Download as pdf or txt
You might also like
- DLL ENGLISH 3 WEEK 2 Q3 HomographsDocument7 pagesDLL ENGLISH 3 WEEK 2 Q3 HomographsOlive L. Gabunal100% (2)
- 4 Roadtec 600 Cummins QSXDocument24 pages4 Roadtec 600 Cummins QSXdavidNo ratings yet
- Lesson Plan 3 2D Shape With ReflectionDocument7 pagesLesson Plan 3 2D Shape With ReflectionfatimaNo ratings yet
- Neurourology and Urodynamics - 2022 - Martin - Is Sacral Neuromodulation Effective in Patients With Parkinson S Disease ADocument7 pagesNeurourology and Urodynamics - 2022 - Martin - Is Sacral Neuromodulation Effective in Patients With Parkinson S Disease AElkin JNo ratings yet
- Relationship Between The Diabetic Polyneuropathy Index and The Neurological Findings of Diabetic PolyneuropathyDocument6 pagesRelationship Between The Diabetic Polyneuropathy Index and The Neurological Findings of Diabetic PolyneuropathyHendro GunawanNo ratings yet
- A Multicenter Cohort StudyDocument9 pagesA Multicenter Cohort Studyfatchurhamzah62No ratings yet
- Art - EDocument7 pagesArt - ECarlos TorresNo ratings yet
- Covid y CorazonDocument19 pagesCovid y CorazonSMIBA MedicinaNo ratings yet
- I-123 Datscan Spect Brain Imaging in Parkinsonian Syndromes: Utility of The Putamen-To-Caudate RatioDocument6 pagesI-123 Datscan Spect Brain Imaging in Parkinsonian Syndromes: Utility of The Putamen-To-Caudate Rationurul auliaNo ratings yet
- Research Paper: NeuropsychiatryDocument11 pagesResearch Paper: NeuropsychiatryveerrajuNo ratings yet
- The CSF Tap Test in Normal Pressure Hydrocephalus - Evaluation Time, Reliability and The Influence of PainDocument6 pagesThe CSF Tap Test in Normal Pressure Hydrocephalus - Evaluation Time, Reliability and The Influence of PainHelena AlessiNo ratings yet
- Clinical Guideline Diagnosing Syncope Part 1: Value of History, Physical Examination, and ElectrocardiographyDocument8 pagesClinical Guideline Diagnosing Syncope Part 1: Value of History, Physical Examination, and ElectrocardiographyPriya JainNo ratings yet
- ContentServer AspDocument8 pagesContentServer AspYuda FhunkshyangNo ratings yet
- Schweitzer 2006Document5 pagesSchweitzer 2006emilNo ratings yet
- Aloysius Elyakim, S.Ked 1408010058 Consulent: DR Donny Argie SP - BS Surgery Departement of W.Z. Johannes Hospital-Nusa Cendana Faculty of MedicineDocument30 pagesAloysius Elyakim, S.Ked 1408010058 Consulent: DR Donny Argie SP - BS Surgery Departement of W.Z. Johannes Hospital-Nusa Cendana Faculty of MedicineShandy BethanNo ratings yet
- AjjababananaDocument7 pagesAjjababananaNaeny BlegurNo ratings yet
- Glyceryl Trinitrate For Acute Intracerebral HemorrhageDocument21 pagesGlyceryl Trinitrate For Acute Intracerebral HemorrhageAhmad Al-atthosNo ratings yet
- Autonomic Neuropathy in Patients With HIV: Course, Impact of Disease Stage, and MedicationDocument6 pagesAutonomic Neuropathy in Patients With HIV: Course, Impact of Disease Stage, and MedicationkarinarakhmaNo ratings yet
- Ou 2016Document8 pagesOu 2016tami widiatul azahraNo ratings yet
- BMM 2018 0348Document14 pagesBMM 2018 0348Harpreet SinghNo ratings yet
- JCDR 10 OC05Document4 pagesJCDR 10 OC05Yafanita IzzatiNo ratings yet
- 55421-Gagal JantungDocument21 pages55421-Gagal JantungAngie CouthalooNo ratings yet
- CTS PDFDocument6 pagesCTS PDFBiola DwikoNo ratings yet
- Causes of Syncope in Patients With AlzheDocument8 pagesCauses of Syncope in Patients With AlzheMichael VavosaNo ratings yet
- Etanercept in Alzheimer Disease: A Randomized, Placebo-Controlled, Double-Blind, Phase 2 TrialDocument8 pagesEtanercept in Alzheimer Disease: A Randomized, Placebo-Controlled, Double-Blind, Phase 2 TrialGiuseppe AcanforaNo ratings yet
- BPPV Comorbid HTDocument4 pagesBPPV Comorbid HTDevi Mutiara JasmineNo ratings yet
- Pulsed Radiofrequency ofDocument8 pagesPulsed Radiofrequency ofDiego Pinto PatroniNo ratings yet
- Art 00011Document6 pagesArt 00011Wanda ArdilaNo ratings yet
- Thesis TopicsDocument14 pagesThesis TopicskiranNo ratings yet
- Restrictive Fluids in Septic Shock. NEJM 2022Document12 pagesRestrictive Fluids in Septic Shock. NEJM 2022neeraj SinghNo ratings yet
- JurnalDocument8 pagesJurnalTher RayNo ratings yet
- SC 2015242Document7 pagesSC 2015242resi ciruNo ratings yet
- Bril (2002) - Validation of The Toronto Clinical Scoring System For Diabetic PolyneuropathyDocument5 pagesBril (2002) - Validation of The Toronto Clinical Scoring System For Diabetic PolyneuropathyRicky WatariNo ratings yet
- Contribution of Speckle Tracking To Estimation of Pulmonary Hypertension by Standard Doppler Echocardiography in Patients With Sys 2161 1149 1000213Document5 pagesContribution of Speckle Tracking To Estimation of Pulmonary Hypertension by Standard Doppler Echocardiography in Patients With Sys 2161 1149 1000213a f indra pratamaNo ratings yet
- Long-Term Clinical Outcome of Fetal Cell Transplantation For Parkinson Disease Two Case ReportsDocument5 pagesLong-Term Clinical Outcome of Fetal Cell Transplantation For Parkinson Disease Two Case Reportsjust for download matterNo ratings yet
- Turn in Bed at NightDocument7 pagesTurn in Bed at NightRiri DaynuriNo ratings yet
- Comparison Between Racemic Bupivacaine and Levobupivacaine Both Combined With Low Dose Fentanyl, Through Intrathecal Route For Transurethral Resection of ProstateDocument4 pagesComparison Between Racemic Bupivacaine and Levobupivacaine Both Combined With Low Dose Fentanyl, Through Intrathecal Route For Transurethral Resection of ProstateInternational Journal of Clinical and Biomedical Research (IJCBR)No ratings yet
- Abstracts USICON2017Document618 pagesAbstracts USICON2017rdLuis1No ratings yet
- FocusDocument9 pagesFocusAdéline NolinNo ratings yet
- Ultrasonido Doppler Temprano AMSDocument7 pagesUltrasonido Doppler Temprano AMSKaren Marbelly OrozcoNo ratings yet
- Cole 2022 Stanford Neuromodulation Therapy SNDocument10 pagesCole 2022 Stanford Neuromodulation Therapy SNVictor Lopez SueroNo ratings yet
- M34 16Document2 pagesM34 16Ana Tomas PetrovicNo ratings yet
- Posterior Tibial Nerve Stimulation As Treatment For The Overactive BladderDocument5 pagesPosterior Tibial Nerve Stimulation As Treatment For The Overactive BladderSendyA-AzizNo ratings yet
- Prevention of Contrast Induced Renal Failure NAC ReviewDocument9 pagesPrevention of Contrast Induced Renal Failure NAC Reviewnaxo128No ratings yet
- Anastomosis Vol 1 Issue 2 PDFDocument36 pagesAnastomosis Vol 1 Issue 2 PDFRashin PNo ratings yet
- 10 1002@mdc3 12810Document10 pages10 1002@mdc3 12810Gonzalo CastroNo ratings yet
- Septic ShockDocument12 pagesSeptic ShockPatrick CommettantNo ratings yet
- Comparison of Surgical Outcome and Complications Between Spinal and General Anaesthesia For Patients Undergoing Percutaneous NephrolithotomyDocument5 pagesComparison of Surgical Outcome and Complications Between Spinal and General Anaesthesia For Patients Undergoing Percutaneous Nephrolithotomynaufal12345No ratings yet
- Fneur 09 00486Document6 pagesFneur 09 00486UnNo ratings yet
- SdarticleDocument6 pagesSdarticleClaudia Alejandra Molina SepulvedaNo ratings yet
- Claudia Craven VENTRICULOMEGALY CLASSIFICATIONDocument17 pagesClaudia Craven VENTRICULOMEGALY CLASSIFICATIONGUI VINCENo ratings yet
- Translateabstract: PatientDocument3 pagesTranslateabstract: PatientAnonymous Rv3ahYRNo ratings yet
- Atm 09 20 1587Document14 pagesAtm 09 20 1587Wina Pertiwi 2003113414No ratings yet
- Indicación RelaparotomiaDocument6 pagesIndicación RelaparotomiaJohnHarvardNo ratings yet
- Comparison of 2 Methods of Neuropathic Pain Assessment in Carpal Tunnel Syndrome and Hand FunctionsDocument8 pagesComparison of 2 Methods of Neuropathic Pain Assessment in Carpal Tunnel Syndrome and Hand FunctionsRidha RazaliNo ratings yet
- Nerjm SesionDocument12 pagesNerjm SesionjorgeNo ratings yet
- Diagnosis of Idiopathic Normal Pressure Hydrocephalus Is Supported by MRI-based Scheme: A Prospective Cohort StudyDocument11 pagesDiagnosis of Idiopathic Normal Pressure Hydrocephalus Is Supported by MRI-based Scheme: A Prospective Cohort StudyDini NanamiNo ratings yet
- A Randomized Controlled Clinical Trial To Compare The Safety and Effi Cacy of Edaravone in Acute Ischemic StrokeDocument5 pagesA Randomized Controlled Clinical Trial To Compare The Safety and Effi Cacy of Edaravone in Acute Ischemic StrokeWahyuni SetiawatiNo ratings yet
- A Practical Two-Step Quantitative Clinical and Electrophysiological Assessment For The Diagnosis and Staging of Dianetic NeuropathyDocument9 pagesA Practical Two-Step Quantitative Clinical and Electrophysiological Assessment For The Diagnosis and Staging of Dianetic NeuropathyGhislaino ItabgaNo ratings yet
- Sp088influence of Telmisartan and Amlodipine Combi PDFDocument3 pagesSp088influence of Telmisartan and Amlodipine Combi PDFKumarsai DurusojuNo ratings yet
- Somatic Manifestations in Renal Disease A Clinical Research StudyDocument14 pagesSomatic Manifestations in Renal Disease A Clinical Research StudyChristian MarchiNo ratings yet
- Long-Term Outcomes After Surgical Treatment of Pediatric Neurogenic Thoracic Outlet SyndromeDocument11 pagesLong-Term Outcomes After Surgical Treatment of Pediatric Neurogenic Thoracic Outlet Syndromewalter fire 0057No ratings yet
- Complementary and Alternative Medical Lab Testing Part 17: OncologyFrom EverandComplementary and Alternative Medical Lab Testing Part 17: OncologyNo ratings yet
- Intracranial Cerebrospinal FluDocument4 pagesIntracranial Cerebrospinal FluAffan AdibNo ratings yet
- Gait Disorders: Editorial CommentaryDocument2 pagesGait Disorders: Editorial CommentaryAffan AdibNo ratings yet
- Alteration of Venous DrainageDocument11 pagesAlteration of Venous DrainageAffan AdibNo ratings yet
- Pitfalls in The Diagnosis of Hydrocephalus: Ymposium ON THE EAD AND ECKDocument4 pagesPitfalls in The Diagnosis of Hydrocephalus: Ymposium ON THE EAD AND ECKAffan AdibNo ratings yet
- 503 FullDocument4 pages503 FullAffan AdibNo ratings yet
- Diagnosis and Treatment of Basal Cell and Squamous Cell CarcinomasDocument8 pagesDiagnosis and Treatment of Basal Cell and Squamous Cell CarcinomasAffan AdibNo ratings yet
- Wpa Supplicant DevelDocument1,952 pagesWpa Supplicant DevelakpolatcemNo ratings yet
- 1) What Is Budgetary Control?Document6 pages1) What Is Budgetary Control?abhiayushNo ratings yet
- Theory Child DevelopmentDocument30 pagesTheory Child Developmentismahanis ghafarNo ratings yet
- How To Log DefectsDocument6 pagesHow To Log DefectsGino AnticonaNo ratings yet
- Wolfram Von Eschenbach - ParzivalDocument324 pagesWolfram Von Eschenbach - ParzivalStanley Castro100% (1)
- 2volt Powerstack BatteriesDocument4 pages2volt Powerstack BatteriesYasirNo ratings yet
- Sample Follow-Up LettersDocument2 pagesSample Follow-Up LettersMhira AlmeroNo ratings yet
- Prepared By:: Dr. Shamsad AhmedDocument29 pagesPrepared By:: Dr. Shamsad AhmedNusrat Jahan NafisaNo ratings yet
- Pembelajaran Literasi Membaca Di Pondok Pesantren Sidogiri Kraton PasuruanDocument17 pagesPembelajaran Literasi Membaca Di Pondok Pesantren Sidogiri Kraton Pasuruanpriyo hartantoNo ratings yet
- Diagrama 950H PDFDocument1 pageDiagrama 950H PDFDaniel Castillo PeñaNo ratings yet
- Professional English 1: WEB 20202 Ms Noorhayati SaharuddinDocument20 pagesProfessional English 1: WEB 20202 Ms Noorhayati SaharuddinAdellNo ratings yet
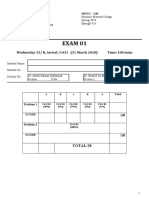
- Meng 310 Exam 01 Spring 2010Document4 pagesMeng 310 Exam 01 Spring 2010Abdulrahman AlzahraniNo ratings yet
- Water ResourcesDocument1 pageWater ResourceshhhhNo ratings yet
- Fyp PPT FinalDocument18 pagesFyp PPT FinalasadNo ratings yet
- Current Limiting Fuses: Proposed NFPA 70-2017 240.67, Arc Modeling and An Assessment Based On IEEE 1584-2002Document8 pagesCurrent Limiting Fuses: Proposed NFPA 70-2017 240.67, Arc Modeling and An Assessment Based On IEEE 1584-2002Ten ApolinarioNo ratings yet
- C & C++ Interview Questions You'll Most Likely Be AskedDocument24 pagesC & C++ Interview Questions You'll Most Likely Be AskedVibrant PublishersNo ratings yet
- Unit 1 - 18EC61Document93 pagesUnit 1 - 18EC61Pritam SarkarNo ratings yet
- Screencast RubricDocument2 pagesScreencast Rubricapi-272483612No ratings yet
- Part Ii: A BC ACB ABC Ø XyzDocument2 pagesPart Ii: A BC ACB ABC Ø XyzHamza NagraNo ratings yet
- Lab 16 - Law of Definite CompositionDocument6 pagesLab 16 - Law of Definite CompositionMicah YapNo ratings yet
- GloverDocument272 pagesGlovermidialaoropesaNo ratings yet
- Database SecurityDocument19 pagesDatabase SecurityVinay VenkatramanNo ratings yet
- [Artificial Intelligence] Ranjan, Sumit, Senthamilarasu, Dr. S. - Applied Deep Learning and Computer Vision for Self-Driving Cars_ Build Autonomous Vehicles Using Deep Neural Networks and Behavi (2020, Packt Publishing) - LibgDocument320 pages[Artificial Intelligence] Ranjan, Sumit, Senthamilarasu, Dr. S. - Applied Deep Learning and Computer Vision for Self-Driving Cars_ Build Autonomous Vehicles Using Deep Neural Networks and Behavi (2020, Packt Publishing) - Libgerik skiNo ratings yet
- HDHR-242U: High Density PolyethyleneDocument1 pageHDHR-242U: High Density Polyethylenefrancisca ulloa riveraNo ratings yet
- Codemap - 2021 No-Code Market ReportDocument34 pagesCodemap - 2021 No-Code Market ReportLogin AppsNo ratings yet
- Layout of NykaaDocument12 pagesLayout of Nykaayogesh DivechaNo ratings yet
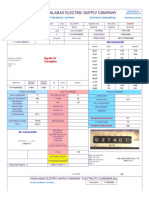
- Fesco Online BillDocument2 pagesFesco Online BillFaisal NaveedNo ratings yet


























































































![[Artificial Intelligence] Ranjan, Sumit, Senthamilarasu, Dr. S. - Applied Deep Learning and Computer Vision for Self-Driving Cars_ Build Autonomous Vehicles Using Deep Neural Networks and Behavi (2020, Packt Publishing) - Libg](https://imgv2-2-f.scribdassets.com/img/document/692994234/149x198/3054a0a56e/1702779147?v=1)