
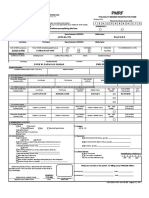
Please Note Any Pre-Application Not Fully Completed Will Be Returned To Applicant
Please Note Any Pre-Application Not Fully Completed Will Be Returned To Applicant
You might also like
- Andrea 2020 Federal Income Tax ReturnDocument11 pagesAndrea 2020 Federal Income Tax ReturnMorenita Pareles100% (1)
- India Maternity FormsDocument3 pagesIndia Maternity FormsJagadish ReddyNo ratings yet
- Insular Life Insurance FormDocument2 pagesInsular Life Insurance FormEarl Cortez0% (1)
- Personal Record: Filipino Iglesia Ni Cristo San Fernando City La UnionDocument3 pagesPersonal Record: Filipino Iglesia Ni Cristo San Fernando City La UnionManolito MacanasNo ratings yet
- Student Individual Inventory: Pangasinan Division Ii Bautista National High SchoolDocument2 pagesStudent Individual Inventory: Pangasinan Division Ii Bautista National High SchoolMichael JunioNo ratings yet
- UPDATED CIF Jul 2021 SAMPLE ONLYDocument2 pagesUPDATED CIF Jul 2021 SAMPLE ONLYChristine Anne PostradoNo ratings yet
- Degamo Incident FormDocument3 pagesDegamo Incident FormJohn Rey LogrosaNo ratings yet
- Ador Incident FormDocument3 pagesAdor Incident FormJohn Rey LogrosaNo ratings yet
- 1 SCHOLARSHIP APPLICATION FORM - Long-Front-PageDocument1 page1 SCHOLARSHIP APPLICATION FORM - Long-Front-PageAngelyn SolisNo ratings yet
- 4PH Application Form Initial InfoDocument1 page4PH Application Form Initial InfoRizzle Domingo100% (1)
- PmrffsfsafDocument2 pagesPmrffsfsafManolito MacanasNo ratings yet
- Brma Application Form 2016Document2 pagesBrma Application Form 2016Joy WongNo ratings yet
- Fish R FormDocument1 pageFish R Formlibertygavarra1No ratings yet
- 2 Detailed Survey HH MembersDocument1 page2 Detailed Survey HH MembersGonzaga Merly CentinoNo ratings yet
- Item "A" - Reporting Person: Philippine National PoliceDocument5 pagesItem "A" - Reporting Person: Philippine National PoliceRomnese SantiagoNo ratings yet
- Item "A" - Reporting Person: Philippine National PoliceDocument5 pagesItem "A" - Reporting Person: Philippine National PoliceRomnese SantiagoNo ratings yet
- SSSForms Change RequestDocument9 pagesSSSForms Change RequestJessa BorreNo ratings yet
- Community Mapping (Region)Document40 pagesCommunity Mapping (Region)Ma Ann Jubay Limbaga-BasaloNo ratings yet
- PMRF - Final 2019Document2 pagesPMRF - Final 2019Silverghost Sun Dance Studio82% (17)
- Revised Incident Record Form BELITDocument2 pagesRevised Incident Record Form BELITJennie Amando100% (1)
- Ocfs 6025Document6 pagesOcfs 6025magdalenaNo ratings yet
- Incident Record Form (IRF)Document2 pagesIncident Record Form (IRF)nayr111312No ratings yet
- SSSForms Change RequestDocument6 pagesSSSForms Change Requestotaku3sthanNo ratings yet
- Afl Peaksun Enterprises and Export Corporation Pgaksun: 2F Peaksun Building 1505 Princeton St. Mandaluyong CityDocument4 pagesAfl Peaksun Enterprises and Export Corporation Pgaksun: 2F Peaksun Building 1505 Princeton St. Mandaluyong CityCarlo Dela CruzNo ratings yet
- Melgar Incident FormDocument3 pagesMelgar Incident FormJohn Rey LogrosaNo ratings yet
- Cenita Incident FormDocument3 pagesCenita Incident FormJohn Rey LogrosaNo ratings yet
- Local Government Unit: (If Married)Document1 pageLocal Government Unit: (If Married)Brix AguasonNo ratings yet
- CBW Housing ApplicationDocument14 pagesCBW Housing Application66bgxwvbgrNo ratings yet
- G1 Form +additional InfoDocument10 pagesG1 Form +additional InfoVERONICANo ratings yet
- Deped Region X Community Mapping Template: Name of Dependents MF Yes NoDocument2 pagesDeped Region X Community Mapping Template: Name of Dependents MF Yes NoChristopher SemillaNo ratings yet
- Ceniza Incident FormDocument3 pagesCeniza Incident FormJohn Rey LogrosaNo ratings yet
- Quezon City University Scholar Profile Form: Youth Development OfficeDocument10 pagesQuezon City University Scholar Profile Form: Youth Development OfficeLedNo ratings yet
- Information Form: Maldives Islamic BankDocument5 pagesInformation Form: Maldives Islamic BankyrafeeuNo ratings yet
- Soccer Registration Form: Player InformationDocument1 pageSoccer Registration Form: Player Informationsmit_jeromeNo ratings yet
- Client Information Form-Québec: FormtextDocument5 pagesClient Information Form-Québec: FormtextJhullian Frederick Val VergaraNo ratings yet
- RBI Form BDocument1 pageRBI Form BGerald Floro Funa100% (2)
- TFOE Members Application FormDocument4 pagesTFOE Members Application FormAndrei Dizon100% (1)
- Buyer Info Sheet 1Document1 pageBuyer Info Sheet 1api-636430593No ratings yet
- Application FormDocument4 pagesApplication FormKim BasicNo ratings yet
- IRF ACT FinalDocument3 pagesIRF ACT FinalHersheykris PimentelNo ratings yet
- Australian Unity Rebate FormDocument2 pagesAustralian Unity Rebate FormpmarteeneNo ratings yet
- Zim Social Security FormDocument3 pagesZim Social Security FormvincentkNo ratings yet
- Reminders:: UHC v.1 January 2020 Philhealth Identification Number (Pin)Document8 pagesReminders:: UHC v.1 January 2020 Philhealth Identification Number (Pin)YhelLappayNo ratings yet
- Personal Detail FormDocument1 pagePersonal Detail FormSalman SamiNo ratings yet
- (Please Send This Back To Corporate Accounts Division) : Application For Group Insurance PlanDocument2 pages(Please Send This Back To Corporate Accounts Division) : Application For Group Insurance PlanKristian Romeo NapiñasNo ratings yet
- Afpslai: Scholarship and Apprenticeship Program Application Form (For Ay 2024-2025)Document3 pagesAfpslai: Scholarship and Apprenticeship Program Application Form (For Ay 2024-2025)juvydanilaNo ratings yet
- Information Form - Individual 08.05.19Document5 pagesInformation Form - Individual 08.05.19hykleNo ratings yet
- PMRF 012020Document2 pagesPMRF 012020coolmer drugstore08No ratings yet
- Apartments Next DoorDocument14 pagesApartments Next DoorDennis GarrettNo ratings yet
- Philhealth Identification Number (Pin) Important Reminders:: PurposeDocument3 pagesPhilhealth Identification Number (Pin) Important Reminders:: PurposeMhelaril AnneNo ratings yet
- JMT HR - Form 002 v1 - Candidate Information FormDocument2 pagesJMT HR - Form 002 v1 - Candidate Information FormMaral Inocencio AltarNo ratings yet
- Personalrecord - Umidcard - Form Balanay, RenanDocument2 pagesPersonalrecord - Umidcard - Form Balanay, RenanErica Jane SarsaleNo ratings yet
- 60 Day Draft Biographical QuestionnaireDocument5 pages60 Day Draft Biographical QuestionnairekensmomkmNo ratings yet
- Date Accomplished (Signature Over Printed Name) : Evaluated/Processed byDocument2 pagesDate Accomplished (Signature Over Printed Name) : Evaluated/Processed byBello EvenNo ratings yet
- Irf ExampleDocument3 pagesIrf ExampleChristopher EstreraNo ratings yet
- Langcuyan Jonalyn Dacles: Please Carefully Read Instructions at The Back Before Accomplishing This FormDocument10 pagesLangcuyan Jonalyn Dacles: Please Carefully Read Instructions at The Back Before Accomplishing This FormPaHm Iglesias LeeNo ratings yet
- Employment Application: Eva Airways CorporationDocument7 pagesEmployment Application: Eva Airways CorporationbibikhaikhoiNo ratings yet
- Valencia & Roxas Income Taxation - IndividualsDocument12 pagesValencia & Roxas Income Taxation - IndividualsJonathan Junio100% (1)
- The Hindu HD Delhi Edition 21-05-2024Document18 pagesThe Hindu HD Delhi Edition 21-05-2024work.shellysNo ratings yet
- Class 11 Election and RepresentationDocument9 pagesClass 11 Election and Representationdoremonc80No ratings yet
- History - IIIDocument330 pagesHistory - IIIRajesh BazadNo ratings yet
- Build Then Sell System RecommendationDocument5 pagesBuild Then Sell System RecommendationAzS94100% (1)
- 4 Presentation FR Ogsimer ReducedDocument40 pages4 Presentation FR Ogsimer Reducedapi-170175919No ratings yet
- Joson v. Ombudsman, April 6, 2016 by LasacaDocument2 pagesJoson v. Ombudsman, April 6, 2016 by LasacaIan M. LasacaNo ratings yet
- Richard de ZoysaDocument6 pagesRichard de ZoysaThavam RatnaNo ratings yet
- Summary Chapter 8Document2 pagesSummary Chapter 8kwon zNo ratings yet
- RB Script LiobaDocument27 pagesRB Script Liobagbs040479No ratings yet
- 1st Summative Test in English Quarter 3Document5 pages1st Summative Test in English Quarter 3Romnick PadolinaNo ratings yet
- JJM Estimated CostDocument2 pagesJJM Estimated Costrajinder_hpiphNo ratings yet
- Accounting Ethics Chap 001Document19 pagesAccounting Ethics Chap 001AhmadAbushiNo ratings yet
- History Month 2022 Calendar of Activities: National Historical Commission of The PhilippinesDocument6 pagesHistory Month 2022 Calendar of Activities: National Historical Commission of The Philippinesalice ganarNo ratings yet
- Lawyer Guardian Ad-Litem in Matters of Child CustodyDocument3 pagesLawyer Guardian Ad-Litem in Matters of Child CustodyDougDanteNo ratings yet
- DecentralizationDocument5 pagesDecentralizationVivek SinhaNo ratings yet
- Article Viii - Judicial Department Section 1-8Document21 pagesArticle Viii - Judicial Department Section 1-8Arnel M. MapaNo ratings yet
- Supreme Court Judgement On Haj SubsidyDocument33 pagesSupreme Court Judgement On Haj SubsidyNDTV100% (1)
- Loc-Gov Week 12Document33 pagesLoc-Gov Week 12Rafael BernardoNo ratings yet
- Who Is Mustafiz PDFDocument3 pagesWho Is Mustafiz PDFPriyo YusufNo ratings yet
- Design, Cost Estimation and Development of Guidelines For The Construction of Rain Water Harvesting Pond.Document80 pagesDesign, Cost Estimation and Development of Guidelines For The Construction of Rain Water Harvesting Pond.Umer Malik100% (1)
- Tripartism and Social Dialogue-2Document32 pagesTripartism and Social Dialogue-2DOLE Region 6No ratings yet
- Annual Minutes TemplateDocument10 pagesAnnual Minutes TemplateAgostina MininiNo ratings yet
- List of Secretaries Registered Sec 241 Companies Act 2016Document185 pagesList of Secretaries Registered Sec 241 Companies Act 2016Abdul GhaffarNo ratings yet
- Local Voice April 2011Document24 pagesLocal Voice April 2011MoveUP, the Movement of United ProfessionalsNo ratings yet
- Trendline Breakout System by THZDocument10 pagesTrendline Breakout System by THZZukhruf AzzuhriNo ratings yet
- Sexual HarrasmentDocument13 pagesSexual HarrasmentFaisal SandhuNo ratings yet
- Oso Review Eze Collins OfomaDocument2 pagesOso Review Eze Collins OfomaCollins Ofoma EzeNo ratings yet
- 217 1 PDFDocument7 pages217 1 PDFcmissalNo ratings yet


















































































Download as pdf or txt
You might also like
- Andrea 2020 Federal Income Tax ReturnDocument11 pagesAndrea 2020 Federal Income Tax ReturnMorenita Pareles100% (1)
- India Maternity FormsDocument3 pagesIndia Maternity FormsJagadish ReddyNo ratings yet
- Insular Life Insurance FormDocument2 pagesInsular Life Insurance FormEarl Cortez0% (1)
- Personal Record: Filipino Iglesia Ni Cristo San Fernando City La UnionDocument3 pagesPersonal Record: Filipino Iglesia Ni Cristo San Fernando City La UnionManolito MacanasNo ratings yet
- Student Individual Inventory: Pangasinan Division Ii Bautista National High SchoolDocument2 pagesStudent Individual Inventory: Pangasinan Division Ii Bautista National High SchoolMichael JunioNo ratings yet
- UPDATED CIF Jul 2021 SAMPLE ONLYDocument2 pagesUPDATED CIF Jul 2021 SAMPLE ONLYChristine Anne PostradoNo ratings yet
- Degamo Incident FormDocument3 pagesDegamo Incident FormJohn Rey LogrosaNo ratings yet
- Ador Incident FormDocument3 pagesAdor Incident FormJohn Rey LogrosaNo ratings yet
- 1 SCHOLARSHIP APPLICATION FORM - Long-Front-PageDocument1 page1 SCHOLARSHIP APPLICATION FORM - Long-Front-PageAngelyn SolisNo ratings yet
- 4PH Application Form Initial InfoDocument1 page4PH Application Form Initial InfoRizzle Domingo100% (1)
- PmrffsfsafDocument2 pagesPmrffsfsafManolito MacanasNo ratings yet
- Brma Application Form 2016Document2 pagesBrma Application Form 2016Joy WongNo ratings yet
- Fish R FormDocument1 pageFish R Formlibertygavarra1No ratings yet
- 2 Detailed Survey HH MembersDocument1 page2 Detailed Survey HH MembersGonzaga Merly CentinoNo ratings yet
- Item "A" - Reporting Person: Philippine National PoliceDocument5 pagesItem "A" - Reporting Person: Philippine National PoliceRomnese SantiagoNo ratings yet
- Item "A" - Reporting Person: Philippine National PoliceDocument5 pagesItem "A" - Reporting Person: Philippine National PoliceRomnese SantiagoNo ratings yet
- SSSForms Change RequestDocument9 pagesSSSForms Change RequestJessa BorreNo ratings yet
- Community Mapping (Region)Document40 pagesCommunity Mapping (Region)Ma Ann Jubay Limbaga-BasaloNo ratings yet
- PMRF - Final 2019Document2 pagesPMRF - Final 2019Silverghost Sun Dance Studio82% (17)
- Revised Incident Record Form BELITDocument2 pagesRevised Incident Record Form BELITJennie Amando100% (1)
- Ocfs 6025Document6 pagesOcfs 6025magdalenaNo ratings yet
- Incident Record Form (IRF)Document2 pagesIncident Record Form (IRF)nayr111312No ratings yet
- SSSForms Change RequestDocument6 pagesSSSForms Change Requestotaku3sthanNo ratings yet
- Afl Peaksun Enterprises and Export Corporation Pgaksun: 2F Peaksun Building 1505 Princeton St. Mandaluyong CityDocument4 pagesAfl Peaksun Enterprises and Export Corporation Pgaksun: 2F Peaksun Building 1505 Princeton St. Mandaluyong CityCarlo Dela CruzNo ratings yet
- Melgar Incident FormDocument3 pagesMelgar Incident FormJohn Rey LogrosaNo ratings yet
- Cenita Incident FormDocument3 pagesCenita Incident FormJohn Rey LogrosaNo ratings yet
- Local Government Unit: (If Married)Document1 pageLocal Government Unit: (If Married)Brix AguasonNo ratings yet
- CBW Housing ApplicationDocument14 pagesCBW Housing Application66bgxwvbgrNo ratings yet
- G1 Form +additional InfoDocument10 pagesG1 Form +additional InfoVERONICANo ratings yet
- Deped Region X Community Mapping Template: Name of Dependents MF Yes NoDocument2 pagesDeped Region X Community Mapping Template: Name of Dependents MF Yes NoChristopher SemillaNo ratings yet
- Ceniza Incident FormDocument3 pagesCeniza Incident FormJohn Rey LogrosaNo ratings yet
- Quezon City University Scholar Profile Form: Youth Development OfficeDocument10 pagesQuezon City University Scholar Profile Form: Youth Development OfficeLedNo ratings yet
- Information Form: Maldives Islamic BankDocument5 pagesInformation Form: Maldives Islamic BankyrafeeuNo ratings yet
- Soccer Registration Form: Player InformationDocument1 pageSoccer Registration Form: Player Informationsmit_jeromeNo ratings yet
- Client Information Form-Québec: FormtextDocument5 pagesClient Information Form-Québec: FormtextJhullian Frederick Val VergaraNo ratings yet
- RBI Form BDocument1 pageRBI Form BGerald Floro Funa100% (2)
- TFOE Members Application FormDocument4 pagesTFOE Members Application FormAndrei Dizon100% (1)
- Buyer Info Sheet 1Document1 pageBuyer Info Sheet 1api-636430593No ratings yet
- Application FormDocument4 pagesApplication FormKim BasicNo ratings yet
- IRF ACT FinalDocument3 pagesIRF ACT FinalHersheykris PimentelNo ratings yet
- Australian Unity Rebate FormDocument2 pagesAustralian Unity Rebate FormpmarteeneNo ratings yet
- Zim Social Security FormDocument3 pagesZim Social Security FormvincentkNo ratings yet
- Reminders:: UHC v.1 January 2020 Philhealth Identification Number (Pin)Document8 pagesReminders:: UHC v.1 January 2020 Philhealth Identification Number (Pin)YhelLappayNo ratings yet
- Personal Detail FormDocument1 pagePersonal Detail FormSalman SamiNo ratings yet
- (Please Send This Back To Corporate Accounts Division) : Application For Group Insurance PlanDocument2 pages(Please Send This Back To Corporate Accounts Division) : Application For Group Insurance PlanKristian Romeo NapiñasNo ratings yet
- Afpslai: Scholarship and Apprenticeship Program Application Form (For Ay 2024-2025)Document3 pagesAfpslai: Scholarship and Apprenticeship Program Application Form (For Ay 2024-2025)juvydanilaNo ratings yet
- Information Form - Individual 08.05.19Document5 pagesInformation Form - Individual 08.05.19hykleNo ratings yet
- PMRF 012020Document2 pagesPMRF 012020coolmer drugstore08No ratings yet
- Apartments Next DoorDocument14 pagesApartments Next DoorDennis GarrettNo ratings yet
- Philhealth Identification Number (Pin) Important Reminders:: PurposeDocument3 pagesPhilhealth Identification Number (Pin) Important Reminders:: PurposeMhelaril AnneNo ratings yet
- JMT HR - Form 002 v1 - Candidate Information FormDocument2 pagesJMT HR - Form 002 v1 - Candidate Information FormMaral Inocencio AltarNo ratings yet
- Personalrecord - Umidcard - Form Balanay, RenanDocument2 pagesPersonalrecord - Umidcard - Form Balanay, RenanErica Jane SarsaleNo ratings yet
- 60 Day Draft Biographical QuestionnaireDocument5 pages60 Day Draft Biographical QuestionnairekensmomkmNo ratings yet
- Date Accomplished (Signature Over Printed Name) : Evaluated/Processed byDocument2 pagesDate Accomplished (Signature Over Printed Name) : Evaluated/Processed byBello EvenNo ratings yet
- Irf ExampleDocument3 pagesIrf ExampleChristopher EstreraNo ratings yet
- Langcuyan Jonalyn Dacles: Please Carefully Read Instructions at The Back Before Accomplishing This FormDocument10 pagesLangcuyan Jonalyn Dacles: Please Carefully Read Instructions at The Back Before Accomplishing This FormPaHm Iglesias LeeNo ratings yet
- Employment Application: Eva Airways CorporationDocument7 pagesEmployment Application: Eva Airways CorporationbibikhaikhoiNo ratings yet
- Valencia & Roxas Income Taxation - IndividualsDocument12 pagesValencia & Roxas Income Taxation - IndividualsJonathan Junio100% (1)
- The Hindu HD Delhi Edition 21-05-2024Document18 pagesThe Hindu HD Delhi Edition 21-05-2024work.shellysNo ratings yet
- Class 11 Election and RepresentationDocument9 pagesClass 11 Election and Representationdoremonc80No ratings yet
- History - IIIDocument330 pagesHistory - IIIRajesh BazadNo ratings yet
- Build Then Sell System RecommendationDocument5 pagesBuild Then Sell System RecommendationAzS94100% (1)
- 4 Presentation FR Ogsimer ReducedDocument40 pages4 Presentation FR Ogsimer Reducedapi-170175919No ratings yet
- Joson v. Ombudsman, April 6, 2016 by LasacaDocument2 pagesJoson v. Ombudsman, April 6, 2016 by LasacaIan M. LasacaNo ratings yet
- Richard de ZoysaDocument6 pagesRichard de ZoysaThavam RatnaNo ratings yet
- Summary Chapter 8Document2 pagesSummary Chapter 8kwon zNo ratings yet
- RB Script LiobaDocument27 pagesRB Script Liobagbs040479No ratings yet
- 1st Summative Test in English Quarter 3Document5 pages1st Summative Test in English Quarter 3Romnick PadolinaNo ratings yet
- JJM Estimated CostDocument2 pagesJJM Estimated Costrajinder_hpiphNo ratings yet
- Accounting Ethics Chap 001Document19 pagesAccounting Ethics Chap 001AhmadAbushiNo ratings yet
- History Month 2022 Calendar of Activities: National Historical Commission of The PhilippinesDocument6 pagesHistory Month 2022 Calendar of Activities: National Historical Commission of The Philippinesalice ganarNo ratings yet
- Lawyer Guardian Ad-Litem in Matters of Child CustodyDocument3 pagesLawyer Guardian Ad-Litem in Matters of Child CustodyDougDanteNo ratings yet
- DecentralizationDocument5 pagesDecentralizationVivek SinhaNo ratings yet
- Article Viii - Judicial Department Section 1-8Document21 pagesArticle Viii - Judicial Department Section 1-8Arnel M. MapaNo ratings yet
- Supreme Court Judgement On Haj SubsidyDocument33 pagesSupreme Court Judgement On Haj SubsidyNDTV100% (1)
- Loc-Gov Week 12Document33 pagesLoc-Gov Week 12Rafael BernardoNo ratings yet
- Who Is Mustafiz PDFDocument3 pagesWho Is Mustafiz PDFPriyo YusufNo ratings yet
- Design, Cost Estimation and Development of Guidelines For The Construction of Rain Water Harvesting Pond.Document80 pagesDesign, Cost Estimation and Development of Guidelines For The Construction of Rain Water Harvesting Pond.Umer Malik100% (1)
- Tripartism and Social Dialogue-2Document32 pagesTripartism and Social Dialogue-2DOLE Region 6No ratings yet
- Annual Minutes TemplateDocument10 pagesAnnual Minutes TemplateAgostina MininiNo ratings yet
- List of Secretaries Registered Sec 241 Companies Act 2016Document185 pagesList of Secretaries Registered Sec 241 Companies Act 2016Abdul GhaffarNo ratings yet
- Local Voice April 2011Document24 pagesLocal Voice April 2011MoveUP, the Movement of United ProfessionalsNo ratings yet
- Trendline Breakout System by THZDocument10 pagesTrendline Breakout System by THZZukhruf AzzuhriNo ratings yet
- Sexual HarrasmentDocument13 pagesSexual HarrasmentFaisal SandhuNo ratings yet
- Oso Review Eze Collins OfomaDocument2 pagesOso Review Eze Collins OfomaCollins Ofoma EzeNo ratings yet
- 217 1 PDFDocument7 pages217 1 PDFcmissalNo ratings yet