Download as pdf or txt
You might also like
- Case Presentation: Acute GastroenteritisDocument60 pagesCase Presentation: Acute GastroenteritisBeverly Datu86% (7)
- Form - Student Health Certificate-1Document2 pagesForm - Student Health Certificate-1hmhida33% (3)
- Ms Exam 500 Items - Answers With RatioDocument61 pagesMs Exam 500 Items - Answers With RatioPrincessDiane'LouiseBautistaMartinNo ratings yet
- Ortho Bone ScrewDocument17 pagesOrtho Bone Screwmedicalcenter100% (1)
- Jurnal 3 WordDocument6 pagesJurnal 3 WordlindaNo ratings yet
- 2014 AJODO SilveiraDocument11 pages2014 AJODO SilveiraJavier Farias VeraNo ratings yet
- Bioprogressive OrthoDocument18 pagesBioprogressive OrthoVishnu S PattathNo ratings yet
- 1 s2.0 S2666430522000036 MainDocument12 pages1 s2.0 S2666430522000036 MainDANTE DELEGUERYNo ratings yet
- Ankylosis of The Temporomandibular Joint and Mandibular Growth Disturbance Caused by Neglected Condylar Fracture in ChildhoodDocument5 pagesAnkylosis of The Temporomandibular Joint and Mandibular Growth Disturbance Caused by Neglected Condylar Fracture in Childhoodfarron_vNo ratings yet
- Case Report Lateral Open Bite Treatment Stability OMT Essential Cabrera USP Brazil AJO DO 2011Document11 pagesCase Report Lateral Open Bite Treatment Stability OMT Essential Cabrera USP Brazil AJO DO 2011AndreaVanoyMartinNo ratings yet
- Openbite CamouflageDocument8 pagesOpenbite CamouflageRakesh RaveendranNo ratings yet
- Pedo JurnalDocument5 pagesPedo JurnalAngelinaNo ratings yet
- Severe Class II Division 1 MalocclusionDocument14 pagesSevere Class II Division 1 MalocclusionCARMEN ROSA AREVALO ROLDANNo ratings yet
- Open Bite: Diagnosis, Treatment and StabilityDocument12 pagesOpen Bite: Diagnosis, Treatment and Stabilityjavi222222No ratings yet
- Case Report: Bhandari PPDocument2 pagesCase Report: Bhandari PPEgiNo ratings yet
- Treatment of Unilateral Buccal Crossbites in The Primary, Early Mixed, and Permanent Dentitions: Case ReportsDocument6 pagesTreatment of Unilateral Buccal Crossbites in The Primary, Early Mixed, and Permanent Dentitions: Case ReportsRisma AisyaNo ratings yet
- Unilateral Cross Bite Treated by Corticotomy-Assisted Expansion: Two Case ReportsDocument9 pagesUnilateral Cross Bite Treated by Corticotomy-Assisted Expansion: Two Case ReportsJavier Farias VeraNo ratings yet
- Orthodontic-Surgical Management of A Horizontally Impacted MaxillDocument13 pagesOrthodontic-Surgical Management of A Horizontally Impacted MaxillegyNo ratings yet
- Maturogenesis of A Complicated Crown Fracture: A Case Report With 8 Years Follow-UpDocument4 pagesMaturogenesis of A Complicated Crown Fracture: A Case Report With 8 Years Follow-UpKIH 20162017No ratings yet
- Maxillary Arch Distalization Using Interradicular Miniscrews and The Lever-Arm ApplianceDocument8 pagesMaxillary Arch Distalization Using Interradicular Miniscrews and The Lever-Arm ApplianceJuan Carlos CárcamoNo ratings yet
- Open Bite: Diagnosis, Treatment and StabilityDocument11 pagesOpen Bite: Diagnosis, Treatment and StabilityJavier Farias VeraNo ratings yet
- Angle Class II Malocclusion Treated Without Extractions and With Growth ControlDocument11 pagesAngle Class II Malocclusion Treated Without Extractions and With Growth ControlishtiiiNo ratings yet
- Catlan's ApplianceDocument5 pagesCatlan's ApplianceFirma Nurdinia DewiNo ratings yet
- Ectopic Tooth in Maxillary Sinus: Case SeriesDocument0 pagesEctopic Tooth in Maxillary Sinus: Case Seriestitis istya aNo ratings yet
- Multidisciplinary Approach For The Treatment of Horizontal Root-Fractured Maxillary Anterior TeethDocument11 pagesMultidisciplinary Approach For The Treatment of Horizontal Root-Fractured Maxillary Anterior TeethGülbike DemirelNo ratings yet
- Open-Cap Acrylic SplintDocument3 pagesOpen-Cap Acrylic SplintFeras Al-ZbounNo ratings yet
- Journal Endang - Ijsr Juli 2020, Fracture MandibleDocument5 pagesJournal Endang - Ijsr Juli 2020, Fracture MandibleEndang Samsudin FKGNo ratings yet
- Premolar Transplantation To Replace A Missing Central IncisorDocument12 pagesPremolar Transplantation To Replace A Missing Central IncisorMaryGonzalesʚïɞNo ratings yet
- EmbedeedDocument4 pagesEmbedeedLori SimmonsNo ratings yet
- AJO DO Revista ArticuloDocument10 pagesAJO DO Revista ArticuloAngélicaLujánNo ratings yet
- A Rare Case Report Along With Surgical Management of Bilateral Maxillary Buccal Exostosis in A Patient of Polydactyly and Distomol.Document3 pagesA Rare Case Report Along With Surgical Management of Bilateral Maxillary Buccal Exostosis in A Patient of Polydactyly and Distomol.Fransiski HoNo ratings yet
- Pulp Revascularization in Immature Permanent Tooth With Apical Periodontitis Using MTADocument6 pagesPulp Revascularization in Immature Permanent Tooth With Apical Periodontitis Using MTALori SimmonsNo ratings yet
- Mandibular Premolar Transplantation To Replace Missing Maxillary Anterior Teeth: A Multidisciplinary ApproachDocument14 pagesMandibular Premolar Transplantation To Replace Missing Maxillary Anterior Teeth: A Multidisciplinary ApproachRicha AhlawatNo ratings yet
- Jurnal Acc 1Document4 pagesJurnal Acc 1Egga Mariana YudaNo ratings yet
- Case Report: Surgical Management of Compound Odontoma Associated With Unerupted ToothDocument7 pagesCase Report: Surgical Management of Compound Odontoma Associated With Unerupted ToothDame rohanaNo ratings yet
- Dental Anomaly 1Document6 pagesDental Anomaly 1Fachriza AfriNo ratings yet
- Closed Reduction Treatment Parasimfisis (Ada Radriograf), Dan Tata LaksananyaDocument7 pagesClosed Reduction Treatment Parasimfisis (Ada Radriograf), Dan Tata LaksananyaVincent AriesNo ratings yet
- Clinical Case Reports - 2022 - Guo - Unicystic Ameloblastoma in A 9 Year Old Child Treated With A Combination ofDocument4 pagesClinical Case Reports - 2022 - Guo - Unicystic Ameloblastoma in A 9 Year Old Child Treated With A Combination ofSaul SilvaNo ratings yet
- Ijda July-Sep 2015Document5 pagesIjda July-Sep 2015bhaskaracharya dontabhaktuniNo ratings yet
- Severe Crowding and A Dilacerated Maxillary Central Incisor in An AdolescentDocument9 pagesSevere Crowding and A Dilacerated Maxillary Central Incisor in An AdolescentDaneyi Giraldo LoaizaNo ratings yet
- Nuevo 3Document4 pagesNuevo 3Salma FaNo ratings yet
- Mukherjee Et AlDocument5 pagesMukherjee Et AlSohaib ShujaatNo ratings yet
- Anterior Crossbite Correction in Early Mixed Dentition Stage Using Functional Jaw Orthopedics Principles: A Case Report With Two-Years Follow-UpDocument13 pagesAnterior Crossbite Correction in Early Mixed Dentition Stage Using Functional Jaw Orthopedics Principles: A Case Report With Two-Years Follow-UpTsaniya KamilahNo ratings yet
- A Case Report On Orthodontic Management of An Adolescent Cleft PatientDocument4 pagesA Case Report On Orthodontic Management of An Adolescent Cleft PatientMichelle WibiantoNo ratings yet
- CE (Ra) F (P) PF1 (EKAK) PFA (AK) PF2 (PAG)Document3 pagesCE (Ra) F (P) PF1 (EKAK) PFA (AK) PF2 (PAG)Lila karla leon villarNo ratings yet
- Jurnal GicDocument6 pagesJurnal GicHusnul KhatimahNo ratings yet
- Odontogenic Cutaneous Sinus Tract Associated With A Mandibular Second Molar Having A Rare Distolingual Root: A Case ReportDocument6 pagesOdontogenic Cutaneous Sinus Tract Associated With A Mandibular Second Molar Having A Rare Distolingual Root: A Case ReportMa NelNo ratings yet
- Atypical Extraction Treatment For Failing Replante - 2020 - American Journal ofDocument11 pagesAtypical Extraction Treatment For Failing Replante - 2020 - American Journal ofAlejandro Aranzábal NavarreteNo ratings yet
- Management of Sub Condylar Fracture in 15 Yr Old Patient: Case ReportDocument6 pagesManagement of Sub Condylar Fracture in 15 Yr Old Patient: Case ReportIma ShofyaNo ratings yet
- Exostosis MandibularDocument6 pagesExostosis MandibularCOne Gomez LinarteNo ratings yet
- 9PediatricTraumavol5issue5p34-39 201910170840181Document7 pages9PediatricTraumavol5issue5p34-39 201910170840181waleed MagidNo ratings yet
- Lanza 2017Document7 pagesLanza 2017Promocoes PromoNo ratings yet
- Root Resorption A 6-Year Follow-Up Case ReportDocument3 pagesRoot Resorption A 6-Year Follow-Up Case Reportpaola lopezNo ratings yet
- Bilateral Cleft Lip and PalateDocument10 pagesBilateral Cleft Lip and PalateAly OsmanNo ratings yet
- Segmental Alveolar Process FractureDocument4 pagesSegmental Alveolar Process FracturegiselaNo ratings yet
- Full Mouth Rehabilitation of The Patient With Severly Worn Out Dentition A Case Report.Document5 pagesFull Mouth Rehabilitation of The Patient With Severly Worn Out Dentition A Case Report.sivak_198100% (1)
- Management of Anterior Dental Crossbite With Removable AppliancesDocument4 pagesManagement of Anterior Dental Crossbite With Removable AppliancesSurya WijayaNo ratings yet
- Severe Gingival Recession Caused by Orthodontic Rubber Band: A Case ReportDocument5 pagesSevere Gingival Recession Caused by Orthodontic Rubber Band: A Case ReportanjozzNo ratings yet
- MapaDocument9 pagesMapaRicha AhlawatNo ratings yet
- Kuchler 2010Document4 pagesKuchler 2010Juliete OliveiraNo ratings yet
- Case ReportDocument8 pagesCase ReportKeyla Paola De La Hoz FonsecaNo ratings yet
- Blended Learning To Improve Learning Outcomes in Digital Electronics CoursesDocument3 pagesBlended Learning To Improve Learning Outcomes in Digital Electronics CoursesIndra D KristionoNo ratings yet
- Guava Tea Leaves: July 2020Document8 pagesGuava Tea Leaves: July 2020Indra D KristionoNo ratings yet
- Effectiveness, Efficiency and Instruction Appeal of Blended Learning ModelDocument18 pagesEffectiveness, Efficiency and Instruction Appeal of Blended Learning ModelIndra D KristionoNo ratings yet
- Complications and Pitfalls in Maxillofacial Trauma: 10.5005/jp-Journals-10028-1108Document7 pagesComplications and Pitfalls in Maxillofacial Trauma: 10.5005/jp-Journals-10028-1108Indra D KristionoNo ratings yet
- Management of Firearm Facial Fractures at The Dr. José Eleuterio González'': University Hospital CaseDocument4 pagesManagement of Firearm Facial Fractures at The Dr. José Eleuterio González'': University Hospital CaseIndra D KristionoNo ratings yet
- Management of Facial Injuries in Elite and Professional Sports A Consensus ReportDocument6 pagesManagement of Facial Injuries in Elite and Professional Sports A Consensus ReportIndra D KristionoNo ratings yet
- Article 2 - NZMJ Midface FracturesDocument9 pagesArticle 2 - NZMJ Midface FracturesIndra D KristionoNo ratings yet
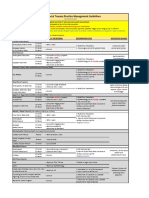
- VUMC Facial Trauma Practice Management GuidelinesDocument1 pageVUMC Facial Trauma Practice Management GuidelinesIndra D KristionoNo ratings yet
- Pengaruh Peningkatan Konsentrasi Pati Biji Alpukat (Persea Americana Mill.) SEBAGAI PENGIKAT TERHADAP Karakteristik Fisik Granul Dan Tablet Ekstrak Akar Alang-ALANG (Imperata Cylindrica Linn.)Document5 pagesPengaruh Peningkatan Konsentrasi Pati Biji Alpukat (Persea Americana Mill.) SEBAGAI PENGIKAT TERHADAP Karakteristik Fisik Granul Dan Tablet Ekstrak Akar Alang-ALANG (Imperata Cylindrica Linn.)Indra D KristionoNo ratings yet
- Tuberculin Skin TestDocument2 pagesTuberculin Skin Testcalmira3653No ratings yet
- Mechanical InjuriesDocument75 pagesMechanical InjuriesArpit MalhotraNo ratings yet
- The Bigger The Bulge The Better - Rayner & Smale PDFDocument4 pagesThe Bigger The Bulge The Better - Rayner & Smale PDFItai IzhakNo ratings yet
- Association Between Breastfeeding Patterns and Type 1 Diabetes Among ChildrenDocument6 pagesAssociation Between Breastfeeding Patterns and Type 1 Diabetes Among ChildrenHarun joel tatipataNo ratings yet
- Wilson's DiseaseDocument52 pagesWilson's DiseaseAmit KumarNo ratings yet
- Practical Application of CPAP: Dr. Srinivas MurkiDocument8 pagesPractical Application of CPAP: Dr. Srinivas MurkiRaji MohanNo ratings yet
- Trauma-Sensitive Yoga - Principles, Practice and ResearchDocument6 pagesTrauma-Sensitive Yoga - Principles, Practice and ResearchRichard Guerra100% (1)
- Instructions: Certification of Health Care Provider: Family and Medical Leave ActDocument5 pagesInstructions: Certification of Health Care Provider: Family and Medical Leave ActMichelleNo ratings yet
- Lilyasari2019 Article EconomicEvaluationOfSildenafilDocument9 pagesLilyasari2019 Article EconomicEvaluationOfSildenafilNajib Al FatinNo ratings yet
- Rifaximin Therapy For Patients With IrritableDocument18 pagesRifaximin Therapy For Patients With IrritableSalman AjaNo ratings yet
- Miniguia de EstudosDocument6 pagesMiniguia de EstudosMaykom LiraNo ratings yet
- Dissertation SalmonellaDocument7 pagesDissertation SalmonellaWriteMyPaperCoCanada100% (1)
- Anemia 130809044630 Phpapp01Document21 pagesAnemia 130809044630 Phpapp01Siddharth Das100% (1)
- T&L Wound Dressing Catalogue (New)Document6 pagesT&L Wound Dressing Catalogue (New)darknightuNo ratings yet
- Hemoperitoneum From Corpus Luteum Cyst Rupture in Pregnancy of Unknown LocationDocument4 pagesHemoperitoneum From Corpus Luteum Cyst Rupture in Pregnancy of Unknown Locationlina ukagoNo ratings yet
- Radiological Chest SignsDocument15 pagesRadiological Chest SignsEzekiel ArtetaNo ratings yet
- Real Time Health Monitoring System Through Iot Using SensorsDocument6 pagesReal Time Health Monitoring System Through Iot Using Sensorsقابوس الليثيNo ratings yet
- Defining The Practice of Medical TechnologyDocument47 pagesDefining The Practice of Medical TechnologyCharles Ian OliquinoNo ratings yet
- Holter Monitor RedactedDocument11 pagesHolter Monitor RedactedAnonymous f2WeA3No ratings yet
- Manuver Head Tilt-Chin Lift-Jaw ThrustDocument6 pagesManuver Head Tilt-Chin Lift-Jaw ThrustKevin CindarjoNo ratings yet
- Intra-Abdominal Infections: Resident's Lecture Edward L. Goodman, MD May 1, 2006Document36 pagesIntra-Abdominal Infections: Resident's Lecture Edward L. Goodman, MD May 1, 2006srweaverNo ratings yet
- Circulatory System: DR Rita Chávez Puente Cie-MgaDocument22 pagesCirculatory System: DR Rita Chávez Puente Cie-Mgarchavez0522No ratings yet
- 1st Internal Assessment Pharmacology 28.7.21 FinalDocument2 pages1st Internal Assessment Pharmacology 28.7.21 FinalSubhom MajumderNo ratings yet
- Case Study 1Document9 pagesCase Study 1andry natanel tonyNo ratings yet
- Coagulation of BloodDocument21 pagesCoagulation of BloodHery StiawanNo ratings yet
- Coding Clinic 2nd QTR 2021Document24 pagesCoding Clinic 2nd QTR 2021haru haroon100% (1)
- Courtney Connolly Critical Elements For Health Assessment Documentation HistoryDocument4 pagesCourtney Connolly Critical Elements For Health Assessment Documentation HistorycourtneyNo ratings yet