Download as pdf or txt
You might also like
- James Tin Yau So - Treatment of Disease With AcupunctureDocument397 pagesJames Tin Yau So - Treatment of Disease With Acupuncturearyaa202096% (26)
- Sop For NsiDocument4 pagesSop For NsiDR KAMAL SUNANo ratings yet
- Applied Nursing Research: Original ArticleDocument8 pagesApplied Nursing Research: Original ArticleWahyonoNo ratings yet
- Efficacy of Occupational Therapy For Patients With Parkinson's Disease: A Randomised Controlled Trial (Vol 13, PG 557, 2014)Document11 pagesEfficacy of Occupational Therapy For Patients With Parkinson's Disease: A Randomised Controlled Trial (Vol 13, PG 557, 2014)Samantha ColleNo ratings yet
- Occupational Therapy and Physiotherapy Benefit The Acute Patient Pathway: A Mixed-Methods StudyDocument12 pagesOccupational Therapy and Physiotherapy Benefit The Acute Patient Pathway: A Mixed-Methods StudyIlvita MayasariNo ratings yet
- Predictors of Psych Intervention To Promote Health Behaviour Adherence in HF 2021Document14 pagesPredictors of Psych Intervention To Promote Health Behaviour Adherence in HF 2021Bob JoeNo ratings yet
- Measuring Person-Centred Care in Nurse-Led Outpatient Rheumatology ClinicsDocument20 pagesMeasuring Person-Centred Care in Nurse-Led Outpatient Rheumatology ClinicsBengt HörbergNo ratings yet
- 10 1002nop2 861Document8 pages10 1002nop2 861Fanni VikorNo ratings yet
- Case Study #3Document26 pagesCase Study #3Reshma MohabeirNo ratings yet
- Session 1 - Manuskrip SR M11 - Innani Wildania Husna - Innani Wildania With CommentsDocument15 pagesSession 1 - Manuskrip SR M11 - Innani Wildania Husna - Innani Wildania With Commentsrenata JeslynNo ratings yet
- Utilización de Tecnologías Móviles en Pacientes Con Psicosis Una Revisión SistemáticaDocument11 pagesUtilización de Tecnologías Móviles en Pacientes Con Psicosis Una Revisión SistemáticaDiego BolívarNo ratings yet
- His 9Document158 pagesHis 9Anjum100% (6)
- Metaanalisis Castro Et Al. 2019Document37 pagesMetaanalisis Castro Et Al. 2019LauraNo ratings yet
- Jurnal 5Document9 pagesJurnal 5raraNo ratings yet
- Idiopathic Interstitial PneumoniaDocument7 pagesIdiopathic Interstitial PneumoniaHunter InsaneNo ratings yet
- Bommersbach (2021) - Mental Health Staff Perceptions of Improvement Opportunities Around Covid 19Document14 pagesBommersbach (2021) - Mental Health Staff Perceptions of Improvement Opportunities Around Covid 19Maximiliano AzconaNo ratings yet
- International Scholarly Research Notices - 2014 - Han - Neuropsychology in Multidisciplinary Stroke Care ClinicalDocument6 pagesInternational Scholarly Research Notices - 2014 - Han - Neuropsychology in Multidisciplinary Stroke Care Clinicalbam.kinney14No ratings yet
- Niemann 37Document19 pagesNiemann 37banitavlad5No ratings yet
- Telerehabilitation System in Nursing Post Stroke - A Systematic ReviewDocument6 pagesTelerehabilitation System in Nursing Post Stroke - A Systematic ReviewErfin WatiNo ratings yet
- Impact - Ijranss-1. Ijranss - Length of Stay Reporting in Forensic Secure Care Can Be Augmented by An Overarching Framework To Map Patient Journey in Mentally Disordered Offender Pathway ForDocument38 pagesImpact - Ijranss-1. Ijranss - Length of Stay Reporting in Forensic Secure Care Can Be Augmented by An Overarching Framework To Map Patient Journey in Mentally Disordered Offender Pathway ForImpact JournalsNo ratings yet
- Non-Pharmacological Therapies For Post-Viral Syndromes, Including Long COVID: A Systematic ReviewDocument28 pagesNon-Pharmacological Therapies For Post-Viral Syndromes, Including Long COVID: A Systematic ReviewNailton Albuquerque FilhoNo ratings yet
- Journal Homepage: - : Introduction:-Objectives of The StudyDocument4 pagesJournal Homepage: - : Introduction:-Objectives of The StudyIJAR JOURNALNo ratings yet
- 1 s2.0 S1201971214017214 Main PDFDocument5 pages1 s2.0 S1201971214017214 Main PDFYohanna ekasntNo ratings yet
- Hex 21 41Document16 pagesHex 21 41fadedoyinNo ratings yet
- Phillips Postanaesthetic 2013Document11 pagesPhillips Postanaesthetic 2013Alex PiecesNo ratings yet
- Gade 2008Document11 pagesGade 2008Agustina IturriNo ratings yet
- Homebasedtelehealth PDFDocument6 pagesHomebasedtelehealth PDFdaniel serraniNo ratings yet
- International Journal of Pharmacy Practice AbstractsDocument40 pagesInternational Journal of Pharmacy Practice AbstractsFabiola NogaNo ratings yet
- Journal Pre-Proof: Kidney MedicineDocument38 pagesJournal Pre-Proof: Kidney MedicineMohammed Shuaib AhmedNo ratings yet
- Characteristics of Case Management in Primary Care PDFDocument11 pagesCharacteristics of Case Management in Primary Care PDFCamila AlmeidaNo ratings yet
- Report of The Nih Task Force On Research Standards For Chronic Low Back PainDocument42 pagesReport of The Nih Task Force On Research Standards For Chronic Low Back PainDragos BourosNo ratings yet
- The Role of Digital Health in Supporting Cancer Patients-1-8Document8 pagesThe Role of Digital Health in Supporting Cancer Patients-1-8EduardoNo ratings yet
- The Role of Digital Health in Supporting Cancer PatientsDocument19 pagesThe Role of Digital Health in Supporting Cancer PatientsEduardoNo ratings yet
- Ebp Final DraftDocument14 pagesEbp Final Draftapi-436039292No ratings yet
- (Journal of Neurosurgery - Spine) Patient Misconceptions Concerning Lumbar Spondylosis Diagnosis and TreatmentDocument7 pages(Journal of Neurosurgery - Spine) Patient Misconceptions Concerning Lumbar Spondylosis Diagnosis and Treatmentefancoolhand09No ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Neurologist Communicationg The Diagnosis of ELADocument9 pagesNeurologist Communicationg The Diagnosis of ELAHabib G. Moutran BarrosoNo ratings yet
- Vgi FX CaderaDocument8 pagesVgi FX CaderaLuz Veronica Taipe MorveliNo ratings yet
- تنزيلDocument9 pagesتنزيلrazanyahya440No ratings yet
- Applications of Telecounselling in Spinal Cord Injury Rehabilitation: A Systematic Review With Effect SizesDocument13 pagesApplications of Telecounselling in Spinal Cord Injury Rehabilitation: A Systematic Review With Effect Sizesjustin_saneNo ratings yet
- Evaluating Preferences For Online Psychological Interventions - 2023 - PsychiatDocument10 pagesEvaluating Preferences For Online Psychological Interventions - 2023 - Psychiattito syahjihadNo ratings yet
- Fisher 2017Document6 pagesFisher 2017Bogdan NeamtuNo ratings yet
- Effectiveness - Primary CareDocument10 pagesEffectiveness - Primary Care...No ratings yet
- Integrated Review of The Literaute FinalDocument31 pagesIntegrated Review of The Literaute Finalapi-547372251No ratings yet
- Example of PHD Research ProposalDocument2 pagesExample of PHD Research ProposalMuhammad Khurram ShahzadNo ratings yet
- Patient Safety During Sedation by Anesthesia ProfeDocument8 pagesPatient Safety During Sedation by Anesthesia ProfeIsmar MorenoNo ratings yet
- Non Medical Prescribing Literature ReviewDocument6 pagesNon Medical Prescribing Literature Reviewc5rm5y5p100% (1)
- Psychotic Disorders and Telepsych 3Document13 pagesPsychotic Disorders and Telepsych 3Maria Von ShaftNo ratings yet
- HPTN 074: HIV Prevention Trial Network 074Document23 pagesHPTN 074: HIV Prevention Trial Network 074Suardy CiayadiNo ratings yet
- Arm 21119Document14 pagesArm 21119nasrilche123No ratings yet
- Evaluation of A National Telemedicine Initiative in The Veterans Health Administration: Factors Associated With Successful ImplementationDocument11 pagesEvaluation of A National Telemedicine Initiative in The Veterans Health Administration: Factors Associated With Successful ImplementationKarl Benedict OngNo ratings yet
- 2007 CESItem Level PsychometricsDocument15 pages2007 CESItem Level PsychometricsCamila Andrea Barrera BlancoNo ratings yet
- Delirium and Associated Length of Stay and Costs in Critically Ill PatientsDocument8 pagesDelirium and Associated Length of Stay and Costs in Critically Ill PatientsedavioNo ratings yet
- Impact of Technology in Better Dispersal of HealthDocument4 pagesImpact of Technology in Better Dispersal of Healthvasthu broto ariyoNo ratings yet
- Physical Activity Coaching Via Telehealth For.3Document11 pagesPhysical Activity Coaching Via Telehealth For.3Montserrat Suárez SánchezNo ratings yet
- Prodinger 2015Document9 pagesProdinger 2015Liliana Patricia Rodriguez VegaNo ratings yet
- Academic Emergency Medicine - 2020 - Ebell - Accuracy of Signs and Symptoms For The Diagnosis of Community AcquiredDocument14 pagesAcademic Emergency Medicine - 2020 - Ebell - Accuracy of Signs and Symptoms For The Diagnosis of Community AcquiredOnilis RiveraNo ratings yet
- HPTN 074: HIV Prevention Trial Network 074Document23 pagesHPTN 074: HIV Prevention Trial Network 074Tulus Dyah AnggraeniNo ratings yet
- HSS Dysphagia and Dysphonia Inventory (HSS-DDI) Following Anterior Cervical FusionDocument10 pagesHSS Dysphagia and Dysphonia Inventory (HSS-DDI) Following Anterior Cervical FusionLarissa MeloNo ratings yet
- Evaluation of The Feedback On Pharmacovigilance Basic Awareness Program Amongst The Medical Post Graduate Residents of A Rural Teaching HospitalDocument6 pagesEvaluation of The Feedback On Pharmacovigilance Basic Awareness Program Amongst The Medical Post Graduate Residents of A Rural Teaching HospitalIJAR JOURNALNo ratings yet
- Journal Review Final PaperDocument10 pagesJournal Review Final Paperapi-464793486No ratings yet
- Finding the Path in Alzheimer’s Disease: Early Diagnosis to Ongoing Collaborative CareFrom EverandFinding the Path in Alzheimer’s Disease: Early Diagnosis to Ongoing Collaborative CareNo ratings yet
- Pain & SympDocument4 pagesPain & SympxxdissuNo ratings yet
- 2024 Rheumatology Student-Clinician HandbookDocument8 pages2024 Rheumatology Student-Clinician HandbookMusimbi MourineNo ratings yet
- Endocrine System (Pathophysiology)Document18 pagesEndocrine System (Pathophysiology)roselle legson100% (1)
- Self Management SkillsDocument9 pagesSelf Management SkillsMerly PerezNo ratings yet
- Research Design, Biostatistics, and Literature Evaluation: Ishaq Lat, Pharm.D., FCCP, FCCM, BCPSDocument18 pagesResearch Design, Biostatistics, and Literature Evaluation: Ishaq Lat, Pharm.D., FCCP, FCCM, BCPSJeremy HamptonNo ratings yet
- Covid-19 Here in San Carlos City, NegrosDocument26 pagesCovid-19 Here in San Carlos City, NegrosMay LimbagaNo ratings yet
- IM HandbookDocument430 pagesIM HandbookPhil ChanNo ratings yet
- Principles of Drug AdministrationDocument4 pagesPrinciples of Drug Administrationlei ruminganNo ratings yet
- Revised Preauth Form IRDADocument5 pagesRevised Preauth Form IRDASurbhi SinghNo ratings yet
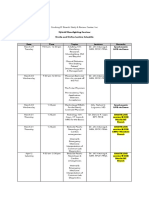
- Hybrid Moonlighting Seminar ScheduleDocument2 pagesHybrid Moonlighting Seminar ScheduleSanielle Karla Garcia LorenzoNo ratings yet
- Tertiaryhospital PDFDocument2 pagesTertiaryhospital PDFRANILENo ratings yet
- Ostemyelitis by Pseudomonas Aeruginosa I PDFDocument1 pageOstemyelitis by Pseudomonas Aeruginosa I PDFJúlio SimõesNo ratings yet
- Health Guard: Bajaj AllianzDocument35 pagesHealth Guard: Bajaj AllianzAlexNo ratings yet
- Disease Control Priority-3Document23 pagesDisease Control Priority-3Abubakar Abdhoo100% (1)
- Some of These Questions Are Personal, and Your Answers Will Be Confidential and Private-Only The MCO Will Get This InformationDocument2 pagesSome of These Questions Are Personal, and Your Answers Will Be Confidential and Private-Only The MCO Will Get This InformationKing Aldus ConstantinoNo ratings yet
- 2011 01 - ACF-F - Nutrition Program Manager Test VF (ENG - BLANK)Document5 pages2011 01 - ACF-F - Nutrition Program Manager Test VF (ENG - BLANK)Javed Ahmed Chandio100% (2)
- NiceDocument45 pagesNiceKenneth Mark B. TevesNo ratings yet
- Endocrinologie Si Nursing Curs 3Document4 pagesEndocrinologie Si Nursing Curs 3gabiflori100% (1)
- Navigation FessDocument5 pagesNavigation FessAravind NooneyNo ratings yet
- Early Regular Egg Exposure in Infants With Eczema: A Randomized Controlled TrialDocument7 pagesEarly Regular Egg Exposure in Infants With Eczema: A Randomized Controlled TrialnicloverNo ratings yet
- Problems On EpidemiologyDocument146 pagesProblems On EpidemiologyAnnie HadassahNo ratings yet
- Servsafe Chapter 2Document66 pagesServsafe Chapter 2Simon Fabon100% (1)
- Bioreactor Concepts For Cell Culture-Based Viral Vaccine ProductionDocument15 pagesBioreactor Concepts For Cell Culture-Based Viral Vaccine ProductionJohn Lloyd GenerosoNo ratings yet
- Contoh RPP Bahasa Inggris Untuk Akademi KebidananDocument29 pagesContoh RPP Bahasa Inggris Untuk Akademi KebidananDwi RamadhaniNo ratings yet
- Imbalance Nutrition Less Than Body RequirementsDocument4 pagesImbalance Nutrition Less Than Body Requirementshatred heartNo ratings yet
- Communicable Disease PresentationDocument67 pagesCommunicable Disease PresentationMonaNo ratings yet
- Republic of The Philippines Tamag, Vigan City 2700 Ilocos Sur Website: MailDocument2 pagesRepublic of The Philippines Tamag, Vigan City 2700 Ilocos Sur Website: MailRenea Joy ArruejoNo ratings yet
- Personalized AyurvedDocument13 pagesPersonalized AyurvedAtul WaghNo ratings yet