
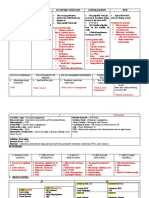
Valvular Heart Disease
Valvular Heart Disease
You might also like
- Sydney Basin Visual Pilot GuideDocument0 pagesSydney Basin Visual Pilot Guidephilridley2No ratings yet
- Codes For Pro, Express, Force & SprintDocument2 pagesCodes For Pro, Express, Force & SprintPelotudoPeloteroNo ratings yet
- Becoming The Perfect Daughter - Spacer XDocument414 pagesBecoming The Perfect Daughter - Spacer XSergio Seferino33% (3)
- Nursing Care of The Child Born With Congenital Heart DisordersDocument3 pagesNursing Care of The Child Born With Congenital Heart DisordersElijah GarciaNo ratings yet
- Word Association PANCEDocument31 pagesWord Association PANCEnevmerka100% (1)
- Very Low-Frequency Electromagnetic Method: A Shallow Subsurface Investigation Technique For Geophysical ApplicationsDocument23 pagesVery Low-Frequency Electromagnetic Method: A Shallow Subsurface Investigation Technique For Geophysical Applicationsassma madouiNo ratings yet
- 4 LD0266Document1 page4 LD0266luyckxj100% (1)
- GS690 Installation Manual Rev ADocument63 pagesGS690 Installation Manual Rev Acasmadi casmadi100% (1)
- Valvular Disease and IEDocument5 pagesValvular Disease and IEdragtoss2No ratings yet
- Mitral StenosisDocument2 pagesMitral StenosisitsmailbbkNo ratings yet
- Valvular HDsDocument2 pagesValvular HDsBell GatesNo ratings yet
- CVS Short Cases: Yapa Wijeratne M/07/189Document2 pagesCVS Short Cases: Yapa Wijeratne M/07/189Li FaungNo ratings yet
- Heart SoundsDocument2 pagesHeart Soundsdanny_awwadNo ratings yet
- Cardiac Examination Inspection, Palpation & Percussion : Dr. Rajesh Bhat UDocument38 pagesCardiac Examination Inspection, Palpation & Percussion : Dr. Rajesh Bhat URanjith RavellaNo ratings yet
- Slide Untuk SabtuDocument35 pagesSlide Untuk SabtuAgustinus FatollaNo ratings yet
- OSCE Internal MedicineDocument139 pagesOSCE Internal MedicineAtef Fahmy100% (2)
- CardiovaskularDocument9 pagesCardiovaskularUnggul YudhaNo ratings yet
- Congenital Heart DiseasesDocument1 pageCongenital Heart DiseasesEmily AnnNo ratings yet
- Mumurs Summary PDFDocument6 pagesMumurs Summary PDFykteo323No ratings yet
- Almaghrabi Cardio ExaminationDocument22 pagesAlmaghrabi Cardio ExaminationSagit Nauman81No ratings yet
- MCQ 1. Heart Sound Heart Sound S1 S2Document7 pagesMCQ 1. Heart Sound Heart Sound S1 S2Atirah AaNo ratings yet
- พี่พงษ์ติวcardioDocument79 pagesพี่พงษ์ติวcardioRapid Medicine67% (3)
- Valvular Heart Disease 2Document46 pagesValvular Heart Disease 2Topea BogdanNo ratings yet
- Paediatrics - Cardiovascular ExaminationDocument5 pagesPaediatrics - Cardiovascular ExaminationhalesipsumNo ratings yet
- ST Elevation MI, STEMIDocument3 pagesST Elevation MI, STEMInmyza89No ratings yet
- Anak 2Document107 pagesAnak 2Nency PurmayaNo ratings yet
- Rheumatic Heart DiseaseDocument21 pagesRheumatic Heart Diseaseram krishnaNo ratings yet
- 1 Cardiovascular System (FINAL) PDFDocument11 pages1 Cardiovascular System (FINAL) PDFJohn Juan TwanNo ratings yet
- 5P MEDICINE2 Valvular Heart Disease 1 - Dr. Rene ManaloDocument6 pages5P MEDICINE2 Valvular Heart Disease 1 - Dr. Rene Manalok.n.e.d.No ratings yet
- Peds Shelf NotesDocument73 pagesPeds Shelf NotesTanyaMusonza100% (1)
- CVS CaseDocument10 pagesCVS Casedoctorumahoney777No ratings yet
- Tao Le, Vikas Bhushan - First Aid For The USMLE Step 1 2020, 30th Anniversary Edition-McGraw-Hill Education (2020) (1) - 1Document9 pagesTao Le, Vikas Bhushan - First Aid For The USMLE Step 1 2020, 30th Anniversary Edition-McGraw-Hill Education (2020) (1) - 1Nanjit SharmaNo ratings yet
- ClinExam by DR AdnanDocument24 pagesClinExam by DR AdnanAdnan ANo ratings yet
- CORNELL NOTE Pediatric Illnesses Part 1&2Document7 pagesCORNELL NOTE Pediatric Illnesses Part 1&2Margareth DandanNo ratings yet
- Dr. Mohammad Shaikhani. Sulaimani University, College of Medicine. Sulaimanya-Iraqi KurdistanDocument51 pagesDr. Mohammad Shaikhani. Sulaimani University, College of Medicine. Sulaimanya-Iraqi KurdistanHNINNo ratings yet
- 3.0 Grand Physiology Finals Compilation - Batch 2017Document89 pages3.0 Grand Physiology Finals Compilation - Batch 2017Sheryl Layne Lao-SebrioNo ratings yet
- Cardiovascular Clinical ExaminationDocument27 pagesCardiovascular Clinical ExaminationAshiniNo ratings yet
- Cardio-Vascular ExaminationDocument43 pagesCardio-Vascular ExaminationDimas FrasesaNo ratings yet
- CVS Heart MurmursDocument2 pagesCVS Heart MurmursIamTinesh100% (1)
- REVIEWER2Document6 pagesREVIEWER2Lorielyn Ashlee GaiteNo ratings yet
- Guidelines For Examination of Cardiovascular System: Bendehiba Latroche, MD, DIS, DIUDocument22 pagesGuidelines For Examination of Cardiovascular System: Bendehiba Latroche, MD, DIS, DIUkskamkalpanaNo ratings yet
- Cardiovascular Shoutouts: When She Says You SayDocument7 pagesCardiovascular Shoutouts: When She Says You SayGbotemi AlaladeNo ratings yet
- Cardiology CardiovascularExaminationDocument5 pagesCardiology CardiovascularExaminationSalifyanji SimpambaNo ratings yet
- CVSDocument71 pagesCVSakshitaNo ratings yet
- Neuro HemorrhagesDocument2 pagesNeuro HemorrhagesmeilunlyNo ratings yet
- Buku HijauDocument22 pagesBuku HijauWahudi YudiNo ratings yet
- Assessment of The Critically Ill PatientDocument5 pagesAssessment of The Critically Ill PatientCris John RicoNo ratings yet
- Peds Shelf NotesDocument88 pagesPeds Shelf Notesγιαννης παπαςNo ratings yet
- Mitral StenosisDocument19 pagesMitral StenosisAbdur RaqibNo ratings yet
- Approach To ArrhythmiasDocument1 pageApproach To ArrhythmiasADITYA SARANGINo ratings yet
- Physical Examination (Wilson)Document11 pagesPhysical Examination (Wilson)Wilson Ong Ying FaNo ratings yet
- PANCE Word Associations PDFDocument27 pagesPANCE Word Associations PDFkatNo ratings yet
- 11 Steps of ECG - Ali Alnahari PDFDocument16 pages11 Steps of ECG - Ali Alnahari PDFBìnhNo ratings yet
- Nclex RN Review Notes 2018 Triple eDocument30 pagesNclex RN Review Notes 2018 Triple eEndla SriniNo ratings yet
- Diaphragm + Abdominal Aorta + IVC + LiverDocument2 pagesDiaphragm + Abdominal Aorta + IVC + LiverannaNo ratings yet
- Cardiac Module - Cardio AnaphyDocument4 pagesCardiac Module - Cardio AnaphyMarie MNNo ratings yet
- CardioDocument13 pagesCardioAnntel RoseNo ratings yet
- Sample Transes 2Document11 pagesSample Transes 2Sophia SalamatNo ratings yet
- Examination of The Cardiovascular SystemDocument2 pagesExamination of The Cardiovascular Systemkenners98% (44)
- Acyanotic Congenital Heart DiseaseDocument48 pagesAcyanotic Congenital Heart DiseasenabillagusrinaNo ratings yet
- Cardiology-1 ValvDocument34 pagesCardiology-1 ValvMahmoud RamadanNo ratings yet
- Step 1 ShartzDocument333 pagesStep 1 ShartzDaniella Vazquez100% (1)
- CardiologyDocument44 pagesCardiologyJim XieNo ratings yet
- Mood StabilizerDocument2 pagesMood Stabilizernmyza89No ratings yet
- Major Depressive Episodes Manic Episode Mixed Episode Hypomanic EpisodeDocument7 pagesMajor Depressive Episodes Manic Episode Mixed Episode Hypomanic Episodenmyza89No ratings yet
- Anxiety Disorder: Yerkes-Dodson Law:an Empirical Relationship Between Arousal andDocument4 pagesAnxiety Disorder: Yerkes-Dodson Law:an Empirical Relationship Between Arousal andnmyza89No ratings yet
- Defense MechanismsDocument5 pagesDefense Mechanismsnmyza89No ratings yet
- INFO Student-Driven AssessmentDocument1 pageINFO Student-Driven Assessmentnmyza89No ratings yet
- Mental Status ExaminationDocument3 pagesMental Status Examinationnmyza89No ratings yet
- PsychiatricDocument1 pagePsychiatricnmyza89No ratings yet
- Evaluation o Suicide RiskDocument2 pagesEvaluation o Suicide Risknmyza89No ratings yet
- DSM OcdDocument2 pagesDSM Ocdnmyza89No ratings yet
- Sudden Cardiac Death: Ischaemic Heart DiseaseDocument4 pagesSudden Cardiac Death: Ischaemic Heart Diseasenmyza89No ratings yet
- Classification of AnaemiaDocument1 pageClassification of Anaemianmyza89No ratings yet
- REVISED Year 4 PPDSupervisor ReportDocument1 pageREVISED Year 4 PPDSupervisor Reportnmyza89No ratings yet
- ST Elevation MI, STEMIDocument3 pagesST Elevation MI, STEMInmyza89No ratings yet
- ? DX Lie N Presentation: Abdominal Palpation VE Auscultation Fetal Heart Sonography /radiographyDocument2 pages? DX Lie N Presentation: Abdominal Palpation VE Auscultation Fetal Heart Sonography /radiographynmyza89No ratings yet
- Fast DPL CTDocument6 pagesFast DPL CTnmyza89No ratings yet
- Surgery - Tools RevisedDocument7 pagesSurgery - Tools Revisednmyza89No ratings yet
- HydrocoeleDocument2 pagesHydrocoelenmyza89No ratings yet
- Past-Years' Exam Questions Cns Anticonvulsant 3. Local AnaestheticDocument2 pagesPast-Years' Exam Questions Cns Anticonvulsant 3. Local Anaestheticnmyza89No ratings yet
- PancreatitisDocument1 pagePancreatitisnmyza89100% (1)
- Appleton CatalogDocument6 pagesAppleton CatalogJay ValdezNo ratings yet
- The Oxford Handbook of Time in Music (Oxford Handbooks)Document556 pagesThe Oxford Handbook of Time in Music (Oxford Handbooks)yi luNo ratings yet
- DBMS Unit VDocument60 pagesDBMS Unit VYuvaraj V, Assistant Professor, BCANo ratings yet
- SE207 Lab ManualDocument44 pagesSE207 Lab ManualchaitanyaNo ratings yet
- Tripp Lite Apsint612Document12 pagesTripp Lite Apsint612samsogoyeNo ratings yet
- Essential DrugsDocument358 pagesEssential Drugsshahera rosdiNo ratings yet
- E-12 Rudder Angle System Sperry RAI PDFDocument116 pagesE-12 Rudder Angle System Sperry RAI PDFAlexandra DuduNo ratings yet
- RL Line/Load Reactors: Driving Power QualityDocument6 pagesRL Line/Load Reactors: Driving Power Qualityjorapa7No ratings yet
- 2011 First Year Scholarship StudentsDocument289 pages2011 First Year Scholarship StudentsBernard100% (2)
- Kitchen SAfety Power Point ComDocument38 pagesKitchen SAfety Power Point CombibubhaskarNo ratings yet
- Vco-151215121140 Import PPTDocument60 pagesVco-151215121140 Import PPTRizwan SPNo ratings yet
- Ayurvedic Herb - EKSHUDocument4 pagesAyurvedic Herb - EKSHUSanjay PisharodiNo ratings yet
- BWSC - Cylinder Liner Monitoring System - 10 0110Document4 pagesBWSC - Cylinder Liner Monitoring System - 10 0110shankar ganesh vadivelNo ratings yet
- MGate MB3180 QIG v3 PDFDocument2 pagesMGate MB3180 QIG v3 PDFHujiLokoNo ratings yet
- GMP Slide Kuliah 2019 - Rev 1Document77 pagesGMP Slide Kuliah 2019 - Rev 1Asta HidayatNo ratings yet
- Physics Challenge Dec14Document2 pagesPhysics Challenge Dec14John DixonNo ratings yet
- Guide To Slide in Bridge ConstructionDocument168 pagesGuide To Slide in Bridge ConstructionpassingtimeNo ratings yet
- Lect2 - 1 11 2011 PDFDocument62 pagesLect2 - 1 11 2011 PDFgendadeyu552625100% (1)
- Electrochemical Model For Performance Analysis of A Tubular SOFCDocument20 pagesElectrochemical Model For Performance Analysis of A Tubular SOFCpapillon tubaNo ratings yet
- Exel Shock Tube - TDS - 2019-03-20 - en - SwedenDocument2 pagesExel Shock Tube - TDS - 2019-03-20 - en - SwedenLejeune HerveNo ratings yet
- Optical Micros PDFDocument24 pagesOptical Micros PDFsensoham03No ratings yet
- My PROPOSALSDocument33 pagesMy PROPOSALSdursam328No ratings yet
- MIT - DT - Week 1 - TranscriptsDocument16 pagesMIT - DT - Week 1 - TranscriptsEzra GaneshaNo ratings yet
- REX012832GYAP3N0Document28 pagesREX012832GYAP3N0marius.chitigaNo ratings yet










































































































Download as docx or pdf
You might also like
- Sydney Basin Visual Pilot GuideDocument0 pagesSydney Basin Visual Pilot Guidephilridley2No ratings yet
- Codes For Pro, Express, Force & SprintDocument2 pagesCodes For Pro, Express, Force & SprintPelotudoPeloteroNo ratings yet
- Becoming The Perfect Daughter - Spacer XDocument414 pagesBecoming The Perfect Daughter - Spacer XSergio Seferino33% (3)
- Nursing Care of The Child Born With Congenital Heart DisordersDocument3 pagesNursing Care of The Child Born With Congenital Heart DisordersElijah GarciaNo ratings yet
- Word Association PANCEDocument31 pagesWord Association PANCEnevmerka100% (1)
- Very Low-Frequency Electromagnetic Method: A Shallow Subsurface Investigation Technique For Geophysical ApplicationsDocument23 pagesVery Low-Frequency Electromagnetic Method: A Shallow Subsurface Investigation Technique For Geophysical Applicationsassma madouiNo ratings yet
- 4 LD0266Document1 page4 LD0266luyckxj100% (1)
- GS690 Installation Manual Rev ADocument63 pagesGS690 Installation Manual Rev Acasmadi casmadi100% (1)
- Valvular Disease and IEDocument5 pagesValvular Disease and IEdragtoss2No ratings yet
- Mitral StenosisDocument2 pagesMitral StenosisitsmailbbkNo ratings yet
- Valvular HDsDocument2 pagesValvular HDsBell GatesNo ratings yet
- CVS Short Cases: Yapa Wijeratne M/07/189Document2 pagesCVS Short Cases: Yapa Wijeratne M/07/189Li FaungNo ratings yet
- Heart SoundsDocument2 pagesHeart Soundsdanny_awwadNo ratings yet
- Cardiac Examination Inspection, Palpation & Percussion : Dr. Rajesh Bhat UDocument38 pagesCardiac Examination Inspection, Palpation & Percussion : Dr. Rajesh Bhat URanjith RavellaNo ratings yet
- Slide Untuk SabtuDocument35 pagesSlide Untuk SabtuAgustinus FatollaNo ratings yet
- OSCE Internal MedicineDocument139 pagesOSCE Internal MedicineAtef Fahmy100% (2)
- CardiovaskularDocument9 pagesCardiovaskularUnggul YudhaNo ratings yet
- Congenital Heart DiseasesDocument1 pageCongenital Heart DiseasesEmily AnnNo ratings yet
- Mumurs Summary PDFDocument6 pagesMumurs Summary PDFykteo323No ratings yet
- Almaghrabi Cardio ExaminationDocument22 pagesAlmaghrabi Cardio ExaminationSagit Nauman81No ratings yet
- MCQ 1. Heart Sound Heart Sound S1 S2Document7 pagesMCQ 1. Heart Sound Heart Sound S1 S2Atirah AaNo ratings yet
- พี่พงษ์ติวcardioDocument79 pagesพี่พงษ์ติวcardioRapid Medicine67% (3)
- Valvular Heart Disease 2Document46 pagesValvular Heart Disease 2Topea BogdanNo ratings yet
- Paediatrics - Cardiovascular ExaminationDocument5 pagesPaediatrics - Cardiovascular ExaminationhalesipsumNo ratings yet
- ST Elevation MI, STEMIDocument3 pagesST Elevation MI, STEMInmyza89No ratings yet
- Anak 2Document107 pagesAnak 2Nency PurmayaNo ratings yet
- Rheumatic Heart DiseaseDocument21 pagesRheumatic Heart Diseaseram krishnaNo ratings yet
- 1 Cardiovascular System (FINAL) PDFDocument11 pages1 Cardiovascular System (FINAL) PDFJohn Juan TwanNo ratings yet
- 5P MEDICINE2 Valvular Heart Disease 1 - Dr. Rene ManaloDocument6 pages5P MEDICINE2 Valvular Heart Disease 1 - Dr. Rene Manalok.n.e.d.No ratings yet
- Peds Shelf NotesDocument73 pagesPeds Shelf NotesTanyaMusonza100% (1)
- CVS CaseDocument10 pagesCVS Casedoctorumahoney777No ratings yet
- Tao Le, Vikas Bhushan - First Aid For The USMLE Step 1 2020, 30th Anniversary Edition-McGraw-Hill Education (2020) (1) - 1Document9 pagesTao Le, Vikas Bhushan - First Aid For The USMLE Step 1 2020, 30th Anniversary Edition-McGraw-Hill Education (2020) (1) - 1Nanjit SharmaNo ratings yet
- ClinExam by DR AdnanDocument24 pagesClinExam by DR AdnanAdnan ANo ratings yet
- CORNELL NOTE Pediatric Illnesses Part 1&2Document7 pagesCORNELL NOTE Pediatric Illnesses Part 1&2Margareth DandanNo ratings yet
- Dr. Mohammad Shaikhani. Sulaimani University, College of Medicine. Sulaimanya-Iraqi KurdistanDocument51 pagesDr. Mohammad Shaikhani. Sulaimani University, College of Medicine. Sulaimanya-Iraqi KurdistanHNINNo ratings yet
- 3.0 Grand Physiology Finals Compilation - Batch 2017Document89 pages3.0 Grand Physiology Finals Compilation - Batch 2017Sheryl Layne Lao-SebrioNo ratings yet
- Cardiovascular Clinical ExaminationDocument27 pagesCardiovascular Clinical ExaminationAshiniNo ratings yet
- Cardio-Vascular ExaminationDocument43 pagesCardio-Vascular ExaminationDimas FrasesaNo ratings yet
- CVS Heart MurmursDocument2 pagesCVS Heart MurmursIamTinesh100% (1)
- REVIEWER2Document6 pagesREVIEWER2Lorielyn Ashlee GaiteNo ratings yet
- Guidelines For Examination of Cardiovascular System: Bendehiba Latroche, MD, DIS, DIUDocument22 pagesGuidelines For Examination of Cardiovascular System: Bendehiba Latroche, MD, DIS, DIUkskamkalpanaNo ratings yet
- Cardiovascular Shoutouts: When She Says You SayDocument7 pagesCardiovascular Shoutouts: When She Says You SayGbotemi AlaladeNo ratings yet
- Cardiology CardiovascularExaminationDocument5 pagesCardiology CardiovascularExaminationSalifyanji SimpambaNo ratings yet
- CVSDocument71 pagesCVSakshitaNo ratings yet
- Neuro HemorrhagesDocument2 pagesNeuro HemorrhagesmeilunlyNo ratings yet
- Buku HijauDocument22 pagesBuku HijauWahudi YudiNo ratings yet
- Assessment of The Critically Ill PatientDocument5 pagesAssessment of The Critically Ill PatientCris John RicoNo ratings yet
- Peds Shelf NotesDocument88 pagesPeds Shelf Notesγιαννης παπαςNo ratings yet
- Mitral StenosisDocument19 pagesMitral StenosisAbdur RaqibNo ratings yet
- Approach To ArrhythmiasDocument1 pageApproach To ArrhythmiasADITYA SARANGINo ratings yet
- Physical Examination (Wilson)Document11 pagesPhysical Examination (Wilson)Wilson Ong Ying FaNo ratings yet
- PANCE Word Associations PDFDocument27 pagesPANCE Word Associations PDFkatNo ratings yet
- 11 Steps of ECG - Ali Alnahari PDFDocument16 pages11 Steps of ECG - Ali Alnahari PDFBìnhNo ratings yet
- Nclex RN Review Notes 2018 Triple eDocument30 pagesNclex RN Review Notes 2018 Triple eEndla SriniNo ratings yet
- Diaphragm + Abdominal Aorta + IVC + LiverDocument2 pagesDiaphragm + Abdominal Aorta + IVC + LiverannaNo ratings yet
- Cardiac Module - Cardio AnaphyDocument4 pagesCardiac Module - Cardio AnaphyMarie MNNo ratings yet
- CardioDocument13 pagesCardioAnntel RoseNo ratings yet
- Sample Transes 2Document11 pagesSample Transes 2Sophia SalamatNo ratings yet
- Examination of The Cardiovascular SystemDocument2 pagesExamination of The Cardiovascular Systemkenners98% (44)
- Acyanotic Congenital Heart DiseaseDocument48 pagesAcyanotic Congenital Heart DiseasenabillagusrinaNo ratings yet
- Cardiology-1 ValvDocument34 pagesCardiology-1 ValvMahmoud RamadanNo ratings yet
- Step 1 ShartzDocument333 pagesStep 1 ShartzDaniella Vazquez100% (1)
- CardiologyDocument44 pagesCardiologyJim XieNo ratings yet
- Mood StabilizerDocument2 pagesMood Stabilizernmyza89No ratings yet
- Major Depressive Episodes Manic Episode Mixed Episode Hypomanic EpisodeDocument7 pagesMajor Depressive Episodes Manic Episode Mixed Episode Hypomanic Episodenmyza89No ratings yet
- Anxiety Disorder: Yerkes-Dodson Law:an Empirical Relationship Between Arousal andDocument4 pagesAnxiety Disorder: Yerkes-Dodson Law:an Empirical Relationship Between Arousal andnmyza89No ratings yet
- Defense MechanismsDocument5 pagesDefense Mechanismsnmyza89No ratings yet
- INFO Student-Driven AssessmentDocument1 pageINFO Student-Driven Assessmentnmyza89No ratings yet
- Mental Status ExaminationDocument3 pagesMental Status Examinationnmyza89No ratings yet
- PsychiatricDocument1 pagePsychiatricnmyza89No ratings yet
- Evaluation o Suicide RiskDocument2 pagesEvaluation o Suicide Risknmyza89No ratings yet
- DSM OcdDocument2 pagesDSM Ocdnmyza89No ratings yet
- Sudden Cardiac Death: Ischaemic Heart DiseaseDocument4 pagesSudden Cardiac Death: Ischaemic Heart Diseasenmyza89No ratings yet
- Classification of AnaemiaDocument1 pageClassification of Anaemianmyza89No ratings yet
- REVISED Year 4 PPDSupervisor ReportDocument1 pageREVISED Year 4 PPDSupervisor Reportnmyza89No ratings yet
- ST Elevation MI, STEMIDocument3 pagesST Elevation MI, STEMInmyza89No ratings yet
- ? DX Lie N Presentation: Abdominal Palpation VE Auscultation Fetal Heart Sonography /radiographyDocument2 pages? DX Lie N Presentation: Abdominal Palpation VE Auscultation Fetal Heart Sonography /radiographynmyza89No ratings yet
- Fast DPL CTDocument6 pagesFast DPL CTnmyza89No ratings yet
- Surgery - Tools RevisedDocument7 pagesSurgery - Tools Revisednmyza89No ratings yet
- HydrocoeleDocument2 pagesHydrocoelenmyza89No ratings yet
- Past-Years' Exam Questions Cns Anticonvulsant 3. Local AnaestheticDocument2 pagesPast-Years' Exam Questions Cns Anticonvulsant 3. Local Anaestheticnmyza89No ratings yet
- PancreatitisDocument1 pagePancreatitisnmyza89100% (1)
- Appleton CatalogDocument6 pagesAppleton CatalogJay ValdezNo ratings yet
- The Oxford Handbook of Time in Music (Oxford Handbooks)Document556 pagesThe Oxford Handbook of Time in Music (Oxford Handbooks)yi luNo ratings yet
- DBMS Unit VDocument60 pagesDBMS Unit VYuvaraj V, Assistant Professor, BCANo ratings yet
- SE207 Lab ManualDocument44 pagesSE207 Lab ManualchaitanyaNo ratings yet
- Tripp Lite Apsint612Document12 pagesTripp Lite Apsint612samsogoyeNo ratings yet
- Essential DrugsDocument358 pagesEssential Drugsshahera rosdiNo ratings yet
- E-12 Rudder Angle System Sperry RAI PDFDocument116 pagesE-12 Rudder Angle System Sperry RAI PDFAlexandra DuduNo ratings yet
- RL Line/Load Reactors: Driving Power QualityDocument6 pagesRL Line/Load Reactors: Driving Power Qualityjorapa7No ratings yet
- 2011 First Year Scholarship StudentsDocument289 pages2011 First Year Scholarship StudentsBernard100% (2)
- Kitchen SAfety Power Point ComDocument38 pagesKitchen SAfety Power Point CombibubhaskarNo ratings yet
- Vco-151215121140 Import PPTDocument60 pagesVco-151215121140 Import PPTRizwan SPNo ratings yet
- Ayurvedic Herb - EKSHUDocument4 pagesAyurvedic Herb - EKSHUSanjay PisharodiNo ratings yet
- BWSC - Cylinder Liner Monitoring System - 10 0110Document4 pagesBWSC - Cylinder Liner Monitoring System - 10 0110shankar ganesh vadivelNo ratings yet
- MGate MB3180 QIG v3 PDFDocument2 pagesMGate MB3180 QIG v3 PDFHujiLokoNo ratings yet
- GMP Slide Kuliah 2019 - Rev 1Document77 pagesGMP Slide Kuliah 2019 - Rev 1Asta HidayatNo ratings yet
- Physics Challenge Dec14Document2 pagesPhysics Challenge Dec14John DixonNo ratings yet
- Guide To Slide in Bridge ConstructionDocument168 pagesGuide To Slide in Bridge ConstructionpassingtimeNo ratings yet
- Lect2 - 1 11 2011 PDFDocument62 pagesLect2 - 1 11 2011 PDFgendadeyu552625100% (1)
- Electrochemical Model For Performance Analysis of A Tubular SOFCDocument20 pagesElectrochemical Model For Performance Analysis of A Tubular SOFCpapillon tubaNo ratings yet
- Exel Shock Tube - TDS - 2019-03-20 - en - SwedenDocument2 pagesExel Shock Tube - TDS - 2019-03-20 - en - SwedenLejeune HerveNo ratings yet
- Optical Micros PDFDocument24 pagesOptical Micros PDFsensoham03No ratings yet
- My PROPOSALSDocument33 pagesMy PROPOSALSdursam328No ratings yet
- MIT - DT - Week 1 - TranscriptsDocument16 pagesMIT - DT - Week 1 - TranscriptsEzra GaneshaNo ratings yet
- REX012832GYAP3N0Document28 pagesREX012832GYAP3N0marius.chitigaNo ratings yet