens 5 Years PosttreatmentDocument7 pagesAnterior Tooth Alignment A Comparison of Orthodontic Retention Regimens 5 Years PosttreatmentRenan VeigaNo ratings yet
- 8 - Clinical Outcome in Periradicular Surgery Effect of Patient - and Tooth-Related Factors - A Multicenter StudyDocument8 pages8 - Clinical Outcome in Periradicular Surgery Effect of Patient - and Tooth-Related Factors - A Multicenter StudykochikaghochiNo ratings yet
- Hendrix 1994 Artigo 7 BaseDocument5 pagesHendrix 1994 Artigo 7 BaseGISELLE DE BRITO HENRIQUENo ratings yet
- Long-Term Clinical Outcome of Rapid Maxillary Expansion As The Only Treatment Performed in Class I MalocclusionDocument5 pagesLong-Term Clinical Outcome of Rapid Maxillary Expansion As The Only Treatment Performed in Class I MalocclusionMariana SantosNo ratings yet
- Long-Term Stability After Orthodontic Treatment Remains InconclusiveDocument2 pagesLong-Term Stability After Orthodontic Treatment Remains InconclusiveHabeeb AL-AbsiNo ratings yet
- NEW BUSHRA FinalDocument22 pagesNEW BUSHRA Finalmudassir rehman100% (1)
- A One Year Pilot Prospective Multicenter StudyDocument10 pagesA One Year Pilot Prospective Multicenter StudyEly Valentina Contreras ArceoNo ratings yet
- Comparison of The Effects of Rapid Maxillary ExpanDocument10 pagesComparison of The Effects of Rapid Maxillary Expancarl marxNo ratings yet
- Maxillary Dentoalveolar Assessment Following Retraction of Maxillary Incisors: A Preliminary StudyDocument8 pagesMaxillary Dentoalveolar Assessment Following Retraction of Maxillary Incisors: A Preliminary StudyAndrea TokumotoNo ratings yet
- 10 1016@j Ajodo 2016 03 020 PDFDocument10 pages10 1016@j Ajodo 2016 03 020 PDFMonojit DuttaNo ratings yet
- J Odw 2016 11 006Document6 pagesJ Odw 2016 11 006Ahmed ElsharkawyNo ratings yet
- Art 2Document6 pagesArt 2Joyce Stefania Posada MauricioNo ratings yet
- Long-Term Stability of Anterior Open-Bite Treatment by Intrusion of Maxillary Posterior TeethDocument9 pagesLong-Term Stability of Anterior Open-Bite Treatment by Intrusion of Maxillary Posterior TeethNg Chun HownNo ratings yet
- Stability of Transverse Expansion in The Mandibular ArchDocument6 pagesStability of Transverse Expansion in The Mandibular ArchManena RivoltaNo ratings yet
- EARLY Intervention in The Transverse DimensionDocument3 pagesEARLY Intervention in The Transverse DimensionBoboc FlorinNo ratings yet
- Effect of Different Incisor Movements On The Soft Tissue Profile (2016)Document9 pagesEffect of Different Incisor Movements On The Soft Tissue Profile (2016)Nicolas ValenzuelaNo ratings yet
- Anterior Tooth Wear and Retention Type Until 5 Years After Orthodontic TreatmentDocument8 pagesAnterior Tooth Wear and Retention Type Until 5 Years After Orthodontic TreatmentRenan VeigaNo ratings yet
- Long-Term Effectiveness of Canine-To-Canine Bonded Exible Spiral Wire Lingual RetainersDocument8 pagesLong-Term Effectiveness of Canine-To-Canine Bonded Exible Spiral Wire Lingual RetainersVinit SinghNo ratings yet
- Artigo BomDocument6 pagesArtigo BomCiro GassibeNo ratings yet
- A Withinpatient Comparative Study of The Influence of Number and Distribution of Ball Attachment Retained Mandibular Overdenture 1011Document6 pagesA Withinpatient Comparative Study of The Influence of Number and Distribution of Ball Attachment Retained Mandibular Overdenture 1011dentureNo ratings yet
- Evaluation of Open Bite Closure Using Clear AligneDocument9 pagesEvaluation of Open Bite Closure Using Clear AligneManuel CastilloNo ratings yet
- Cephalometric Assessment of Dentofacial Vertical Changes in Class I Subjects Treated With and Without ExtractionDocument7 pagesCephalometric Assessment of Dentofacial Vertical Changes in Class I Subjects Treated With and Without ExtractionMohamed FaragNo ratings yet
- 3205 All On Four Concept in Implant Dentistry A Literature ReviewDocument7 pages3205 All On Four Concept in Implant Dentistry A Literature ReviewAngelaBaleaNo ratings yet
- Outcome of Single Immediate Implants Placed inDocument8 pagesOutcome of Single Immediate Implants Placed injuanita enriquezNo ratings yet
- Periapical Bone Healing After ApicectomyDocument5 pagesPeriapical Bone Healing After ApicectomyMarwa Wagih ElboraeyNo ratings yet
- Miroperforaciones PDFDocument6 pagesMiroperforaciones PDFceci hdeezNo ratings yet
- Fu 2016Document10 pagesFu 2016Soe San KyawNo ratings yet
- Bone Augmentation of The Edentulous Maxilla For Implant Placement: A Systematic ReviewDocument12 pagesBone Augmentation of The Edentulous Maxilla For Implant Placement: A Systematic ReviewJarvin Miguel Buitrago GalindezNo ratings yet
- Factors Influencing The Outcome of Root-Resection Therapy in Molars: A 10-Year Retrospective StudyDocument9 pagesFactors Influencing The Outcome of Root-Resection Therapy in Molars: A 10-Year Retrospective StudyAshok KpNo ratings yet
- Agliardi - Immediate Fixed Rehabilitation ofDocument11 pagesAgliardi - Immediate Fixed Rehabilitation ofAnsaquilo AnsaquiloNo ratings yet
- A. Alineadores - L. Levrini, A. CarganicoDocument5 pagesA. Alineadores - L. Levrini, A. CarganicoYayis LondoñoNo ratings yet
- Mandibular 2 Implant Ball Bar Overdenture 10 Yaers CUNE IJP 2010Document9 pagesMandibular 2 Implant Ball Bar Overdenture 10 Yaers CUNE IJP 2010Johnny CHNo ratings yet
- Cerny Fixed RetainerDocument88 pagesCerny Fixed Retainerchinchiayeh5699No ratings yet
- Skeletal Anchorage Augmentation in Extraction/Nonextraction Orthodontic Treatment: A Randomized Clinical StudyDocument13 pagesSkeletal Anchorage Augmentation in Extraction/Nonextraction Orthodontic Treatment: A Randomized Clinical Studyaleja.b7815No ratings yet
- 1 s2.0 S088954061001005X MainDocument6 pages1 s2.0 S088954061001005X MainPanaite TinelaNo ratings yet
- Therapeutic Changes in Extraction Versus Non-Extraction Orthodontic TreatmentDocument12 pagesTherapeutic Changes in Extraction Versus Non-Extraction Orthodontic Treatmentmohamed chaaboubNo ratings yet
- Magnetic BBDocument7 pagesMagnetic BBVicente ContrerasNo ratings yet
- What-are-the-Surgical-Movements-in-Orthognathic-Surgery-That-Most-Affect-the-Upper-Airways-A-Three-Dimensional-AnalysisDocument13 pagesWhat-are-the-Surgical-Movements-in-Orthognathic-Surgery-That-Most-Affect-the-Upper-Airways-A-Three-Dimensional-Analysisr1maxilo2021No ratings yet
- Does The Maxillary Midline Diastema Close After Frenectomy?: Oral SurgeryDocument10 pagesDoes The Maxillary Midline Diastema Close After Frenectomy?: Oral Surgeryantonio dlNo ratings yet
- Implant Therapy: Clinical Approaches and Evidence of Success, Second EditionFrom EverandImplant Therapy: Clinical Approaches and Evidence of Success, Second EditionNo ratings yet
- Rahman MD Matiur-2230130236-10noDocument4 pagesRahman MD Matiur-2230130236-10noadnanNo ratings yet
- Open Printable/Searchable Copy (PDF Format) : Global Mapper User's ManualDocument361 pagesOpen Printable/Searchable Copy (PDF Format) : Global Mapper User's ManualIrwan RusmanaNo ratings yet
- Activity 2: Mathematical Modeling of Physical SystemsDocument10 pagesActivity 2: Mathematical Modeling of Physical SystemsNico SilorioNo ratings yet
- The History and Evolution of QuaternionsDocument3 pagesThe History and Evolution of QuaternionsAnton Van WykNo ratings yet
- FURLEY, David J. (1981) - The Greek Theory of The Infinite UniverseDocument16 pagesFURLEY, David J. (1981) - The Greek Theory of The Infinite UniverseAri CostamagnaNo ratings yet
- Keepers Smart Contracts Audit v0.1 GingerSecDocument60 pagesKeepers Smart Contracts Audit v0.1 GingerSecAbhishek ShuklaNo ratings yet
- Quality Assurance of Pressure-Sensitive Tapes: Standard Practice ForDocument6 pagesQuality Assurance of Pressure-Sensitive Tapes: Standard Practice ForYoga PradanaNo ratings yet
- Jeep-Willys DmiDocument14 pagesJeep-Willys DmiGabriel Fodor100% (1)
- Matter-Nature and Behaviour (Conceptual Questions With Very Short Answers)Document4 pagesMatter-Nature and Behaviour (Conceptual Questions With Very Short Answers)Syed Mazhar AliNo ratings yet
- XLPE Polyethylene Lifetime Detection PDFDocument120 pagesXLPE Polyethylene Lifetime Detection PDFconqiuNo ratings yet
- Atmel ATmega328 Test Circuit DiagramDocument6 pagesAtmel ATmega328 Test Circuit Diagramcadeyare2No ratings yet
- Shoes Shop Online WebsiteDocument26 pagesShoes Shop Online WebsiteNguyễn HưngNo ratings yet
- Masonry TutorialDocument45 pagesMasonry TutorialGajendra Joshi100% (2)
- Steam Tables AsmeDocument32 pagesSteam Tables AsmeNatsNo ratings yet
- Freeman Et Al The Condor 2019Document11 pagesFreeman Et Al The Condor 2019Guilain TSETAGHONo ratings yet
- Unit 2Document3 pagesUnit 2lewlking123No ratings yet
- Scratch Tester 430Document4 pagesScratch Tester 430laboratorioNo ratings yet
- Design, Implementation and Verification of 32-Bit ALU With VIODocument6 pagesDesign, Implementation and Verification of 32-Bit ALU With VIONubia DiazNo ratings yet
- Nouradini PDFDocument15 pagesNouradini PDFDavi AhmadNo ratings yet
- Evc Drive User Manual en Us 160814Document142 pagesEvc Drive User Manual en Us 160814Coil98No ratings yet
- Useful Note For SEF Quiz No.1Document12 pagesUseful Note For SEF Quiz No.1ganamuNo ratings yet
- 01-Introduction To VSCDocument30 pages01-Introduction To VSCeng7senNo ratings yet
- Flexible Sprinkler ConnectionDocument5 pagesFlexible Sprinkler ConnectionOwais AhmedNo ratings yet
- Step by Step 1 PDFDocument164 pagesStep by Step 1 PDFMohamed Ali100% (1)
- B. TECH 2nd Semester June 2019-1 PDFDocument5 pagesB. TECH 2nd Semester June 2019-1 PDFHarshitNo ratings yet
- 7sd522 SiemensDocument17 pages7sd522 SiemensSanthosh Kumar VinayagamNo ratings yet
- The Fundamentals of End MillsDocument3 pagesThe Fundamentals of End MillsILikeScribd5050No ratings yet
- Sample Form Inspection ChecklistDocument5 pagesSample Form Inspection Checklistadolf001No ratings yet
- The Scalpel Finishing Technique: A Tooth-Friendly Way To Finish Dental Composites in Anterior TeethDocument18 pagesThe Scalpel Finishing Technique: A Tooth-Friendly Way To Finish Dental Composites in Anterior TeethSoraya BouchammaNo ratings yet























































































Download as pdf or txt
You might also like
- HVACR Supermarket Piping DiagramDocument1 pageHVACR Supermarket Piping DiagramAngel sandovalNo ratings yet
- Short-And Long-Term Evaluation of Mandibular Dental Arch Dimensional Changes in Patients Treated With A Lip Bumper During Mixed Dentition Followed by Fixed AppliancesDocument8 pagesShort-And Long-Term Evaluation of Mandibular Dental Arch Dimensional Changes in Patients Treated With A Lip Bumper During Mixed Dentition Followed by Fixed AppliancesGABRIELA NIETO GONZALEZNo ratings yet
- Long-Term Effects of Rapid Maxillary Expansion Followed by Fixed AppliancesDocument5 pagesLong-Term Effects of Rapid Maxillary Expansion Followed by Fixed AppliancesFourthMolar.comNo ratings yet
- Stability of Orthodontic Treatment Outcome in Relation To Retention Status: An 8-Year Follow-UpDocument7 pagesStability of Orthodontic Treatment Outcome in Relation To Retention Status: An 8-Year Follow-UpNeeraj AroraNo ratings yet
- Strability of Orhodontic Treatment Outcome in Relation To Retention Status A 8 Year Follow UpDocument7 pagesStrability of Orhodontic Treatment Outcome in Relation To Retention Status A 8 Year Follow UpBraulio CaroNo ratings yet
- Fixed Versus Removable Orthodontic Appliances To Correct Anterior Crossbite in The Mixed Dentition-A Randomized Controlled Trial PDFDocument6 pagesFixed Versus Removable Orthodontic Appliances To Correct Anterior Crossbite in The Mixed Dentition-A Randomized Controlled Trial PDFJejeNo ratings yet
- Deguchi, 2011Document9 pagesDeguchi, 2011Laiana LarussaNo ratings yet
- ART - EXP.MAND.7.Postretention Changes in Mandibular CrowdingDocument11 pagesART - EXP.MAND.7.Postretention Changes in Mandibular CrowdingDiana Paola FontechaNo ratings yet
- Original Research Article: Burhan Showkat, Jayesh S. Rahalkar, Sandeep Jethe, Ravindra ManerikarDocument5 pagesOriginal Research Article: Burhan Showkat, Jayesh S. Rahalkar, Sandeep Jethe, Ravindra ManerikarjaslinshalinNo ratings yet
- CJN 079Document199 pagesCJN 079SelvaArockiamNo ratings yet
- Cju 005Document5 pagesCju 005gifar ihsanNo ratings yet
- Stalpers Am JOrthod Dentofac Orthop 2007132316323Document8 pagesStalpers Am JOrthod Dentofac Orthop 2007132316323thomas QuilangNo ratings yet
- Mandibular Incisor Recrowding Is It Different in Extraction and Nonextraction Cases 2247 2452.1000649Document7 pagesMandibular Incisor Recrowding Is It Different in Extraction and Nonextraction Cases 2247 2452.1000649monicaordonezNo ratings yet
- Stability of Class II Malocclusion Treatment With The Distal Jet Followed by Fixed AppliancesDocument8 pagesStability of Class II Malocclusion Treatment With The Distal Jet Followed by Fixed AppliancesFabian BarretoNo ratings yet
- 10 1067@mpr 2000 107113Document7 pages10 1067@mpr 2000 107113gbaez.88No ratings yet
- Implant-Supported Removable Partial Dentures in The Mandible A 3-16 Year Retrospective StudyDocument8 pagesImplant-Supported Removable Partial Dentures in The Mandible A 3-16 Year Retrospective StudyMohammad Fadyl YunizarNo ratings yet
- Predictors of Postretention Stability of Mandibular Dental Arch Dimensions in Patients Treated With A Lip Bumper During Mixed Dentition Followed by Fixed AppliancesDocument6 pagesPredictors of Postretention Stability of Mandibular Dental Arch Dimensions in Patients Treated With A Lip Bumper During Mixed Dentition Followed by Fixed AppliancesGABRIELA NIETO GONZALEZNo ratings yet
- A Longitudinal Study of Incremental Expansion Using A Mandibular Lip BumperDocument5 pagesA Longitudinal Study of Incremental Expansion Using A Mandibular Lip Bumperapi-26468957No ratings yet
- Stability of Unilateral Posterior Crossbite Correction in The Mixed Dentition: A Randomized Clinical Trial With A 3-Year Follow-UpDocument9 pagesStability of Unilateral Posterior Crossbite Correction in The Mixed Dentition: A Randomized Clinical Trial With A 3-Year Follow-UpPae Anusorn AmtanonNo ratings yet
- Mandibular Incisor Alignment in Untreated Subjects Compared With Long-Term Changes After OrthodonticDocument9 pagesMandibular Incisor Alignment in Untreated Subjects Compared With Long-Term Changes After OrthodonticPAOLA IVETTE MARTINEZ RODRIGUEZNo ratings yet
- Cone-Beam Computed Tomography Evaluation of Periodontal and Bone Support Loss in Extraction CasesDocument8 pagesCone-Beam Computed Tomography Evaluation of Periodontal and Bone Support Loss in Extraction CasesAlla MushkeyNo ratings yet
- Anterior Tooth Alignment A Comparison of Orthodontic Retention Regimens 5 Years PosttreatmentDocument7 pagesAnterior Tooth Alignment A Comparison of Orthodontic Retention Regimens 5 Years PosttreatmentRenan VeigaNo ratings yet
- 8 - Clinical Outcome in Periradicular Surgery Effect of Patient - and Tooth-Related Factors - A Multicenter StudyDocument8 pages8 - Clinical Outcome in Periradicular Surgery Effect of Patient - and Tooth-Related Factors - A Multicenter StudykochikaghochiNo ratings yet
- Hendrix 1994 Artigo 7 BaseDocument5 pagesHendrix 1994 Artigo 7 BaseGISELLE DE BRITO HENRIQUENo ratings yet
- Long-Term Clinical Outcome of Rapid Maxillary Expansion As The Only Treatment Performed in Class I MalocclusionDocument5 pagesLong-Term Clinical Outcome of Rapid Maxillary Expansion As The Only Treatment Performed in Class I MalocclusionMariana SantosNo ratings yet
- Long-Term Stability After Orthodontic Treatment Remains InconclusiveDocument2 pagesLong-Term Stability After Orthodontic Treatment Remains InconclusiveHabeeb AL-AbsiNo ratings yet
- NEW BUSHRA FinalDocument22 pagesNEW BUSHRA Finalmudassir rehman100% (1)
- A One Year Pilot Prospective Multicenter StudyDocument10 pagesA One Year Pilot Prospective Multicenter StudyEly Valentina Contreras ArceoNo ratings yet
- Comparison of The Effects of Rapid Maxillary ExpanDocument10 pagesComparison of The Effects of Rapid Maxillary Expancarl marxNo ratings yet
- Maxillary Dentoalveolar Assessment Following Retraction of Maxillary Incisors: A Preliminary StudyDocument8 pagesMaxillary Dentoalveolar Assessment Following Retraction of Maxillary Incisors: A Preliminary StudyAndrea TokumotoNo ratings yet
- 10 1016@j Ajodo 2016 03 020 PDFDocument10 pages10 1016@j Ajodo 2016 03 020 PDFMonojit DuttaNo ratings yet
- J Odw 2016 11 006Document6 pagesJ Odw 2016 11 006Ahmed ElsharkawyNo ratings yet
- Art 2Document6 pagesArt 2Joyce Stefania Posada MauricioNo ratings yet
- Long-Term Stability of Anterior Open-Bite Treatment by Intrusion of Maxillary Posterior TeethDocument9 pagesLong-Term Stability of Anterior Open-Bite Treatment by Intrusion of Maxillary Posterior TeethNg Chun HownNo ratings yet
- Stability of Transverse Expansion in The Mandibular ArchDocument6 pagesStability of Transverse Expansion in The Mandibular ArchManena RivoltaNo ratings yet
- EARLY Intervention in The Transverse DimensionDocument3 pagesEARLY Intervention in The Transverse DimensionBoboc FlorinNo ratings yet
- Effect of Different Incisor Movements On The Soft Tissue Profile (2016)Document9 pagesEffect of Different Incisor Movements On The Soft Tissue Profile (2016)Nicolas ValenzuelaNo ratings yet
- Anterior Tooth Wear and Retention Type Until 5 Years After Orthodontic TreatmentDocument8 pagesAnterior Tooth Wear and Retention Type Until 5 Years After Orthodontic TreatmentRenan VeigaNo ratings yet
- Long-Term Effectiveness of Canine-To-Canine Bonded Exible Spiral Wire Lingual RetainersDocument8 pagesLong-Term Effectiveness of Canine-To-Canine Bonded Exible Spiral Wire Lingual RetainersVinit SinghNo ratings yet
- Artigo BomDocument6 pagesArtigo BomCiro GassibeNo ratings yet
- A Withinpatient Comparative Study of The Influence of Number and Distribution of Ball Attachment Retained Mandibular Overdenture 1011Document6 pagesA Withinpatient Comparative Study of The Influence of Number and Distribution of Ball Attachment Retained Mandibular Overdenture 1011dentureNo ratings yet
- Evaluation of Open Bite Closure Using Clear AligneDocument9 pagesEvaluation of Open Bite Closure Using Clear AligneManuel CastilloNo ratings yet
- Cephalometric Assessment of Dentofacial Vertical Changes in Class I Subjects Treated With and Without ExtractionDocument7 pagesCephalometric Assessment of Dentofacial Vertical Changes in Class I Subjects Treated With and Without ExtractionMohamed FaragNo ratings yet
- 3205 All On Four Concept in Implant Dentistry A Literature ReviewDocument7 pages3205 All On Four Concept in Implant Dentistry A Literature ReviewAngelaBaleaNo ratings yet
- Outcome of Single Immediate Implants Placed inDocument8 pagesOutcome of Single Immediate Implants Placed injuanita enriquezNo ratings yet
- Periapical Bone Healing After ApicectomyDocument5 pagesPeriapical Bone Healing After ApicectomyMarwa Wagih ElboraeyNo ratings yet
- Miroperforaciones PDFDocument6 pagesMiroperforaciones PDFceci hdeezNo ratings yet
- Fu 2016Document10 pagesFu 2016Soe San KyawNo ratings yet
- Bone Augmentation of The Edentulous Maxilla For Implant Placement: A Systematic ReviewDocument12 pagesBone Augmentation of The Edentulous Maxilla For Implant Placement: A Systematic ReviewJarvin Miguel Buitrago GalindezNo ratings yet
- Factors Influencing The Outcome of Root-Resection Therapy in Molars: A 10-Year Retrospective StudyDocument9 pagesFactors Influencing The Outcome of Root-Resection Therapy in Molars: A 10-Year Retrospective StudyAshok KpNo ratings yet
- Agliardi - Immediate Fixed Rehabilitation ofDocument11 pagesAgliardi - Immediate Fixed Rehabilitation ofAnsaquilo AnsaquiloNo ratings yet
- A. Alineadores - L. Levrini, A. CarganicoDocument5 pagesA. Alineadores - L. Levrini, A. CarganicoYayis LondoñoNo ratings yet
- Mandibular 2 Implant Ball Bar Overdenture 10 Yaers CUNE IJP 2010Document9 pagesMandibular 2 Implant Ball Bar Overdenture 10 Yaers CUNE IJP 2010Johnny CHNo ratings yet
- Cerny Fixed RetainerDocument88 pagesCerny Fixed Retainerchinchiayeh5699No ratings yet
- Skeletal Anchorage Augmentation in Extraction/Nonextraction Orthodontic Treatment: A Randomized Clinical StudyDocument13 pagesSkeletal Anchorage Augmentation in Extraction/Nonextraction Orthodontic Treatment: A Randomized Clinical Studyaleja.b7815No ratings yet
- 1 s2.0 S088954061001005X MainDocument6 pages1 s2.0 S088954061001005X MainPanaite TinelaNo ratings yet
- Therapeutic Changes in Extraction Versus Non-Extraction Orthodontic TreatmentDocument12 pagesTherapeutic Changes in Extraction Versus Non-Extraction Orthodontic Treatmentmohamed chaaboubNo ratings yet
- Magnetic BBDocument7 pagesMagnetic BBVicente ContrerasNo ratings yet
- What-are-the-Surgical-Movements-in-Orthognathic-Surgery-That-Most-Affect-the-Upper-Airways-A-Three-Dimensional-AnalysisDocument13 pagesWhat-are-the-Surgical-Movements-in-Orthognathic-Surgery-That-Most-Affect-the-Upper-Airways-A-Three-Dimensional-Analysisr1maxilo2021No ratings yet
- Does The Maxillary Midline Diastema Close After Frenectomy?: Oral SurgeryDocument10 pagesDoes The Maxillary Midline Diastema Close After Frenectomy?: Oral Surgeryantonio dlNo ratings yet
- Implant Therapy: Clinical Approaches and Evidence of Success, Second EditionFrom EverandImplant Therapy: Clinical Approaches and Evidence of Success, Second EditionNo ratings yet
- Rahman MD Matiur-2230130236-10noDocument4 pagesRahman MD Matiur-2230130236-10noadnanNo ratings yet
- Open Printable/Searchable Copy (PDF Format) : Global Mapper User's ManualDocument361 pagesOpen Printable/Searchable Copy (PDF Format) : Global Mapper User's ManualIrwan RusmanaNo ratings yet
- Activity 2: Mathematical Modeling of Physical SystemsDocument10 pagesActivity 2: Mathematical Modeling of Physical SystemsNico SilorioNo ratings yet
- The History and Evolution of QuaternionsDocument3 pagesThe History and Evolution of QuaternionsAnton Van WykNo ratings yet
- FURLEY, David J. (1981) - The Greek Theory of The Infinite UniverseDocument16 pagesFURLEY, David J. (1981) - The Greek Theory of The Infinite UniverseAri CostamagnaNo ratings yet
- Keepers Smart Contracts Audit v0.1 GingerSecDocument60 pagesKeepers Smart Contracts Audit v0.1 GingerSecAbhishek ShuklaNo ratings yet
- Quality Assurance of Pressure-Sensitive Tapes: Standard Practice ForDocument6 pagesQuality Assurance of Pressure-Sensitive Tapes: Standard Practice ForYoga PradanaNo ratings yet
- Jeep-Willys DmiDocument14 pagesJeep-Willys DmiGabriel Fodor100% (1)
- Matter-Nature and Behaviour (Conceptual Questions With Very Short Answers)Document4 pagesMatter-Nature and Behaviour (Conceptual Questions With Very Short Answers)Syed Mazhar AliNo ratings yet
- XLPE Polyethylene Lifetime Detection PDFDocument120 pagesXLPE Polyethylene Lifetime Detection PDFconqiuNo ratings yet
- Atmel ATmega328 Test Circuit DiagramDocument6 pagesAtmel ATmega328 Test Circuit Diagramcadeyare2No ratings yet
- Shoes Shop Online WebsiteDocument26 pagesShoes Shop Online WebsiteNguyễn HưngNo ratings yet
- Masonry TutorialDocument45 pagesMasonry TutorialGajendra Joshi100% (2)
- Steam Tables AsmeDocument32 pagesSteam Tables AsmeNatsNo ratings yet
- Freeman Et Al The Condor 2019Document11 pagesFreeman Et Al The Condor 2019Guilain TSETAGHONo ratings yet
- Unit 2Document3 pagesUnit 2lewlking123No ratings yet
- Scratch Tester 430Document4 pagesScratch Tester 430laboratorioNo ratings yet
- Design, Implementation and Verification of 32-Bit ALU With VIODocument6 pagesDesign, Implementation and Verification of 32-Bit ALU With VIONubia DiazNo ratings yet
- Nouradini PDFDocument15 pagesNouradini PDFDavi AhmadNo ratings yet
- Evc Drive User Manual en Us 160814Document142 pagesEvc Drive User Manual en Us 160814Coil98No ratings yet
- Useful Note For SEF Quiz No.1Document12 pagesUseful Note For SEF Quiz No.1ganamuNo ratings yet
- 01-Introduction To VSCDocument30 pages01-Introduction To VSCeng7senNo ratings yet
- Flexible Sprinkler ConnectionDocument5 pagesFlexible Sprinkler ConnectionOwais AhmedNo ratings yet
- Step by Step 1 PDFDocument164 pagesStep by Step 1 PDFMohamed Ali100% (1)
- B. TECH 2nd Semester June 2019-1 PDFDocument5 pagesB. TECH 2nd Semester June 2019-1 PDFHarshitNo ratings yet
- 7sd522 SiemensDocument17 pages7sd522 SiemensSanthosh Kumar VinayagamNo ratings yet
- The Fundamentals of End MillsDocument3 pagesThe Fundamentals of End MillsILikeScribd5050No ratings yet
- Sample Form Inspection ChecklistDocument5 pagesSample Form Inspection Checklistadolf001No ratings yet
- The Scalpel Finishing Technique: A Tooth-Friendly Way To Finish Dental Composites in Anterior TeethDocument18 pagesThe Scalpel Finishing Technique: A Tooth-Friendly Way To Finish Dental Composites in Anterior TeethSoraya BouchammaNo ratings yet