
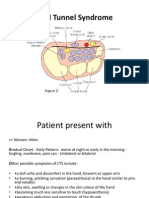
Carpal Tunnel Syndrome: Nabilah Ayob 060 100 814
Carpal Tunnel Syndrome: Nabilah Ayob 060 100 814
You might also like
- Atlas of Oral Maxillofacial SurgeryDocument2 pagesAtlas of Oral Maxillofacial SurgeryStefan PutnikNo ratings yet
- Chronic Kidney Disease Pathophysiology Schematic DiagramDocument3 pagesChronic Kidney Disease Pathophysiology Schematic Diagramnursing concept maps100% (5)
- Korean Hand Therapy KHT Syllabus PDFDocument15 pagesKorean Hand Therapy KHT Syllabus PDFAurora Alina Bujor-FlueranNo ratings yet
- Ergonomics in Dentistry: By, DR - Rakesh R Nair P.G Student Cons & Endo KVG Dental CollegeDocument94 pagesErgonomics in Dentistry: By, DR - Rakesh R Nair P.G Student Cons & Endo KVG Dental Collegenur awanisNo ratings yet
- ICO Exams. E-Source.2019 PDFDocument11 pagesICO Exams. E-Source.2019 PDFHussain SyedNo ratings yet
- Carpal Tunnel SyndromeDocument23 pagesCarpal Tunnel Syndromeanon_312039754No ratings yet
- Presentasi Kasus Carpal Tunnel Syndrome: Presented By: Ihsanul PikriDocument25 pagesPresentasi Kasus Carpal Tunnel Syndrome: Presented By: Ihsanul PikriIhsanNo ratings yet
- Hand & WristDocument56 pagesHand & WristAbdallah Samir Mostafa٢٠١٩٠٢١٥٩No ratings yet
- Carpal Tunnel SyndromeDocument39 pagesCarpal Tunnel SyndromeNindyNo ratings yet
- Carpal Tunnel SyndromeDocument7 pagesCarpal Tunnel SyndromeNeecel PastoralNo ratings yet
- Carpal Tunnel Syndrom Wesam Aljabali - 1Document38 pagesCarpal Tunnel Syndrom Wesam Aljabali - 1مركز ريلاكس للعلاج الطبيعيNo ratings yet
- Carpal Tunnel Syndrome AntyDocument22 pagesCarpal Tunnel Syndrome Antyamel015No ratings yet
- Carpal Tunnel Syndrome-AbiDocument34 pagesCarpal Tunnel Syndrome-AbiSri MahadhanaNo ratings yet
- Carpaltunnelsyndrome 140620053022 Phpapp01Document36 pagesCarpaltunnelsyndrome 140620053022 Phpapp01bennyariepradanaNo ratings yet
- Carpal Tunnel SyndromeDocument22 pagesCarpal Tunnel SyndromePinimNo ratings yet
- Carpal Tunnel SyndromeDocument5 pagesCarpal Tunnel SyndromeCatherine Camille AvelinoNo ratings yet
- Journal Reading CTSDocument27 pagesJournal Reading CTSwillie hardysonNo ratings yet
- Cuestionario Kamath y StothardDocument4 pagesCuestionario Kamath y StothardPasha Camacho100% (1)
- Carpal Tunnel SyndromeDocument2 pagesCarpal Tunnel SyndromeHejar A.No ratings yet
- Carpal Tunnel SyndromeDocument24 pagesCarpal Tunnel SyndromeReymond GuevarraNo ratings yet
- Compressive Neuropathy of Upper LimbDocument49 pagesCompressive Neuropathy of Upper LimbYamunaVaaneeSivalingamNo ratings yet
- Carpal Tunnel Syndrome FinalDocument4 pagesCarpal Tunnel Syndrome Finalcatherine_suganob6496100% (2)
- Carpal Tunnel SyndromeDocument4 pagesCarpal Tunnel Syndromevenks2kNo ratings yet
- Carpal Tunnel Syndrome Power Point PresentationDocument6 pagesCarpal Tunnel Syndrome Power Point Presentationapi-237061134No ratings yet
- EXP Carpal TunnelDocument7 pagesEXP Carpal TunnelRomelyn OrdillasNo ratings yet
- Neurovascular Assessment.... MMMMMDocument7 pagesNeurovascular Assessment.... MMMMMArian May MarcosNo ratings yet
- Introduction: Assignment On Posterior Wrist PalpationDocument11 pagesIntroduction: Assignment On Posterior Wrist PalpationRashi SinghNo ratings yet
- Manual Therapy in The Treatment of Carpal Tunnel Syndrome in Diabetic Patients: A Randomized Clinical TrialDocument34 pagesManual Therapy in The Treatment of Carpal Tunnel Syndrome in Diabetic Patients: A Randomized Clinical Trialnandhini raguNo ratings yet
- Avinash CTSDocument71 pagesAvinash CTSavinashrao39No ratings yet
- Biology Project Work: Mariam Tahoora IXADocument19 pagesBiology Project Work: Mariam Tahoora IXAMariam TahooraNo ratings yet
- Carpal Tunnel SyndormeDocument6 pagesCarpal Tunnel SyndormeMAE THERESE MONICITNo ratings yet
- Carpal Tunnel SyndromeDocument5 pagesCarpal Tunnel Syndromecat momsNo ratings yet
- Carpal Tunnel SyndromeDocument9 pagesCarpal Tunnel SyndromeMaha RajaNo ratings yet
- Neuromusculosklatal Disorders FK UnayaDocument62 pagesNeuromusculosklatal Disorders FK UnayaSuci MayveraNo ratings yet
- Trigger Finger and Ganglion Cyct - Seminar Ortho Year 5Document63 pagesTrigger Finger and Ganglion Cyct - Seminar Ortho Year 5Sh Zahra100% (1)
- Carpal Tunnel SyndromeDocument2 pagesCarpal Tunnel SyndromeTony HermawanNo ratings yet
- Carpal Tunnel SyndromeDocument21 pagesCarpal Tunnel Syndromerudresh singhNo ratings yet
- Carpal Tunnel Syndrome: Recommended ReadingDocument6 pagesCarpal Tunnel Syndrome: Recommended ReadingRezki HarisoeNo ratings yet
- Carpal Tunnel SyndromeDocument38 pagesCarpal Tunnel Syndromereza prayogaNo ratings yet
- Carpal Tunnel SyndromeDocument29 pagesCarpal Tunnel SyndromeAnn Heerah100% (2)
- Carpal Tunnel SyndromeDocument17 pagesCarpal Tunnel SyndromeAstrid IndriatiNo ratings yet
- Carpal Tunnel Syndrome Fact SheetDocument6 pagesCarpal Tunnel Syndrome Fact SheetTissa RanatungeNo ratings yet
- الفصل الثاني محاضرات PDFDocument20 pagesالفصل الثاني محاضرات PDFAZOZ 19No ratings yet
- What Is Carpal Tunnel SyndromeDocument3 pagesWhat Is Carpal Tunnel SyndromerutipuspitaNo ratings yet
- Thoracic Outlet SyndromeDocument16 pagesThoracic Outlet SyndromeDeepak RajNo ratings yet
- De Quervain's TendinosisDocument19 pagesDe Quervain's TendinosisSze Wing LeeNo ratings yet
- Carpal Tunnel SyndromeDocument6 pagesCarpal Tunnel SyndromeRACHELLE ANNE L LUISNo ratings yet
- Peripheral Nerve Disorders (Dr. Ken)Document72 pagesPeripheral Nerve Disorders (Dr. Ken)Nurindha Shimelia M ZNo ratings yet
- De Quervain's TendinosisDocument19 pagesDe Quervain's TendinosisSze Wing LeeNo ratings yet
- Carpal Tunnel Syndrome - Clinical Manifestations and Diagnosis - UpToDateDocument19 pagesCarpal Tunnel Syndrome - Clinical Manifestations and Diagnosis - UpToDatefarhatullahsialNo ratings yet
- Carpal Tunnel Syndrome InforDocument5 pagesCarpal Tunnel Syndrome InforAnonymous uTEAEbugNo ratings yet
- PBL 6Document13 pagesPBL 6polog.jm610No ratings yet
- Traumatic Spinal Cord InjuriesDocument28 pagesTraumatic Spinal Cord Injuriesbibi bennyNo ratings yet
- Carpal Tunnel Syndrome (CTS)Document50 pagesCarpal Tunnel Syndrome (CTS)Nor Fatin GaliNo ratings yet
- Carpal Tunnel SyndromeDocument7 pagesCarpal Tunnel SyndromeSenoirb LemhesNo ratings yet
- CTS-Boy - CtsDocument10 pagesCTS-Boy - CtsFahmi RizqiNo ratings yet
- Hetvi's CTS-ProjectDocument20 pagesHetvi's CTS-Projectshreyathakkar607No ratings yet
- Hand and Wrist DisordersDocument25 pagesHand and Wrist Disorders202003339No ratings yet
- Carpal Tunnel Syndrome (CTS) : by Dr. Rinaldo OslimDocument10 pagesCarpal Tunnel Syndrome (CTS) : by Dr. Rinaldo OslimAidil AdlhaNo ratings yet
- Modul KFR Peripheral NeuropathyDocument68 pagesModul KFR Peripheral NeuropathyHasna Diyani SalamahNo ratings yet
- Wrist and Finger SeminarDocument40 pagesWrist and Finger SeminarMisoNo ratings yet
- Carpal Tunnel SyndromeDocument3 pagesCarpal Tunnel SyndromeAvery SandsNo ratings yet
- Angela Hand and Upper ExtremityDocument59 pagesAngela Hand and Upper ExtremityJenny RajanNo ratings yet
- Carpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandCarpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Clinical Applicability and Diagnostic Performance of Electrocardiographic Criteria For Left Ventricular Hypertrophy Diagnosis in Older AdultsDocument10 pagesClinical Applicability and Diagnostic Performance of Electrocardiographic Criteria For Left Ventricular Hypertrophy Diagnosis in Older AdultsFausto Medina MolinaNo ratings yet
- Recent Advances in Periodontal Surgical Technology: By-Dr Monisha Kaushik 3 Yr MDSDocument20 pagesRecent Advances in Periodontal Surgical Technology: By-Dr Monisha Kaushik 3 Yr MDSmonishakaus24No ratings yet
- Anestesi Luar BiasaDocument51 pagesAnestesi Luar BiasarozanfikriNo ratings yet
- Heal Hormonal Acne A8nmpzDocument29 pagesHeal Hormonal Acne A8nmpzPetra PNo ratings yet
- Adrenal Fatigue WebDocument2 pagesAdrenal Fatigue Webfractalmonkey2No ratings yet
- Somatoform Symptom Disorder: A Diagnostic Dilemma!: BMJ Case Reports November 2019Document5 pagesSomatoform Symptom Disorder: A Diagnostic Dilemma!: BMJ Case Reports November 2019HKNo ratings yet
- Osteoporosis Treatment-Teriparatide Injections - ForteoDocument2 pagesOsteoporosis Treatment-Teriparatide Injections - Forteorameshg2020No ratings yet
- (Medicalstudyzone - Com) NBME 24 ADocument201 pages(Medicalstudyzone - Com) NBME 24 AmarioNo ratings yet
- Nifedipine+for+preterm+labour PPG v4 1 PDFDocument9 pagesNifedipine+for+preterm+labour PPG v4 1 PDFosezele emekaNo ratings yet
- Disorders of The Adrenal GlandsDocument9 pagesDisorders of The Adrenal Glandsmoon businessNo ratings yet
- Uterotonic Agents For Postpartum Hemorrhage PDFDocument1 pageUterotonic Agents For Postpartum Hemorrhage PDFJTNo ratings yet
- CVA or StrokeDocument14 pagesCVA or StrokeJoenalyn AliguinNo ratings yet
- Nle FC Manila 2023 May - EDITEDDocument12 pagesNle FC Manila 2023 May - EDITEDAngela NeriNo ratings yet
- MTAP BACTE MIDTERMS MergedDocument26 pagesMTAP BACTE MIDTERMS MergedLea Juan100% (1)
- Case Presentation On Depression: BY: Mirza Habeeb Pharm D-III Yr 15122D1007Document32 pagesCase Presentation On Depression: BY: Mirza Habeeb Pharm D-III Yr 15122D1007Habeeb0% (1)
- Rationalization 1st PeriodDocument14 pagesRationalization 1st PeriodJenny Agustin FabrosNo ratings yet
- Dissertation DentistryDocument4 pagesDissertation DentistryWriteMyPersuasivePaperSingapore100% (2)
- Surgery 37: Recent Advances inDocument226 pagesSurgery 37: Recent Advances inmudasir61No ratings yet
- Chapter 9KSSM FORM 4 BIODocument12 pagesChapter 9KSSM FORM 4 BIOYEO MING HUI MoeNo ratings yet
- Anaphylactic ShockDocument18 pagesAnaphylactic ShockMarcella AmadeaNo ratings yet
- BIOLOGY MCQsDocument469 pagesBIOLOGY MCQsPrachi KiranNo ratings yet
- Neral Information II. HISTORY OF PRESENT ILLNESS: Patient ExperiencedDocument10 pagesNeral Information II. HISTORY OF PRESENT ILLNESS: Patient ExperiencedBianca Watanabe - RatillaNo ratings yet
- Physiotherapy in Cardiopulmonary Conditions MCQ PDFDocument2 pagesPhysiotherapy in Cardiopulmonary Conditions MCQ PDFDrGyanaranjan Pradhan PT67% (6)
- FULL Download Ebook PDF Handbook of Chronic Kidney Disease Management by John T Daugirdas PDF EbookDocument41 pagesFULL Download Ebook PDF Handbook of Chronic Kidney Disease Management by John T Daugirdas PDF Ebookwilliam.hoisington872100% (45)
- Ajada Volume 6 December 2021 Isssue PDFDocument111 pagesAjada Volume 6 December 2021 Isssue PDFanyango oliloNo ratings yet
- (MT 57) para - MidtermsDocument56 pages(MT 57) para - MidtermsLiana JeonNo ratings yet
























































































Download as pdf or txt
You might also like
- Atlas of Oral Maxillofacial SurgeryDocument2 pagesAtlas of Oral Maxillofacial SurgeryStefan PutnikNo ratings yet
- Chronic Kidney Disease Pathophysiology Schematic DiagramDocument3 pagesChronic Kidney Disease Pathophysiology Schematic Diagramnursing concept maps100% (5)
- Korean Hand Therapy KHT Syllabus PDFDocument15 pagesKorean Hand Therapy KHT Syllabus PDFAurora Alina Bujor-FlueranNo ratings yet
- Ergonomics in Dentistry: By, DR - Rakesh R Nair P.G Student Cons & Endo KVG Dental CollegeDocument94 pagesErgonomics in Dentistry: By, DR - Rakesh R Nair P.G Student Cons & Endo KVG Dental Collegenur awanisNo ratings yet
- ICO Exams. E-Source.2019 PDFDocument11 pagesICO Exams. E-Source.2019 PDFHussain SyedNo ratings yet
- Carpal Tunnel SyndromeDocument23 pagesCarpal Tunnel Syndromeanon_312039754No ratings yet
- Presentasi Kasus Carpal Tunnel Syndrome: Presented By: Ihsanul PikriDocument25 pagesPresentasi Kasus Carpal Tunnel Syndrome: Presented By: Ihsanul PikriIhsanNo ratings yet
- Hand & WristDocument56 pagesHand & WristAbdallah Samir Mostafa٢٠١٩٠٢١٥٩No ratings yet
- Carpal Tunnel SyndromeDocument39 pagesCarpal Tunnel SyndromeNindyNo ratings yet
- Carpal Tunnel SyndromeDocument7 pagesCarpal Tunnel SyndromeNeecel PastoralNo ratings yet
- Carpal Tunnel Syndrom Wesam Aljabali - 1Document38 pagesCarpal Tunnel Syndrom Wesam Aljabali - 1مركز ريلاكس للعلاج الطبيعيNo ratings yet
- Carpal Tunnel Syndrome AntyDocument22 pagesCarpal Tunnel Syndrome Antyamel015No ratings yet
- Carpal Tunnel Syndrome-AbiDocument34 pagesCarpal Tunnel Syndrome-AbiSri MahadhanaNo ratings yet
- Carpaltunnelsyndrome 140620053022 Phpapp01Document36 pagesCarpaltunnelsyndrome 140620053022 Phpapp01bennyariepradanaNo ratings yet
- Carpal Tunnel SyndromeDocument22 pagesCarpal Tunnel SyndromePinimNo ratings yet
- Carpal Tunnel SyndromeDocument5 pagesCarpal Tunnel SyndromeCatherine Camille AvelinoNo ratings yet
- Journal Reading CTSDocument27 pagesJournal Reading CTSwillie hardysonNo ratings yet
- Cuestionario Kamath y StothardDocument4 pagesCuestionario Kamath y StothardPasha Camacho100% (1)
- Carpal Tunnel SyndromeDocument2 pagesCarpal Tunnel SyndromeHejar A.No ratings yet
- Carpal Tunnel SyndromeDocument24 pagesCarpal Tunnel SyndromeReymond GuevarraNo ratings yet
- Compressive Neuropathy of Upper LimbDocument49 pagesCompressive Neuropathy of Upper LimbYamunaVaaneeSivalingamNo ratings yet
- Carpal Tunnel Syndrome FinalDocument4 pagesCarpal Tunnel Syndrome Finalcatherine_suganob6496100% (2)
- Carpal Tunnel SyndromeDocument4 pagesCarpal Tunnel Syndromevenks2kNo ratings yet
- Carpal Tunnel Syndrome Power Point PresentationDocument6 pagesCarpal Tunnel Syndrome Power Point Presentationapi-237061134No ratings yet
- EXP Carpal TunnelDocument7 pagesEXP Carpal TunnelRomelyn OrdillasNo ratings yet
- Neurovascular Assessment.... MMMMMDocument7 pagesNeurovascular Assessment.... MMMMMArian May MarcosNo ratings yet
- Introduction: Assignment On Posterior Wrist PalpationDocument11 pagesIntroduction: Assignment On Posterior Wrist PalpationRashi SinghNo ratings yet
- Manual Therapy in The Treatment of Carpal Tunnel Syndrome in Diabetic Patients: A Randomized Clinical TrialDocument34 pagesManual Therapy in The Treatment of Carpal Tunnel Syndrome in Diabetic Patients: A Randomized Clinical Trialnandhini raguNo ratings yet
- Avinash CTSDocument71 pagesAvinash CTSavinashrao39No ratings yet
- Biology Project Work: Mariam Tahoora IXADocument19 pagesBiology Project Work: Mariam Tahoora IXAMariam TahooraNo ratings yet
- Carpal Tunnel SyndormeDocument6 pagesCarpal Tunnel SyndormeMAE THERESE MONICITNo ratings yet
- Carpal Tunnel SyndromeDocument5 pagesCarpal Tunnel Syndromecat momsNo ratings yet
- Carpal Tunnel SyndromeDocument9 pagesCarpal Tunnel SyndromeMaha RajaNo ratings yet
- Neuromusculosklatal Disorders FK UnayaDocument62 pagesNeuromusculosklatal Disorders FK UnayaSuci MayveraNo ratings yet
- Trigger Finger and Ganglion Cyct - Seminar Ortho Year 5Document63 pagesTrigger Finger and Ganglion Cyct - Seminar Ortho Year 5Sh Zahra100% (1)
- Carpal Tunnel SyndromeDocument2 pagesCarpal Tunnel SyndromeTony HermawanNo ratings yet
- Carpal Tunnel SyndromeDocument21 pagesCarpal Tunnel Syndromerudresh singhNo ratings yet
- Carpal Tunnel Syndrome: Recommended ReadingDocument6 pagesCarpal Tunnel Syndrome: Recommended ReadingRezki HarisoeNo ratings yet
- Carpal Tunnel SyndromeDocument38 pagesCarpal Tunnel Syndromereza prayogaNo ratings yet
- Carpal Tunnel SyndromeDocument29 pagesCarpal Tunnel SyndromeAnn Heerah100% (2)
- Carpal Tunnel SyndromeDocument17 pagesCarpal Tunnel SyndromeAstrid IndriatiNo ratings yet
- Carpal Tunnel Syndrome Fact SheetDocument6 pagesCarpal Tunnel Syndrome Fact SheetTissa RanatungeNo ratings yet
- الفصل الثاني محاضرات PDFDocument20 pagesالفصل الثاني محاضرات PDFAZOZ 19No ratings yet
- What Is Carpal Tunnel SyndromeDocument3 pagesWhat Is Carpal Tunnel SyndromerutipuspitaNo ratings yet
- Thoracic Outlet SyndromeDocument16 pagesThoracic Outlet SyndromeDeepak RajNo ratings yet
- De Quervain's TendinosisDocument19 pagesDe Quervain's TendinosisSze Wing LeeNo ratings yet
- Carpal Tunnel SyndromeDocument6 pagesCarpal Tunnel SyndromeRACHELLE ANNE L LUISNo ratings yet
- Peripheral Nerve Disorders (Dr. Ken)Document72 pagesPeripheral Nerve Disorders (Dr. Ken)Nurindha Shimelia M ZNo ratings yet
- De Quervain's TendinosisDocument19 pagesDe Quervain's TendinosisSze Wing LeeNo ratings yet
- Carpal Tunnel Syndrome - Clinical Manifestations and Diagnosis - UpToDateDocument19 pagesCarpal Tunnel Syndrome - Clinical Manifestations and Diagnosis - UpToDatefarhatullahsialNo ratings yet
- Carpal Tunnel Syndrome InforDocument5 pagesCarpal Tunnel Syndrome InforAnonymous uTEAEbugNo ratings yet
- PBL 6Document13 pagesPBL 6polog.jm610No ratings yet
- Traumatic Spinal Cord InjuriesDocument28 pagesTraumatic Spinal Cord Injuriesbibi bennyNo ratings yet
- Carpal Tunnel Syndrome (CTS)Document50 pagesCarpal Tunnel Syndrome (CTS)Nor Fatin GaliNo ratings yet
- Carpal Tunnel SyndromeDocument7 pagesCarpal Tunnel SyndromeSenoirb LemhesNo ratings yet
- CTS-Boy - CtsDocument10 pagesCTS-Boy - CtsFahmi RizqiNo ratings yet
- Hetvi's CTS-ProjectDocument20 pagesHetvi's CTS-Projectshreyathakkar607No ratings yet
- Hand and Wrist DisordersDocument25 pagesHand and Wrist Disorders202003339No ratings yet
- Carpal Tunnel Syndrome (CTS) : by Dr. Rinaldo OslimDocument10 pagesCarpal Tunnel Syndrome (CTS) : by Dr. Rinaldo OslimAidil AdlhaNo ratings yet
- Modul KFR Peripheral NeuropathyDocument68 pagesModul KFR Peripheral NeuropathyHasna Diyani SalamahNo ratings yet
- Wrist and Finger SeminarDocument40 pagesWrist and Finger SeminarMisoNo ratings yet
- Carpal Tunnel SyndromeDocument3 pagesCarpal Tunnel SyndromeAvery SandsNo ratings yet
- Angela Hand and Upper ExtremityDocument59 pagesAngela Hand and Upper ExtremityJenny RajanNo ratings yet
- Carpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandCarpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Clinical Applicability and Diagnostic Performance of Electrocardiographic Criteria For Left Ventricular Hypertrophy Diagnosis in Older AdultsDocument10 pagesClinical Applicability and Diagnostic Performance of Electrocardiographic Criteria For Left Ventricular Hypertrophy Diagnosis in Older AdultsFausto Medina MolinaNo ratings yet
- Recent Advances in Periodontal Surgical Technology: By-Dr Monisha Kaushik 3 Yr MDSDocument20 pagesRecent Advances in Periodontal Surgical Technology: By-Dr Monisha Kaushik 3 Yr MDSmonishakaus24No ratings yet
- Anestesi Luar BiasaDocument51 pagesAnestesi Luar BiasarozanfikriNo ratings yet
- Heal Hormonal Acne A8nmpzDocument29 pagesHeal Hormonal Acne A8nmpzPetra PNo ratings yet
- Adrenal Fatigue WebDocument2 pagesAdrenal Fatigue Webfractalmonkey2No ratings yet
- Somatoform Symptom Disorder: A Diagnostic Dilemma!: BMJ Case Reports November 2019Document5 pagesSomatoform Symptom Disorder: A Diagnostic Dilemma!: BMJ Case Reports November 2019HKNo ratings yet
- Osteoporosis Treatment-Teriparatide Injections - ForteoDocument2 pagesOsteoporosis Treatment-Teriparatide Injections - Forteorameshg2020No ratings yet
- (Medicalstudyzone - Com) NBME 24 ADocument201 pages(Medicalstudyzone - Com) NBME 24 AmarioNo ratings yet
- Nifedipine+for+preterm+labour PPG v4 1 PDFDocument9 pagesNifedipine+for+preterm+labour PPG v4 1 PDFosezele emekaNo ratings yet
- Disorders of The Adrenal GlandsDocument9 pagesDisorders of The Adrenal Glandsmoon businessNo ratings yet
- Uterotonic Agents For Postpartum Hemorrhage PDFDocument1 pageUterotonic Agents For Postpartum Hemorrhage PDFJTNo ratings yet
- CVA or StrokeDocument14 pagesCVA or StrokeJoenalyn AliguinNo ratings yet
- Nle FC Manila 2023 May - EDITEDDocument12 pagesNle FC Manila 2023 May - EDITEDAngela NeriNo ratings yet
- MTAP BACTE MIDTERMS MergedDocument26 pagesMTAP BACTE MIDTERMS MergedLea Juan100% (1)
- Case Presentation On Depression: BY: Mirza Habeeb Pharm D-III Yr 15122D1007Document32 pagesCase Presentation On Depression: BY: Mirza Habeeb Pharm D-III Yr 15122D1007Habeeb0% (1)
- Rationalization 1st PeriodDocument14 pagesRationalization 1st PeriodJenny Agustin FabrosNo ratings yet
- Dissertation DentistryDocument4 pagesDissertation DentistryWriteMyPersuasivePaperSingapore100% (2)
- Surgery 37: Recent Advances inDocument226 pagesSurgery 37: Recent Advances inmudasir61No ratings yet
- Chapter 9KSSM FORM 4 BIODocument12 pagesChapter 9KSSM FORM 4 BIOYEO MING HUI MoeNo ratings yet
- Anaphylactic ShockDocument18 pagesAnaphylactic ShockMarcella AmadeaNo ratings yet
- BIOLOGY MCQsDocument469 pagesBIOLOGY MCQsPrachi KiranNo ratings yet
- Neral Information II. HISTORY OF PRESENT ILLNESS: Patient ExperiencedDocument10 pagesNeral Information II. HISTORY OF PRESENT ILLNESS: Patient ExperiencedBianca Watanabe - RatillaNo ratings yet
- Physiotherapy in Cardiopulmonary Conditions MCQ PDFDocument2 pagesPhysiotherapy in Cardiopulmonary Conditions MCQ PDFDrGyanaranjan Pradhan PT67% (6)
- FULL Download Ebook PDF Handbook of Chronic Kidney Disease Management by John T Daugirdas PDF EbookDocument41 pagesFULL Download Ebook PDF Handbook of Chronic Kidney Disease Management by John T Daugirdas PDF Ebookwilliam.hoisington872100% (45)
- Ajada Volume 6 December 2021 Isssue PDFDocument111 pagesAjada Volume 6 December 2021 Isssue PDFanyango oliloNo ratings yet
- (MT 57) para - MidtermsDocument56 pages(MT 57) para - MidtermsLiana JeonNo ratings yet