
Clinical Notes 42017
Clinical Notes 42017
You might also like
- GNC SSN Past Paper 18-1Document32 pagesGNC SSN Past Paper 18-1Fan Eli100% (30)
- NCP Failure To Thrive.Document14 pagesNCP Failure To Thrive.Yashoda Satpute100% (3)
- Impaired Verbal CommunicationDocument1 pageImpaired Verbal Communicationdana100% (3)
- Bibliography For IsmDocument6 pagesBibliography For Ismapi-736923280No ratings yet
- Babcock&perea Evidence PaperDocument9 pagesBabcock&perea Evidence Paperapi-238107777No ratings yet
- Awareness of Text Neck Syndrome in Young-Adult Pop PDFDocument5 pagesAwareness of Text Neck Syndrome in Young-Adult Pop PDFBarkha FulwaniNo ratings yet
- Use of Elastic Bandage Associated With Speech Therapy in The Control of Sialorrhea (Hypersalivation)Document9 pagesUse of Elastic Bandage Associated With Speech Therapy in The Control of Sialorrhea (Hypersalivation)MayzaNo ratings yet
- Reducing Dental Anxiety in Pediatric PatientsDocument6 pagesReducing Dental Anxiety in Pediatric Patientsapi-613602373No ratings yet
- Addition of Kinesio Taping of The Orbicularis Oris Muscles To Speech Therapy Rapidly Improves Drooling in Children With Neurological Disorders, 2019Document7 pagesAddition of Kinesio Taping of The Orbicularis Oris Muscles To Speech Therapy Rapidly Improves Drooling in Children With Neurological Disorders, 2019Maria Del Mar Marulanda GrizalesNo ratings yet
- Long Term Effects of The Palatal Plate Therapy For The Orofacial Regulation in Children With Down SyndromeDocument6 pagesLong Term Effects of The Palatal Plate Therapy For The Orofacial Regulation in Children With Down Syndromenatashanascimento.odontoNo ratings yet
- Motivation and Compliance With Intraoral ElasticsDocument7 pagesMotivation and Compliance With Intraoral ElasticsValery V JaureguiNo ratings yet
- Transcutaneous Electrical Nerve Stimulation in Speech Therapy Rehabilitation ofDocument13 pagesTranscutaneous Electrical Nerve Stimulation in Speech Therapy Rehabilitation ofGabriel DefazNo ratings yet
- Dental Caries: Treatment of Deep CariesDocument2 pagesDental Caries: Treatment of Deep CariesKingkan HongyonNo ratings yet
- Aphasia TherapyDocument294 pagesAphasia Therapynagarjuna.clpsyNo ratings yet
- Drwouling ManagementDocument7 pagesDrwouling Managementsanober AkramNo ratings yet
- BPJ Vol 10 No 2 P 959-967Document9 pagesBPJ Vol 10 No 2 P 959-967ilomurtalaNo ratings yet
- JAMA OphthalmolDocument15 pagesJAMA OphthalmolAyen AlingNo ratings yet
- Research ProposalDocument2 pagesResearch ProposalM ClementsNo ratings yet
- Core Level 3: HPE 353W Research PaperDocument10 pagesCore Level 3: HPE 353W Research PaperAnonymous XMU2EoqxYNo ratings yet
- P. Siaperas Teacch Autism 10 (4) 2006Document14 pagesP. Siaperas Teacch Autism 10 (4) 2006Rania ChioureaNo ratings yet
- Concentration Level 3: HPE 353W Research PaperDocument10 pagesConcentration Level 3: HPE 353W Research PaperAnonymous XMU2EoqxYNo ratings yet
- Oral Appliance Therapy For Obstructive Sleep Apnea63, Number 6, May 2001, 1294-1295Document3 pagesOral Appliance Therapy For Obstructive Sleep Apnea63, Number 6, May 2001, 1294-1295api-22211213No ratings yet
- Intensive Speech Therapy in Ugandan Patients With Cleft (Lip And) Palate ADocument12 pagesIntensive Speech Therapy in Ugandan Patients With Cleft (Lip And) Palate Acvdk8dc8sbNo ratings yet
- Treatments For Infantile Postural AsymmetryDocument7 pagesTreatments For Infantile Postural AsymmetryraquelbibiNo ratings yet
- JR 1 Blok 15Document21 pagesJR 1 Blok 15Audio TechnicaNo ratings yet
- Solis Pazmino2020Document6 pagesSolis Pazmino2020Fábio LopesNo ratings yet
- Can A Flavored Spray (Pill Glide) Help Children Swallow Their Medicines? A Pilot StudyDocument11 pagesCan A Flavored Spray (Pill Glide) Help Children Swallow Their Medicines? A Pilot StudyUmar AliNo ratings yet
- Effects of Palatal Crib and Bonded Spurs in Early Treatment of Anterior Open Bite: A Prospective Randomized Clinical StudyDocument6 pagesEffects of Palatal Crib and Bonded Spurs in Early Treatment of Anterior Open Bite: A Prospective Randomized Clinical StudyShreyaNo ratings yet
- Does The Development and Use of Modern Disposable Diape - 2021 - Journal of PediDocument9 pagesDoes The Development and Use of Modern Disposable Diape - 2021 - Journal of PediDamaradyaNo ratings yet
- Fernandes 2012Document5 pagesFernandes 2012Andreea Popovici - IşfanNo ratings yet
- Hand Rehab FacilityDocument5 pagesHand Rehab FacilityManik MishraNo ratings yet
- Effects of Palatal Crib and Bonded Spurs in Early Treatment of Anterior Open BiteDocument6 pagesEffects of Palatal Crib and Bonded Spurs in Early Treatment of Anterior Open BiteflorinNo ratings yet
- A Unique Habit-Breaking Therapy: An Innovative Approach (PKS Approach)Document3 pagesA Unique Habit-Breaking Therapy: An Innovative Approach (PKS Approach)IJAR JOURNALNo ratings yet
- Clinical Linguistics & Phonetics: Inger Lundeborg Hammarström, Rose-Marie Svensson & Karin MyrbergDocument15 pagesClinical Linguistics & Phonetics: Inger Lundeborg Hammarström, Rose-Marie Svensson & Karin MyrbergRafael AlvesNo ratings yet
- J Jfludis 2021 105843Document21 pagesJ Jfludis 2021 105843ANDREA MIRANDA MEZA GARNICANo ratings yet
- Journal Critique 1Document4 pagesJournal Critique 1Marianne PasciolcoNo ratings yet
- 2176 9451 Dpjo 22 03 00079Document10 pages2176 9451 Dpjo 22 03 00079Maha BadraNo ratings yet
- Facial Soft TisuesDocument6 pagesFacial Soft TisuesMoni Garcia SantosNo ratings yet
- The Effects of Oral Motor Exercises On Diadochokinetic RatesDocument23 pagesThe Effects of Oral Motor Exercises On Diadochokinetic RatesNicole GrayNo ratings yet
- The Presence of Altered Craniocervical Posture and Mobility in Smartphone-Addicted Teenagers With Temporomandibular DisordersDocument8 pagesThe Presence of Altered Craniocervical Posture and Mobility in Smartphone-Addicted Teenagers With Temporomandibular DisordersJoão MaiaNo ratings yet
- Deformidad Craneal y Desarrollo MotorDocument9 pagesDeformidad Craneal y Desarrollo MotordianareinaNo ratings yet
- The Effectiveness of An Oral Sensorimotor Stimulation Protocol For The Early Achievement of Exclusive Oral Feeding in Premature Infants A RandomizedDocument14 pagesThe Effectiveness of An Oral Sensorimotor Stimulation Protocol For The Early Achievement of Exclusive Oral Feeding in Premature Infants A RandomizedJUAN CARLOSNo ratings yet
- 10 Intl J Lang Comm Disor - 2019 - Park - Effect of Effortful Swallowing Training On Tongue Strength and OropharyngealDocument6 pages10 Intl J Lang Comm Disor - 2019 - Park - Effect of Effortful Swallowing Training On Tongue Strength and OropharyngealAndressa AraújoNo ratings yet
- Armin Bidarian Moniri PDFDocument74 pagesArmin Bidarian Moniri PDFManuela LourençoNo ratings yet
- Audiologi 1Document12 pagesAudiologi 1Andy Caroll JuniorsNo ratings yet
- Literature Review DraftDocument6 pagesLiterature Review Draftapi-520874386No ratings yet
- 2016, Oliveira Et Al, PEED, Validation Brasilian Version The Voice Disability Coping Questionnaire, J Voice Art TeseDocument9 pages2016, Oliveira Et Al, PEED, Validation Brasilian Version The Voice Disability Coping Questionnaire, J Voice Art TeseCarol PaesNo ratings yet
- Spinal in ChildernDocument9 pagesSpinal in ChildernKhairani FirdausNo ratings yet
- 1 Bordino L Zanj J Et Al 2022 Pediatric Flexible Endoscopic Evaluation of SwallowingDocument7 pages1 Bordino L Zanj J Et Al 2022 Pediatric Flexible Endoscopic Evaluation of Swallowingfranciscojavier.hernandez.eNo ratings yet
- The Effectiveness of Massage For Children With Cerebral Palsy: A Systematic ReviewDocument11 pagesThe Effectiveness of Massage For Children With Cerebral Palsy: A Systematic ReviewAl MukaramahNo ratings yet
- JOHOE - Volume 5 - Issue 1 - Pages 13-16Document4 pagesJOHOE - Volume 5 - Issue 1 - Pages 13-16Tô ThuỷNo ratings yet
- Elastic Therapeutic Taping in Paediatrics PDFDocument12 pagesElastic Therapeutic Taping in Paediatrics PDFAnonymous r0hChg4mzNo ratings yet
- A 3-Year Patient-Centred Follow-Up of 516 Consecutively Treated Orthognathic Surgery PatientsDocument7 pagesA 3-Year Patient-Centred Follow-Up of 516 Consecutively Treated Orthognathic Surgery Patientsodontologia uvNo ratings yet
- Final Revishion EssayDocument9 pagesFinal Revishion Essayapi-743811249No ratings yet
- Journal Article Review AssessmentDocument4 pagesJournal Article Review Assessmentapi-711088465No ratings yet
- Disfunción Masticatoria en Síndrome de DownDocument7 pagesDisfunción Masticatoria en Síndrome de DownLuis Leonardo Cepeda GuíñezNo ratings yet
- The Challenge of Child Management During Dental Care: Use of Nonpharmacological ApproachesDocument2 pagesThe Challenge of Child Management During Dental Care: Use of Nonpharmacological ApproachesAndres RamosNo ratings yet
- McManus PDFDocument6 pagesMcManus PDFilona ilincaNo ratings yet
- Longitudinal Study of Growth of Children With Unilateral Cleft-Lip Palate From Birth To Two Years of AgeDocument7 pagesLongitudinal Study of Growth of Children With Unilateral Cleft-Lip Palate From Birth To Two Years of AgeCarlos CastañedaNo ratings yet
- Pediatrics & TherapeuticsDocument7 pagesPediatrics & TherapeuticsAmit PasiNo ratings yet
- Abhilash Ghae (Maslp 2) I, Research Proposal, 2020 2022Document27 pagesAbhilash Ghae (Maslp 2) I, Research Proposal, 2020 2022Abhilash GhadeiNo ratings yet
- Sleep Disorders in Pediatric Dentistry: Clinical Guide on Diagnosis and ManagementFrom EverandSleep Disorders in Pediatric Dentistry: Clinical Guide on Diagnosis and ManagementEdmund LiemNo ratings yet
- Endoscopy in Pediatric Inflammatory Bowel DiseaseFrom EverandEndoscopy in Pediatric Inflammatory Bowel DiseaseLuigi Dall'OglioNo ratings yet
- Studies Into Mechanisms Behind Kinesio TapingDocument2 pagesStudies Into Mechanisms Behind Kinesio TapingchristinaNo ratings yet
- Ataxia Coordinative Physiotherapy BroetzDocument12 pagesAtaxia Coordinative Physiotherapy BroetzchristinaNo ratings yet
- Skin Movement in Truck RotationDocument1 pageSkin Movement in Truck RotationchristinaNo ratings yet
- Classroom Activities For Understanding Duchenne: English SpanishDocument6 pagesClassroom Activities For Understanding Duchenne: English SpanishchristinaNo ratings yet
- Poster SOSORT 2014 Elastic Therapeutic TapeDocument1 pagePoster SOSORT 2014 Elastic Therapeutic TapechristinaNo ratings yet
- Organ Zones: Thanking AEVNM For Use of ImageDocument1 pageOrgan Zones: Thanking AEVNM For Use of ImagechristinaNo ratings yet
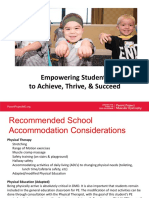
- Empowering Students To Achieve, Thrive, & SucceedDocument6 pagesEmpowering Students To Achieve, Thrive, & SucceedchristinaNo ratings yet
- Clinical Notes 2 ETT-Ped Taping Pre-TermDocument3 pagesClinical Notes 2 ETT-Ped Taping Pre-TermchristinaNo ratings yet
- Muscle Strength and Physical FitnessDocument20 pagesMuscle Strength and Physical FitnesschristinaNo ratings yet
- What Is Pediatric Heel Pain?Document2 pagesWhat Is Pediatric Heel Pain?christinaNo ratings yet
- Normative Reference Values SPECIFIC TESTSDocument113 pagesNormative Reference Values SPECIFIC TESTSchristinaNo ratings yet
- BLS AlgorithmDocument9 pagesBLS AlgorithmDr VJ GeorgeNo ratings yet
- ZDocument5 pagesZBiljana Custovic RadicicNo ratings yet
- Drug Product PerformanceDocument1 pageDrug Product PerformanceLuna Abigail TorresNo ratings yet
- Balanti An ES School Contingency Plan FINALDocument54 pagesBalanti An ES School Contingency Plan FINALCathyren Capizonda TevesNo ratings yet
- Active Assisted and Passive Movement in TreatmentDocument4 pagesActive Assisted and Passive Movement in TreatmentshravaniNo ratings yet
- What Is ThalassemiaDocument2 pagesWhat Is ThalassemiaFatima Azzahra Khairul AnuarNo ratings yet
- What Is Acrophobia?: Computer-Simulated Phobia PTSD Zoophobia Acrophobia U.S. NavyDocument1 pageWhat Is Acrophobia?: Computer-Simulated Phobia PTSD Zoophobia Acrophobia U.S. NavyE. LópezNo ratings yet
- Module 1Document9 pagesModule 1ALEXANDER BRYAN GONo ratings yet
- CMC-Time Table 1st Year MBBS 150620Document1 pageCMC-Time Table 1st Year MBBS 150620KhanNo ratings yet
- Elsevier - Anaesthesiology Clinics - Vol.26, Issues 1 - Obstetric Anesthesia (2008) PDFDocument230 pagesElsevier - Anaesthesiology Clinics - Vol.26, Issues 1 - Obstetric Anesthesia (2008) PDFMila KarmilaNo ratings yet
- Division 3: Trauma EmergenciesDocument48 pagesDivision 3: Trauma EmergenciesmadhuNo ratings yet
- Indra Diagnostic Centre & Blood Bank: Department of UltrasoundDocument1 pageIndra Diagnostic Centre & Blood Bank: Department of Ultrasoundpassword123resetNo ratings yet
- PROTOZOANS (Blood and Tissue Flagellates)Document4 pagesPROTOZOANS (Blood and Tissue Flagellates)Eunice AndradeNo ratings yet
- CGHS Rate ListDocument39 pagesCGHS Rate ListAniruddha KoparkarNo ratings yet
- Mpu3312 Assignment-May22Document6 pagesMpu3312 Assignment-May22kentbiibibibiNo ratings yet
- CLINPHARM Lab Act 1Document8 pagesCLINPHARM Lab Act 1ezzaNo ratings yet
- Fitness Plan: Luas Wilaya 34 508 542 100.00% 244 48.00 44.00 9.00 11.00 22.00 0.00Document2 pagesFitness Plan: Luas Wilaya 34 508 542 100.00% 244 48.00 44.00 9.00 11.00 22.00 0.00Acep DediNo ratings yet
- 1 s2.0 S0735109786800183 Main PDFDocument252 pages1 s2.0 S0735109786800183 Main PDFdangthieuhoiNo ratings yet
- Aiims 2010 November 2010 DentalDocument62 pagesAiims 2010 November 2010 DentalMrunal Doiphode100% (1)
- Fundamentals of Pharmacology 8th Edition Bullock Test BankDocument9 pagesFundamentals of Pharmacology 8th Edition Bullock Test Bankdorissamuelqpnrrz100% (33)
- A Screening Instrument For Autism Months of Age: A Follow-Up StudyDocument9 pagesA Screening Instrument For Autism Months of Age: A Follow-Up StudyJose Alonso Aguilar ValeraNo ratings yet
- Tinea Capitis Dermoscopy and Calcium Fluorescent Microscopy As Highly Efficient and Precise Diagnostic Tools - Xiao2020Document4 pagesTinea Capitis Dermoscopy and Calcium Fluorescent Microscopy As Highly Efficient and Precise Diagnostic Tools - Xiao2020KhairunNisaNo ratings yet
- BURNDocument5 pagesBURNLara TechiesNo ratings yet
- OB C. 15 Study GuideDocument10 pagesOB C. 15 Study GuidePaige Nicole GauthreauxNo ratings yet
- Presentation BP MonitorDocument7 pagesPresentation BP MonitorImwaniki21No ratings yet
- Fisa Evaluare DurereDocument2 pagesFisa Evaluare DurerecristianNo ratings yet
- Unspoken Needs KrisnamalDocument26 pagesUnspoken Needs Krisnamalmalaysianhospicecouncil6240No ratings yet



































































































Download as pdf or txt
You might also like
- GNC SSN Past Paper 18-1Document32 pagesGNC SSN Past Paper 18-1Fan Eli100% (30)
- NCP Failure To Thrive.Document14 pagesNCP Failure To Thrive.Yashoda Satpute100% (3)
- Impaired Verbal CommunicationDocument1 pageImpaired Verbal Communicationdana100% (3)
- Bibliography For IsmDocument6 pagesBibliography For Ismapi-736923280No ratings yet
- Babcock&perea Evidence PaperDocument9 pagesBabcock&perea Evidence Paperapi-238107777No ratings yet
- Awareness of Text Neck Syndrome in Young-Adult Pop PDFDocument5 pagesAwareness of Text Neck Syndrome in Young-Adult Pop PDFBarkha FulwaniNo ratings yet
- Use of Elastic Bandage Associated With Speech Therapy in The Control of Sialorrhea (Hypersalivation)Document9 pagesUse of Elastic Bandage Associated With Speech Therapy in The Control of Sialorrhea (Hypersalivation)MayzaNo ratings yet
- Reducing Dental Anxiety in Pediatric PatientsDocument6 pagesReducing Dental Anxiety in Pediatric Patientsapi-613602373No ratings yet
- Addition of Kinesio Taping of The Orbicularis Oris Muscles To Speech Therapy Rapidly Improves Drooling in Children With Neurological Disorders, 2019Document7 pagesAddition of Kinesio Taping of The Orbicularis Oris Muscles To Speech Therapy Rapidly Improves Drooling in Children With Neurological Disorders, 2019Maria Del Mar Marulanda GrizalesNo ratings yet
- Long Term Effects of The Palatal Plate Therapy For The Orofacial Regulation in Children With Down SyndromeDocument6 pagesLong Term Effects of The Palatal Plate Therapy For The Orofacial Regulation in Children With Down Syndromenatashanascimento.odontoNo ratings yet
- Motivation and Compliance With Intraoral ElasticsDocument7 pagesMotivation and Compliance With Intraoral ElasticsValery V JaureguiNo ratings yet
- Transcutaneous Electrical Nerve Stimulation in Speech Therapy Rehabilitation ofDocument13 pagesTranscutaneous Electrical Nerve Stimulation in Speech Therapy Rehabilitation ofGabriel DefazNo ratings yet
- Dental Caries: Treatment of Deep CariesDocument2 pagesDental Caries: Treatment of Deep CariesKingkan HongyonNo ratings yet
- Aphasia TherapyDocument294 pagesAphasia Therapynagarjuna.clpsyNo ratings yet
- Drwouling ManagementDocument7 pagesDrwouling Managementsanober AkramNo ratings yet
- BPJ Vol 10 No 2 P 959-967Document9 pagesBPJ Vol 10 No 2 P 959-967ilomurtalaNo ratings yet
- JAMA OphthalmolDocument15 pagesJAMA OphthalmolAyen AlingNo ratings yet
- Research ProposalDocument2 pagesResearch ProposalM ClementsNo ratings yet
- Core Level 3: HPE 353W Research PaperDocument10 pagesCore Level 3: HPE 353W Research PaperAnonymous XMU2EoqxYNo ratings yet
- P. Siaperas Teacch Autism 10 (4) 2006Document14 pagesP. Siaperas Teacch Autism 10 (4) 2006Rania ChioureaNo ratings yet
- Concentration Level 3: HPE 353W Research PaperDocument10 pagesConcentration Level 3: HPE 353W Research PaperAnonymous XMU2EoqxYNo ratings yet
- Oral Appliance Therapy For Obstructive Sleep Apnea63, Number 6, May 2001, 1294-1295Document3 pagesOral Appliance Therapy For Obstructive Sleep Apnea63, Number 6, May 2001, 1294-1295api-22211213No ratings yet
- Intensive Speech Therapy in Ugandan Patients With Cleft (Lip And) Palate ADocument12 pagesIntensive Speech Therapy in Ugandan Patients With Cleft (Lip And) Palate Acvdk8dc8sbNo ratings yet
- Treatments For Infantile Postural AsymmetryDocument7 pagesTreatments For Infantile Postural AsymmetryraquelbibiNo ratings yet
- JR 1 Blok 15Document21 pagesJR 1 Blok 15Audio TechnicaNo ratings yet
- Solis Pazmino2020Document6 pagesSolis Pazmino2020Fábio LopesNo ratings yet
- Can A Flavored Spray (Pill Glide) Help Children Swallow Their Medicines? A Pilot StudyDocument11 pagesCan A Flavored Spray (Pill Glide) Help Children Swallow Their Medicines? A Pilot StudyUmar AliNo ratings yet
- Effects of Palatal Crib and Bonded Spurs in Early Treatment of Anterior Open Bite: A Prospective Randomized Clinical StudyDocument6 pagesEffects of Palatal Crib and Bonded Spurs in Early Treatment of Anterior Open Bite: A Prospective Randomized Clinical StudyShreyaNo ratings yet
- Does The Development and Use of Modern Disposable Diape - 2021 - Journal of PediDocument9 pagesDoes The Development and Use of Modern Disposable Diape - 2021 - Journal of PediDamaradyaNo ratings yet
- Fernandes 2012Document5 pagesFernandes 2012Andreea Popovici - IşfanNo ratings yet
- Hand Rehab FacilityDocument5 pagesHand Rehab FacilityManik MishraNo ratings yet
- Effects of Palatal Crib and Bonded Spurs in Early Treatment of Anterior Open BiteDocument6 pagesEffects of Palatal Crib and Bonded Spurs in Early Treatment of Anterior Open BiteflorinNo ratings yet
- A Unique Habit-Breaking Therapy: An Innovative Approach (PKS Approach)Document3 pagesA Unique Habit-Breaking Therapy: An Innovative Approach (PKS Approach)IJAR JOURNALNo ratings yet
- Clinical Linguistics & Phonetics: Inger Lundeborg Hammarström, Rose-Marie Svensson & Karin MyrbergDocument15 pagesClinical Linguistics & Phonetics: Inger Lundeborg Hammarström, Rose-Marie Svensson & Karin MyrbergRafael AlvesNo ratings yet
- J Jfludis 2021 105843Document21 pagesJ Jfludis 2021 105843ANDREA MIRANDA MEZA GARNICANo ratings yet
- Journal Critique 1Document4 pagesJournal Critique 1Marianne PasciolcoNo ratings yet
- 2176 9451 Dpjo 22 03 00079Document10 pages2176 9451 Dpjo 22 03 00079Maha BadraNo ratings yet
- Facial Soft TisuesDocument6 pagesFacial Soft TisuesMoni Garcia SantosNo ratings yet
- The Effects of Oral Motor Exercises On Diadochokinetic RatesDocument23 pagesThe Effects of Oral Motor Exercises On Diadochokinetic RatesNicole GrayNo ratings yet
- The Presence of Altered Craniocervical Posture and Mobility in Smartphone-Addicted Teenagers With Temporomandibular DisordersDocument8 pagesThe Presence of Altered Craniocervical Posture and Mobility in Smartphone-Addicted Teenagers With Temporomandibular DisordersJoão MaiaNo ratings yet
- Deformidad Craneal y Desarrollo MotorDocument9 pagesDeformidad Craneal y Desarrollo MotordianareinaNo ratings yet
- The Effectiveness of An Oral Sensorimotor Stimulation Protocol For The Early Achievement of Exclusive Oral Feeding in Premature Infants A RandomizedDocument14 pagesThe Effectiveness of An Oral Sensorimotor Stimulation Protocol For The Early Achievement of Exclusive Oral Feeding in Premature Infants A RandomizedJUAN CARLOSNo ratings yet
- 10 Intl J Lang Comm Disor - 2019 - Park - Effect of Effortful Swallowing Training On Tongue Strength and OropharyngealDocument6 pages10 Intl J Lang Comm Disor - 2019 - Park - Effect of Effortful Swallowing Training On Tongue Strength and OropharyngealAndressa AraújoNo ratings yet
- Armin Bidarian Moniri PDFDocument74 pagesArmin Bidarian Moniri PDFManuela LourençoNo ratings yet
- Audiologi 1Document12 pagesAudiologi 1Andy Caroll JuniorsNo ratings yet
- Literature Review DraftDocument6 pagesLiterature Review Draftapi-520874386No ratings yet
- 2016, Oliveira Et Al, PEED, Validation Brasilian Version The Voice Disability Coping Questionnaire, J Voice Art TeseDocument9 pages2016, Oliveira Et Al, PEED, Validation Brasilian Version The Voice Disability Coping Questionnaire, J Voice Art TeseCarol PaesNo ratings yet
- Spinal in ChildernDocument9 pagesSpinal in ChildernKhairani FirdausNo ratings yet
- 1 Bordino L Zanj J Et Al 2022 Pediatric Flexible Endoscopic Evaluation of SwallowingDocument7 pages1 Bordino L Zanj J Et Al 2022 Pediatric Flexible Endoscopic Evaluation of Swallowingfranciscojavier.hernandez.eNo ratings yet
- The Effectiveness of Massage For Children With Cerebral Palsy: A Systematic ReviewDocument11 pagesThe Effectiveness of Massage For Children With Cerebral Palsy: A Systematic ReviewAl MukaramahNo ratings yet
- JOHOE - Volume 5 - Issue 1 - Pages 13-16Document4 pagesJOHOE - Volume 5 - Issue 1 - Pages 13-16Tô ThuỷNo ratings yet
- Elastic Therapeutic Taping in Paediatrics PDFDocument12 pagesElastic Therapeutic Taping in Paediatrics PDFAnonymous r0hChg4mzNo ratings yet
- A 3-Year Patient-Centred Follow-Up of 516 Consecutively Treated Orthognathic Surgery PatientsDocument7 pagesA 3-Year Patient-Centred Follow-Up of 516 Consecutively Treated Orthognathic Surgery Patientsodontologia uvNo ratings yet
- Final Revishion EssayDocument9 pagesFinal Revishion Essayapi-743811249No ratings yet
- Journal Article Review AssessmentDocument4 pagesJournal Article Review Assessmentapi-711088465No ratings yet
- Disfunción Masticatoria en Síndrome de DownDocument7 pagesDisfunción Masticatoria en Síndrome de DownLuis Leonardo Cepeda GuíñezNo ratings yet
- The Challenge of Child Management During Dental Care: Use of Nonpharmacological ApproachesDocument2 pagesThe Challenge of Child Management During Dental Care: Use of Nonpharmacological ApproachesAndres RamosNo ratings yet
- McManus PDFDocument6 pagesMcManus PDFilona ilincaNo ratings yet
- Longitudinal Study of Growth of Children With Unilateral Cleft-Lip Palate From Birth To Two Years of AgeDocument7 pagesLongitudinal Study of Growth of Children With Unilateral Cleft-Lip Palate From Birth To Two Years of AgeCarlos CastañedaNo ratings yet
- Pediatrics & TherapeuticsDocument7 pagesPediatrics & TherapeuticsAmit PasiNo ratings yet
- Abhilash Ghae (Maslp 2) I, Research Proposal, 2020 2022Document27 pagesAbhilash Ghae (Maslp 2) I, Research Proposal, 2020 2022Abhilash GhadeiNo ratings yet
- Sleep Disorders in Pediatric Dentistry: Clinical Guide on Diagnosis and ManagementFrom EverandSleep Disorders in Pediatric Dentistry: Clinical Guide on Diagnosis and ManagementEdmund LiemNo ratings yet
- Endoscopy in Pediatric Inflammatory Bowel DiseaseFrom EverandEndoscopy in Pediatric Inflammatory Bowel DiseaseLuigi Dall'OglioNo ratings yet
- Studies Into Mechanisms Behind Kinesio TapingDocument2 pagesStudies Into Mechanisms Behind Kinesio TapingchristinaNo ratings yet
- Ataxia Coordinative Physiotherapy BroetzDocument12 pagesAtaxia Coordinative Physiotherapy BroetzchristinaNo ratings yet
- Skin Movement in Truck RotationDocument1 pageSkin Movement in Truck RotationchristinaNo ratings yet
- Classroom Activities For Understanding Duchenne: English SpanishDocument6 pagesClassroom Activities For Understanding Duchenne: English SpanishchristinaNo ratings yet
- Poster SOSORT 2014 Elastic Therapeutic TapeDocument1 pagePoster SOSORT 2014 Elastic Therapeutic TapechristinaNo ratings yet
- Organ Zones: Thanking AEVNM For Use of ImageDocument1 pageOrgan Zones: Thanking AEVNM For Use of ImagechristinaNo ratings yet
- Empowering Students To Achieve, Thrive, & SucceedDocument6 pagesEmpowering Students To Achieve, Thrive, & SucceedchristinaNo ratings yet
- Clinical Notes 2 ETT-Ped Taping Pre-TermDocument3 pagesClinical Notes 2 ETT-Ped Taping Pre-TermchristinaNo ratings yet
- Muscle Strength and Physical FitnessDocument20 pagesMuscle Strength and Physical FitnesschristinaNo ratings yet
- What Is Pediatric Heel Pain?Document2 pagesWhat Is Pediatric Heel Pain?christinaNo ratings yet
- Normative Reference Values SPECIFIC TESTSDocument113 pagesNormative Reference Values SPECIFIC TESTSchristinaNo ratings yet
- BLS AlgorithmDocument9 pagesBLS AlgorithmDr VJ GeorgeNo ratings yet
- ZDocument5 pagesZBiljana Custovic RadicicNo ratings yet
- Drug Product PerformanceDocument1 pageDrug Product PerformanceLuna Abigail TorresNo ratings yet
- Balanti An ES School Contingency Plan FINALDocument54 pagesBalanti An ES School Contingency Plan FINALCathyren Capizonda TevesNo ratings yet
- Active Assisted and Passive Movement in TreatmentDocument4 pagesActive Assisted and Passive Movement in TreatmentshravaniNo ratings yet
- What Is ThalassemiaDocument2 pagesWhat Is ThalassemiaFatima Azzahra Khairul AnuarNo ratings yet
- What Is Acrophobia?: Computer-Simulated Phobia PTSD Zoophobia Acrophobia U.S. NavyDocument1 pageWhat Is Acrophobia?: Computer-Simulated Phobia PTSD Zoophobia Acrophobia U.S. NavyE. LópezNo ratings yet
- Module 1Document9 pagesModule 1ALEXANDER BRYAN GONo ratings yet
- CMC-Time Table 1st Year MBBS 150620Document1 pageCMC-Time Table 1st Year MBBS 150620KhanNo ratings yet
- Elsevier - Anaesthesiology Clinics - Vol.26, Issues 1 - Obstetric Anesthesia (2008) PDFDocument230 pagesElsevier - Anaesthesiology Clinics - Vol.26, Issues 1 - Obstetric Anesthesia (2008) PDFMila KarmilaNo ratings yet
- Division 3: Trauma EmergenciesDocument48 pagesDivision 3: Trauma EmergenciesmadhuNo ratings yet
- Indra Diagnostic Centre & Blood Bank: Department of UltrasoundDocument1 pageIndra Diagnostic Centre & Blood Bank: Department of Ultrasoundpassword123resetNo ratings yet
- PROTOZOANS (Blood and Tissue Flagellates)Document4 pagesPROTOZOANS (Blood and Tissue Flagellates)Eunice AndradeNo ratings yet
- CGHS Rate ListDocument39 pagesCGHS Rate ListAniruddha KoparkarNo ratings yet
- Mpu3312 Assignment-May22Document6 pagesMpu3312 Assignment-May22kentbiibibibiNo ratings yet
- CLINPHARM Lab Act 1Document8 pagesCLINPHARM Lab Act 1ezzaNo ratings yet
- Fitness Plan: Luas Wilaya 34 508 542 100.00% 244 48.00 44.00 9.00 11.00 22.00 0.00Document2 pagesFitness Plan: Luas Wilaya 34 508 542 100.00% 244 48.00 44.00 9.00 11.00 22.00 0.00Acep DediNo ratings yet
- 1 s2.0 S0735109786800183 Main PDFDocument252 pages1 s2.0 S0735109786800183 Main PDFdangthieuhoiNo ratings yet
- Aiims 2010 November 2010 DentalDocument62 pagesAiims 2010 November 2010 DentalMrunal Doiphode100% (1)
- Fundamentals of Pharmacology 8th Edition Bullock Test BankDocument9 pagesFundamentals of Pharmacology 8th Edition Bullock Test Bankdorissamuelqpnrrz100% (33)
- A Screening Instrument For Autism Months of Age: A Follow-Up StudyDocument9 pagesA Screening Instrument For Autism Months of Age: A Follow-Up StudyJose Alonso Aguilar ValeraNo ratings yet
- Tinea Capitis Dermoscopy and Calcium Fluorescent Microscopy As Highly Efficient and Precise Diagnostic Tools - Xiao2020Document4 pagesTinea Capitis Dermoscopy and Calcium Fluorescent Microscopy As Highly Efficient and Precise Diagnostic Tools - Xiao2020KhairunNisaNo ratings yet
- BURNDocument5 pagesBURNLara TechiesNo ratings yet
- OB C. 15 Study GuideDocument10 pagesOB C. 15 Study GuidePaige Nicole GauthreauxNo ratings yet
- Presentation BP MonitorDocument7 pagesPresentation BP MonitorImwaniki21No ratings yet
- Fisa Evaluare DurereDocument2 pagesFisa Evaluare DurerecristianNo ratings yet
- Unspoken Needs KrisnamalDocument26 pagesUnspoken Needs Krisnamalmalaysianhospicecouncil6240No ratings yet