Download as xlsx, pdf, or txt
You might also like
- Data Analysis ProcedureDocument5 pagesData Analysis Procedureabebelema100% (9)
- Integrated Application Form (XLSX Format)Document42 pagesIntegrated Application Form (XLSX Format)Hazel BisaNo ratings yet
- 2-E.BMR Liquid InjectionDocument28 pages2-E.BMR Liquid InjectionMohammed Zubair100% (7)
- CRO and Sponsor - Integrated Application FormDocument4 pagesCRO and Sponsor - Integrated Application FormNaevisweloveuNo ratings yet
- Risk Assessment - HV 11kV Cable, Joint & TerminationDocument90 pagesRisk Assessment - HV 11kV Cable, Joint & TerminationJobish PK0% (2)
- Email Worksheet: Application Process OverviewDocument27 pagesEmail Worksheet: Application Process OverviewIsabel PeraltaNo ratings yet
- Amcc 7-322Document15 pagesAmcc 7-322khara teanoNo ratings yet
- Fda FormDocument14 pagesFda FormCharry MarquezNo ratings yet
- Integrated ApplicationForm (BLANK)Document42 pagesIntegrated ApplicationForm (BLANK)Reggie Theresa MarquezNo ratings yet
- Email Worksheet: Application Process OverviewDocument16 pagesEmail Worksheet: Application Process OverviewBibi BoboyNo ratings yet
- Tender DetailsDocument2 pagesTender DetailsArindam PaulNo ratings yet
- Complete Sample Copy3Document12 pagesComplete Sample Copy3Prep RCNo ratings yet
- FAQ: Product RegistrationDocument5 pagesFAQ: Product RegistrationCalvin WangNo ratings yet
- Initial Cosmetics TraderDocument4 pagesInitial Cosmetics TradersalemcarolineNo ratings yet
- Tender DetailsDocument2 pagesTender DetailsArindam PaulNo ratings yet
- BV Standard Sa Factory Profile Management Interview Rev 2 20jan06 (Internal)Document2 pagesBV Standard Sa Factory Profile Management Interview Rev 2 20jan06 (Internal)Adi FauziNo ratings yet
- Evolution V6 Lesson 1 LEDocument38 pagesEvolution V6 Lesson 1 LEFanuel NjobvuNo ratings yet
- SPP LogDocument1 pageSPP Logazrul shahNo ratings yet
- 4.4.2 Request - Certification Service 22.08.17Document3 pages4.4.2 Request - Certification Service 22.08.17bobby francis dela rosaNo ratings yet
- FDA-Circular-No.-2020-030-1 EservicesDocument34 pagesFDA-Circular-No.-2020-030-1 EservicesMedSure PharmacyNo ratings yet
- Solar Nit NFRDocument1 pageSolar Nit NFRscarce.genes.0mNo ratings yet
- Intellectual Property Office of The PhilippinesDocument2 pagesIntellectual Property Office of The Philippinesmiggy13No ratings yet
- SupplierDocument7 pagesSupplier4Chat GptNo ratings yet
- Tender DetailsDocument2 pagesTender DetailsArindam PaulNo ratings yet
- Documents Required For West Bengal On Line TenderDocument3 pagesDocuments Required For West Bengal On Line TenderDipankar ChatterjeeNo ratings yet
- Op QD 015Document5 pagesOp QD 015ujangketul62100% (1)
- SUGAMDocument22 pagesSUGAMSreedhar TirunagariNo ratings yet
- Published Niet 08Document3 pagesPublished Niet 08SOUMYA BHATTNo ratings yet
- Manual - IMPORTED FOOD INSPECTION SYSTEM A WINDOW FOR CIVIL PETITIONS (22.10.27.)Document26 pagesManual - IMPORTED FOOD INSPECTION SYSTEM A WINDOW FOR CIVIL PETITIONS (22.10.27.)letruongngocminhquyenNo ratings yet
- Tender DetailsDocument2 pagesTender DetailsArindam PaulNo ratings yet
- Abra Provincial Hospital: Quality ProcedureDocument2 pagesAbra Provincial Hospital: Quality ProcedureFritz N. TurquezaNo ratings yet
- OCA - 115c - Initial Application (Processing & Trading) - 181119Document4 pagesOCA - 115c - Initial Application (Processing & Trading) - 181119jamil voraNo ratings yet
- USER MANUAL VENDOR Bank Sumsel BabelDocument28 pagesUSER MANUAL VENDOR Bank Sumsel BabelHaryo Kusuma Wibawa, ST, CPCNo ratings yet
- Email Worksheet: Application Process OverviewDocument19 pagesEmail Worksheet: Application Process OverviewnetmiNo ratings yet
- Five Pump Fire StationDocument132 pagesFive Pump Fire StationArindam PaulNo ratings yet
- Haz 2Document16 pagesHaz 2Jalagandeeswaran KalimuthuNo ratings yet
- 1J5 S4hana1809 BPD en BRDocument39 pages1J5 S4hana1809 BPD en BRMarcelo MilhomemNo ratings yet
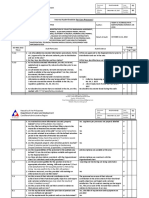
- Internal Audit Checklist (For Core Processes) : Issue Number: Effective Date: Document CodeDocument5 pagesInternal Audit Checklist (For Core Processes) : Issue Number: Effective Date: Document CodejulyenfortunatoNo ratings yet
- SOP For Calibration of FT-IR SpectrometerDocument8 pagesSOP For Calibration of FT-IR SpectrometerSolomon Gamanuel100% (1)
- Registration GuideDocument10 pagesRegistration Guideriski odeNo ratings yet
- 2020ENZAA409118069smeta PaFru FEB 20 KCHDocument59 pages2020ENZAA409118069smeta PaFru FEB 20 KCHHichamDouiebNo ratings yet
- Supplier'S Assessment Form: Amit Engineering WorksDocument4 pagesSupplier'S Assessment Form: Amit Engineering Worksranjeet singhNo ratings yet
- Supplier 2a UsDocument5 pagesSupplier 2a Ustyui876No ratings yet
- Structured System Analysis and Design MethodDocument18 pagesStructured System Analysis and Design MethodsudarakagamageNo ratings yet
- PC ApplicationQuestionnaireSPO FO 23 enDocument7 pagesPC ApplicationQuestionnaireSPO FO 23 enduy02091989No ratings yet
- FAQs On OTS Registration ProcessDocument3 pagesFAQs On OTS Registration ProcessNARASIMHA CHIYYADRINo ratings yet
- SBMA - Business Registration Application PDFDocument6 pagesSBMA - Business Registration Application PDFfallingobjectNo ratings yet
- 48v Box InputDocument2 pages48v Box InputHammadAlviNo ratings yet
- MD050 - PHD PO Invoice Tracking With PO V2Document12 pagesMD050 - PHD PO Invoice Tracking With PO V2Mohamed IbrahimNo ratings yet
- MAF - Domestic - FinalDocument6 pagesMAF - Domestic - FinalSumit BhamisaraNo ratings yet
- CE User Guide PDFDocument62 pagesCE User Guide PDFARKA DEEPNo ratings yet
- ASOC ManualDocument39 pagesASOC Manualkarthik venegallaNo ratings yet
- BOC - Import License ApplicationDocument6 pagesBOC - Import License ApplicationRaeanne Sabado BangitNo ratings yet
- FDA Circular No. 2021 012 Annex A ClearDocument14 pagesFDA Circular No. 2021 012 Annex A ClearDayne Ocampo-SolimanNo ratings yet
- Factory Profile - Management Interview - Rev 3Document3 pagesFactory Profile - Management Interview - Rev 3Hưng LưuNo ratings yet
- BRD - BFO and TOCDocument10 pagesBRD - BFO and TOCRashika GuptaNo ratings yet
- JV-P08 Corrective Action (OK)Document41 pagesJV-P08 Corrective Action (OK)BÍCH NGUYỄNNo ratings yet
- Onlinesales UserManualDocument81 pagesOnlinesales UserManualNish NíShänthNo ratings yet
- X Checklist - IECDocument4 pagesX Checklist - IECadministratorNo ratings yet
- Itop Portal Manual - 0 PDFDocument12 pagesItop Portal Manual - 0 PDFwassimaNo ratings yet
- Act5 BATCH MANUFACTURING RECORDDocument4 pagesAct5 BATCH MANUFACTURING RECORDIsabel PeraltaNo ratings yet
- Exercise 5 - QC 1Document2 pagesExercise 5 - QC 1Isabel PeraltaNo ratings yet
- APPGP MFG OC G4 PD UNIT DOSE AND BATCH FORMULATIONDocument5 pagesAPPGP MFG OC G4 PD UNIT DOSE AND BATCH FORMULATIONIsabel PeraltaNo ratings yet
- Application Letter FormatDocument1 pageApplication Letter FormatIsabel PeraltaNo ratings yet
- Activity 2BUSINESSPLANDocument3 pagesActivity 2BUSINESSPLANIsabel PeraltaNo ratings yet
- Clinical Pharmacy Laboratory ExercisesDocument18 pagesClinical Pharmacy Laboratory ExercisesIsabel PeraltaNo ratings yet
- ACT. 4 WarehouseDocument2 pagesACT. 4 WarehouseIsabel PeraltaNo ratings yet
- Chlorides of Sodium, Calcium and Potassium Chlorides of Sodium, Calcium and PotassiumDocument1 pageChlorides of Sodium, Calcium and Potassium Chlorides of Sodium, Calcium and PotassiumIsabel PeraltaNo ratings yet
- Ppgp-Mfg-Oc G3 - Pd-2 - CP, CPP, Cqa NOTES On The ActivityDocument5 pagesPpgp-Mfg-Oc G3 - Pd-2 - CP, CPP, Cqa NOTES On The ActivityIsabel Peralta50% (2)
- ACT5LABELDocument1 pageACT5LABELIsabel PeraltaNo ratings yet
- EXP5 ManuflabDocument2 pagesEXP5 ManuflabIsabel PeraltaNo ratings yet
- Final Ampule Box Esquijo LopezDocument1 pageFinal Ampule Box Esquijo LopezIsabel PeraltaNo ratings yet
- PPGP MFG Oc g4 PD Unit Dose and Batch FormulationDocument3 pagesPPGP MFG Oc g4 PD Unit Dose and Batch FormulationIsabel PeraltaNo ratings yet
- Experiment 1 LABELDocument6 pagesExperiment 1 LABELIsabel PeraltaNo ratings yet
- Email Worksheet: Application Process OverviewDocument27 pagesEmail Worksheet: Application Process OverviewIsabel PeraltaNo ratings yet
- Assignment A. List Down The Processes in Drug Development and Explain EachDocument2 pagesAssignment A. List Down The Processes in Drug Development and Explain EachIsabel PeraltaNo ratings yet
- PHM 302L: Pharmacognosy and Plant Chemistry: Week 4: Experiment 9 ResinsDocument23 pagesPHM 302L: Pharmacognosy and Plant Chemistry: Week 4: Experiment 9 ResinsIsabel PeraltaNo ratings yet
- FPPGP MFG OC G4 PD UNIT DOSE AND BATCH FORMULATIONDocument4 pagesFPPGP MFG OC G4 PD UNIT DOSE AND BATCH FORMULATIONIsabel PeraltaNo ratings yet
- Factors To Consider in Development of Nutraceutical and Dietary SupplementsDocument5 pagesFactors To Consider in Development of Nutraceutical and Dietary SupplementsIsabel PeraltaNo ratings yet
- Perpetual Help College of Manila: Business PlanDocument14 pagesPerpetual Help College of Manila: Business PlanIsabel PeraltaNo ratings yet
- PHM304: Microbiology and Parasitology: Week 2: Parasitic InfectionDocument36 pagesPHM304: Microbiology and Parasitology: Week 2: Parasitic InfectionIsabel PeraltaNo ratings yet
- Isabel P. Esquijo Bs Pharmacy Science, Technology and SocietyDocument2 pagesIsabel P. Esquijo Bs Pharmacy Science, Technology and SocietyIsabel PeraltaNo ratings yet
- AQA-Physics Experiments PDFDocument63 pagesAQA-Physics Experiments PDFAnonymous zfqrXhuNo ratings yet
- Cot1 DLPDocument11 pagesCot1 DLPNelvie DatuNo ratings yet
- Excel Skills For Data Analytics and Visualization: InstructionsDocument6 pagesExcel Skills For Data Analytics and Visualization: InstructionsKAPIL MBA 2021-23 (Delhi)No ratings yet
- Challenges Faced by An Economics TeacherDocument8 pagesChallenges Faced by An Economics TeacherSanjay mehta100% (4)
- Lec 3 (Linked List)Document12 pagesLec 3 (Linked List)Dr LolaNo ratings yet
- AWTI Calendar 23-24 - MergedDocument17 pagesAWTI Calendar 23-24 - MergedArnel MagbojosNo ratings yet
- Introduction To LinguisticsDocument14 pagesIntroduction To LinguisticsasdfadsNo ratings yet
- 2020engg Cap2 CutoffDocument1,115 pages2020engg Cap2 Cutofframeshdorage12No ratings yet
- Unit 0 - Friends Word of Self, Family and Friends Writing SpeakingDocument14 pagesUnit 0 - Friends Word of Self, Family and Friends Writing SpeakinglelaNo ratings yet
- Lesson - 3 Periodic TableDocument19 pagesLesson - 3 Periodic TableHeaven varghese C S C SNo ratings yet
- Unit-2 Design ConceptsDocument37 pagesUnit-2 Design ConceptsNeo TarunNo ratings yet
- Unit-1 Chemistry (Matter) Lesson 1-A Properties of Matter-Solid, Liquid, and Gas (Grade 3) ObjectivesDocument16 pagesUnit-1 Chemistry (Matter) Lesson 1-A Properties of Matter-Solid, Liquid, and Gas (Grade 3) Objectiveshaizelle resmaNo ratings yet
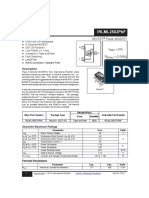
- Infineon IRLML2502 DataSheet v01 - 01 ENDocument10 pagesInfineon IRLML2502 DataSheet v01 - 01 ENabbaseftekhariNo ratings yet
- Emf Values of Organic CompoundsDocument34 pagesEmf Values of Organic CompoundsPrabir SahaNo ratings yet
- Why Use Analysis Up-Front in The Design Cycle?: CosmosDocument8 pagesWhy Use Analysis Up-Front in The Design Cycle?: CosmosRoshni BishtNo ratings yet
- Bangladesh Police: Government of The People's Republic of BangladeshDocument1 pageBangladesh Police: Government of The People's Republic of BangladeshHIPG Pro Gaming100% (1)
- Castrol Enduron 10W-40Document2 pagesCastrol Enduron 10W-40Chun-Nien LaiNo ratings yet
- Group 3 Written Report Unit III 1Document8 pagesGroup 3 Written Report Unit III 1Almere AzurNo ratings yet
- Personality Development2022 23Document6 pagesPersonality Development2022 23Veena VaishyNo ratings yet
- Aesop Sustainability Report 2021 1670404443Document33 pagesAesop Sustainability Report 2021 1670404443eNo ratings yet
- Specific Heat Capacities WorksheetDocument2 pagesSpecific Heat Capacities WorksheetRebeca RiveraNo ratings yet
- Embankment Construction MethodologyDocument16 pagesEmbankment Construction MethodologyTinwin HtutNo ratings yet
- PERIODIC TEST - Docx (N)Document2 pagesPERIODIC TEST - Docx (N)Sooraj RajmohanNo ratings yet
- The Goodheart-Willcox Co., Inc.: Publisher Tinley Park, IllinoisDocument23 pagesThe Goodheart-Willcox Co., Inc.: Publisher Tinley Park, IllinoisSaurav ShresthaNo ratings yet
- Leviton AppNote RetentionForceTechnologyDocument5 pagesLeviton AppNote RetentionForceTechnologySajeda M. Al-TalafhaNo ratings yet
- (Bradford Books) Sidney I. Wiener, Jeffrey S. Taube - Head Direction Cells and The Neural Mechanisms of Spatial Orientation-The MIT Press (2005)Document503 pages(Bradford Books) Sidney I. Wiener, Jeffrey S. Taube - Head Direction Cells and The Neural Mechanisms of Spatial Orientation-The MIT Press (2005)Víctor FuentesNo ratings yet
- Determination of Water Potential in A Plant PartDocument3 pagesDetermination of Water Potential in A Plant PartMishti2No ratings yet
- How To Design An Innovative WorkplaceDocument2 pagesHow To Design An Innovative WorkplacemuskanNo ratings yet
- Management 3-4-1Document9 pagesManagement 3-4-1Jewel Galvez OctavianoNo ratings yet