Professional Documents
Culture Documents
I. Demographic Data II. Chief Complaints Iii. History of Present Illness IV. Genogram V. Laboratory/Diagnostic Studies
I. Demographic Data II. Chief Complaints Iii. History of Present Illness IV. Genogram V. Laboratory/Diagnostic Studies
Uploaded by
mylene dabucolOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
I. Demographic Data II. Chief Complaints Iii. History of Present Illness IV. Genogram V. Laboratory/Diagnostic Studies
I. Demographic Data II. Chief Complaints Iii. History of Present Illness IV. Genogram V. Laboratory/Diagnostic Studies
Uploaded by
mylene dabucolCopyright:
Available Formats
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
I. DEMOGRAPHIC DATA
II. CHIEF COMPLAINTS
III. HISTORY OF PRESENT ILLNESS
IV. GENOGRAM
V. LABORATORY/DIAGNOSTIC STUDIES
a) Diagnostic Test
Computed Tomography (CT) Scan
Blood Test: Basic Metabolic Panel (BMP)
b) Date of Examination: November 22, 2021
Laboratory Normal Values Result Nursing
Significant
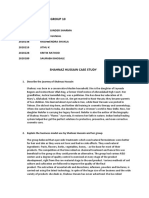
Computed
Tomography (CT)
Scan
• Indicates
Abdomen stability with aortic
(Transversal) dissection from
descending aorta
to common iliacs.
(Coronal)
LEVEL III CCMC-CN 1
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
(Sagittal)
Computed
Tomography (CT)
Scan
Brain • Scattered foci in
both the cerebral
and cerebellar
hemisphere
bilaterally,
LEVEL III CCMC-CN 2
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
indicates altered
sensory and
motor functions.
• Infarction on one
side, indicates for
brain ischemia.
Basic Metabolic
Panel
65 – 100 mg/dL 155 mg/dL • Increased sugar
Glucose 8 – 25 mg/dL 20 mg/dL in blood indicates
LEVEL III CCMC-CN 3
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
BUN 0.8 – 1.4 mg/dL 1.2 mg/dL body lacks
Creatinine 133 – 146 mEq/L 145mEq/L enough insulin.
Sodium 3.5 – 5.3 mEq/L 4.7 mEq/L
Potassium 97 – 110 mEq/L 100 mEq/L • above average
Chloride 18 – 30 mEq/L 20 mEq/L of urea nitrogen
Carbon dioxide and creatinine in
blood may
indicate of risk of
renal dysfunction.
• above average
of sodium
indicates risk for
hypertension
LEVEL III CCMC-CN 4
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
VI. ASSESSMENT: FUNCTIONAL HEALTH PATTERNS
a. Health-Perception Health Maintenance Pattern
b. Nutritional-Metabolic Pattern
c. Elimination Pattern
d. Activity-Exercise Pattern
e. Sleep-Rest Pattern
f. Cognitive Perceptual Pattern
g. Self-Perception-Self-Concept Pattern
h. Role-Relationship Pattern
i. Sexuality Reproductive Pattern
j. Coping and Stress Tolerance Pattern
k. Value-Belief Pattern
VII. ANATOMY AND PHYSIOLOGY
a. Macro anatomy
The brain is considered to be the most powerful organ as it controls thought, memory, emotion,
touch, motor skills, vision, breathing, temperature, hunger and every process that regulates our
LEVEL III CCMC-CN 5
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
body. It weighs about 3 pounds in average adult, and is composed of 60% fats, while the
remaining 40% is a combination of water, protein, carbohydrates and salts. It is enclosed within
the skull, which provides frontal, lateral and dorsal protection. The brain itself is a not a muscle.
It contains blood vessels and nerves, including neurons and glial cells. The brain can be divided
into the cerebrum, brainstem and cerebellum.
Cerebrum – The cerebrum (front of the brain) is the largest part of the brain that initiates
and coordinates movement and is also responsible in regulating the temperature.
Speech, judgment, thinking and reasoning, problem-solving, emotions and learning are
powered by the other areas of the cerebrum. Other functions relate to vision, hearing,
touch and other senses. The cerebrum has four sections, called lobes: frontal, parietal,
temporal and occipital. Each lobe serves specific functions.
o Frontal lobe – Is located in front of the head, and is the largest lobe of the brain.
Personality characteristics, decision-making and movement are said to be
associated with the frontal lobe. Recognition of smell usually involves parts of the
frontal lobe. It also contains Broca’s area, which is associated with speech ability.
o Parietal lobe – this is located in the middle part of the brain. The parietal lobe
facilitates a person’s ability to identify objects and understand spatial
relationships (where one’s body is compared with objects around the person). It
is also involved in interpreting pain and touch in the body. The Wernicke’s area is
found in the parietal lobe, which helps the brain understand spoken language.
o Temporal lobe – This lobe is found at the sides of the brain, temporal lobes are
involved in short-term memory, speech, musical rhythm and some degree of
smell recognition.
o Occipital lobe – this is located at the back part of the brain, that is involved with
vision.
Cerebellum – The cerebellum (also called as, “the little brain”) is located above the
brain stem and at the back portion of the head, below the temporal and occipital lobes. It
is responsible for coordinating voluntary muscle movements and to maintain posture,
balance and equilibrium.
LEVEL III CCMC-CN 6
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
Brain stem – The middle of the brain is called as the brainstem. It connects the
cerebrum with the
spinal cord. The
brainstem includes
the midbrain, the
pons and the
medulla. The
midbrain facilitates
several functions,
from hearing and
movement to
calculating responses
and environmental
changes. The pons is
the connection bet
ween the midbrain
and the medulla. It is
the origin for four of
the 12 cranial nerves, which enable a range of activities such as tear production,
chewing, blinking, focusing vision, balance, hearing and facial expression. The medulla
is located at the bottom of the brainstem, where the brain connects to the spinal cord.
Numerous functions of the medulla are essential for survival, these includes regulation of
many bodily activities, including heart rhythm, breathing, blood flow, and oxygen and
carbon dioxide levels. The medulla also produces reflexive activities such as sneezing,
vomiting, coughing and swallowing.
b. Micro anatomy
The Anterior Cerebral Artery (ACA), Middle Cerebral Artery (MCA), and the Posterior Cerebral
Artery (PCA) are the three main vessels that carry blood to the brain. Among these three
LEVEL III CCMC-CN 7
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
vessels, MCA is the commonly involves and is largest artery that supplies blood to a large
portion of the brain. It supplies blood to the frontal, temporal and parietal lobes, as well as deep
brain structures including the basal ganglia and intimal capsule. Occlusions of this vessel most
typically result in hemiplegia and sensory loss of the contralateral side of the body as well as
visual deficits, aphasia and unilateral neglect. Involvement of the PCA can result in visual
deficits, while involvement of the ACA can result in behavioral changes, contralateral weakness
and sensory loss, and incontinence. Strokes involving the vertebral-basilar circulation can also
occur and affect the cerebellum, brainstem, or both. Cerebellar strokes will commonly impair
balance and coordination.
c. Physiology
Cerebral blood flow (CBF) is the blood supply to the brain in a given period of time. In an adult,
CBF is typically 750 milliliters per minute or 15% of the cardiac output. This equates to an
average perfusion of 50 to 54 milliliters of blood per 100 grams of brain tissue per minute.
Arteries deliver oxygenated blood, glucose and other nutrients to the brain. Veins carry "used or
spent" blood back to the heart, to remove carbon dioxide, lactic acid, and other metabolic
products. Because the brain would quickly suffer damage from any stoppage in blood supply,
the cerebral circulatory system has safeguards including autoregulation of the blood vessels.
The failure of these safeguards may result in a stroke. CBF is tightly regulated to meet the
brain's metabolic demands. Too much blood (a clinical condition of a normal homeostatic
response of hyperemia) can raise intracranial pressure (ICP), which can compress and damage
delicate brain tissue. Too little blood flow (ischemia) results if blood flow to the brain is below 18
to 20 ml per 100 g per minute, and tissue death occurs if flow dips below 8 to 10 ml per 100 g
per minute. In brain tissue, a biochemical cascade known as the ischemic cascade is triggered
when the tissue becomes ischemic, potentially resulting in damage to and the death of brain
cells.
VIII. PATHOPHYSIOLOGY
a. Definition
LEVEL III CCMC-CN 8
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
In a schematic brain attack, there is disruption of the cerebral blood flow due to
obstruction of a blood vessel. This disruption in blood flow initiates a complex series of
cellular metabolic events referred to as ischemic cascade. The ischemic cascade begins
when cerebral blood flow falls to less than 25 mL/100 g/min. At this point, neurons can
no longer maintain aerobic respiration, which generates large amounts of lactic acid,
causing a change in the pH level. This switch to the Jess efficient anaerobic respiration
also renders the neurons incapable of producing sufficient quantities of adenosine
triphosphate (ATP) to fuel the depolarization processes. Thus, the membrane pumps
that maintain electrolyte balances begin to fail and the cell cease to function.
b. Risk Factors
The major risk factors for this are people who have a high blood pressure,
diabetes, those who have a heart and blood vessel diseases, High LDL cholesterol and
those who have been smoking. Arteriovenous malformations (AVM) and brain
aneurysms are also a major risk. AVMS are tangles of poorly formed arteries and veins
that can break open in the brain.
c. Diagnostics Studies and Its Possible Results
A diagnostic of cerebrovascular accident or stroke should be made based on the results
of multiple tests including:
Computed tomography (CT) uses X-rays to take clear, detailed pictures of your
brain. It is often done right after a stroke is suspected. A brain CT scan can show
if there is bleeding in the brain or damage to the brain cells from a stroke.
Magnetic resonance imaging (MRI) uses magnets and radio waves to create
pictures of your brain. An MRI may be used instead of—or in addition to—a CT
scan to diagnose a stroke. This test can detect changes in brain tissue and
damage to brain cells.
LEVEL III CCMC-CN 9
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
Other imaging tests to look for narrowed blood vessels in the neck or an
aneurysm or tangled blood vessels in the brain.
d. Medical-Surgical Management
Perioperative Phase
To prepare for the surgery, tests are ordered by the doctor several days before the
procedure. These tests include blood tests, chest x-ray, electrocardiogram as well as a
brain scan by MRI, CT, or PET.
The patient should not take anti-inflammatory medicines or blood thinners, for at least one
week before the procedure.
The patient should stop smoking, chewing tobacco, and drinking alcohol for 1-2 weeks.
The patient should not eat or drink anything for at least 8 – 12 hours before the procedure.
The patient’s head is shaved over the area where the craniotomy will be done.
Intraoperative Phase
Control of bleeding
Identification of injuries
Control of contamination
Reconstruction (if possible)
Once anesthesia takes effect and the patient is asleep, the head is help in a fixed position
using a 3-pin skull fixation device.
Post-operative
Keep the incision clean. Craniotomy incisions are usually closed with sutures or surgical
staples.
The patient is taken to the recovery room and watched closely. The vital signs (that is,
temperature, blood pressure, heart rate, and breathing) are monitored.
Watched closely. The breathing tubes and catheters are usually left in place and a drip
may be put into a vein to give fluids.
LEVEL III CCMC-CN 10
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
Watch the incision for signs of infection or complications.
Control Pain.
Gradually return to activity.
e. Pharmacological Management
1. Supportive manage - airway, temperature, blood pressure, cardiac assessment
2. Thrombolysis - intravenous/intra arterial
3. Antiplatelet drugs
4. Anticoagulant drugs
5. Hemodilution, vasodilators, and induced hypertension
6. Neuroprotective agents
f. Diagram
LEVEL III CCMC-CN 11
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
IX. SUMMARY OF FINDINGS
Cues
Legend
ROS ROS
-forward flexed posture with kyphosis and forward head
*
-Vital signs:
BP 126/70 mmHg, P 74 bpm, R 16 rpm, T 98° F (36.7° C), wt 274 lb
*
(124.28 kg), ht 5 ft 10 inches, BMI 39.34 - Obese
-no skin lesions presented
exhibited LLE internal rotation and foot drop on the left.
*
-unable to initiate a step with his LLE
*
-decreased ROM of left dorsiflexion
*
-decreased balance. decreased gait velocity
*
-decreased step length bilaterally
*
-decreased weight shift to the left
*
-displayed good balance in sitting in that he was able to remain seated
without loss of balance for an unspecified amount of time
-in standing, able to balance with a FWW and standby assistance,
however he leaned to the right during dynamic activities.
-displayed short-term memory loss and confusion regarding sequence of
*
recent events
-left lower extremity slightly cold and stiffness noted
*
-near vision, able to read magazine at 13 inches with eyeglasses
*
ASSESSMENT ASSESSMENT
LEVEL III CCMC-CN 12
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
When asked about his present condition, the patient was very motivated
to regain independence.
He is aware of his current health situation that he can recover from it as
long as he complies with every order, medication and instruction given
by the doctor.
The patient describes a healthy diet as being able to eat lots of fruits and
vegetables.
The client drinks more than 8 glasses of water per day.
Following his stroke, prior to acute PT rehabilitation, the patient had
been maximum assist of two to total assist with Hoyer lift in all transfers
while residing at the nursing home.
he displayed some short-term memory loss and confusion regarding the
* sequence of recent events.
Level of Anxiety- Moderate
Support system- High
Level of self-worth- High
He lived alone in an urban community with his farm and managing his
farm independently.
He start loses his sex drive and have erectile dysfunction when he was
* 48 or 49.
The patient is easily became tearful and emotional at times, and had a
history of depression following his CVA.
He also stated that no matter what difficulties or problems arise,
everything will be fine because he places God at the center of
everything.
Lab. Findings Lab. Findings
Scattered foci in both the cerebral and cerebellar hemisphere bilaterally,
* indicate altered sensory and motor functions.
Infarction on one side, indicates for brain ischemia
*
LEVEL III CCMC-CN 13
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
Glucose level 155 mg/dL, Increased sugar in blood indicates body lacks
enough insulin.
ACTUAL NSG DX RISK/POTENTIAL NSG DX WELLNESS NSG DX
(ABC, MASLOWS SAFETY
HIERARCHY OF NEEDS)
Ineffective Tissue Perfusion Risk for Injury Readiness for Spiritual Being
related to insufficient blood
flow to organs and tissues as
evidenced by changes in
speech, difficulty swallowing,
and motor weakness.
Impaired Physical Mobility Risk for Caregiver Role Strain Readiness for Enhanced
related to the involvement of
Family Coping
neuromuscular weakness as
evidenced by weakness
hemiplegia with involvement of
upper and lower extremities.
Disturbed Sensory Perception Risk for Falls Health Seeking Behaviour
related to altered sensory
reception as evidenced by
aphasia, and dysphagia.
Self – Care Deficit Risk for Unstable Blood
Glucose
Disturbed Sleep Pattern
LEVEL III CCMC-CN 14
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
X. DRUG STUDY
LEVEL III CCMC-CN 1
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
XI. NURSING CARE PLAN
a. PREOPERATIVE
NURSING
DAT SCIENTIFIC GOAL OF NURSING EVALUATI
CUES DIAGNOS RATIONALE
E BASIS CARE INTERVENTION ON
IS
Nov Subjectiv Risk for -High blood After 8 1. Assist the 1. These risk After 8
emb e: prone pressure (HBP) hours of patient in factors have been hours of
er Patient behaviou or hypertension nursing identifying shown to nursing
24, complain r means high interventio modifiable risk contribute to interventi
202 ed of related pressure(tensio ns ,the pat factors like diet hypertension ons ,the
1
dizzines to lack n) in the ,the high in sodium, 2. Lack of patient
s before of arteries. patient saturated fats and cooperation is was able
admissio knowledg Arteries are will cholesterol. common reason for to
n. e about vessels that verbalize 2. Reinforce the failure of verbalize
the carry blood understandi importance of antihypertensive understand
disease. from the ng of the adhering to therapy ing of the
pumping heart disease treatment regimen 3. Decreases disease
to all the process and and keeping follow peripheral venous process
LEVEL III CCMC-CN 1
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
tissues and treatment up appointments pooling that may and
organs of the regimen 3. Suggest frequent be potentiated by treatment
body. High position vasodilators and regimen
blood pressure changes ,leg 4. Caffeine is a
does not mean exercises when cardiac stimulant
excessive lying down. and may adversely
motional 4. Encourage affect cardiac
tension ,althou patient to decrease function
gh emotional or eliminate
tension and caffeine like in
stress can tea, coffee ,cola
temporarily and chocolates..
increase blood
pressure.
Normal blood
pressure is
below
120/80;blood
pressure
LEVEL III CCMC-CN 2
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
between
120/80and
139/89 is
called
"prehypertensio
n".
NURSIN
NURSING
G EVALUATI
DATE CUES SCIENTIFIC BASIS GOAL OF CARE INTERVEN RATIONALE
DIAGN ON
TION
OSIS
Novem Subject Decrea Cardiac output is the STG:At the end of 30- 1. Assess At the
ber 24, ive: amount of blood that the min Nursing
sed ed for and end of 8-
heart pumps in one minute.
2021 episodes Interventions, the
It's the product of heart rate
document hour
Cardiac client will be able to: 1.
of (the number of heartbeats the ff: Nursing
blacking Output per minute) and stroke - Cerebral
o Mental Intervent
out related
volume (the amount of Demonstratehemodyna perfusion is
Status ions, the
blood pumped per beat), micstability directly r/t
resulting Mental goal was
to and it's usually given in a (bloodpressure
from cardiac
value of liters/minute. andcardiac output)by partially
LEVEL III CCMC-CN 3
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
hypoten altered Normal cardiac output is 20% Status output and met as
typically between 4 and 8 –
sion. o Lung aortic evidenced
heart liters per minute, 30% asrevealed in
and decreased cardiac
sounds perfusion by:
rate thecardiac monitor
output means the output o Blood pressure and - PR =
and is lower than 4 LTG:At the end of 8- Pressure is -Cardiac
liters/minute. hourNursingInterventi
rhythm o Heart influenced monitorin
https:// ons, theclient will be
blog.prepscholar.com/ Sounds by hypoxia g
ableto:
decreased-cardiac-output- o Urine and revealed
care-plan Output electrolyte slight
Demonstratehemodyna
o and acid-base disturban
micstability
(Bloodpressure Peripheral variation ce
andcardiac output)by Perfusion - Crackles
31%-80% asrevealed in may develop Endorsed
thecardiac monitor 2. Kept to the
r/t
client on alterations next
Manifestabsence bed in in MI shift NOD
of angina
Semi- - for
fowler’s Hypotension further
and r/t intervent
administer ions and
LEVEL III CCMC-CN 4
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
ed high hypoperfusion revisions
flow O2 , vagal of NCP
via nasal stimulation, for
cannula dysrhythmias, continuit
or y of
ventricular care
3. Monito dysfunction
red and may occur
assessed
angina for -Bradycardia
type, may be
severity present
and because of
duration vagal
stimulation
4. Adminis or conduction
tered disturbances
beta- r/t area of
blockers MI
and
LEVEL III CCMC-CN 5
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
inotropin - Urine
agents and output
monitored >0.5ml/kg/hr
their may reflect
effects reduced renal
perfusion and
glomerular
filtration as
a result of
reduced
cardiac
output
- Decread may
indictae a
decreased
cardiac
output
2. Facilitate
oxygenation
LEVEL III CCMC-CN 6
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
3. Angina
indicates
myocardial
ischemia,
which may
decrease
cardiac
output
4. To
determine
effects of
therapy
NURSING NURSING
GOAL OF EVALUATIO
DATE CUES DIAGNOSI SCIENTIFIC BASIS INTERVENTIO RATIONALE
CARE N
S N
Novemb Subjective: Risk for Where your stroke Short-term Independent: • To Short
er 24, residual falls occurred in the brain will Goal: • Assessed assess term: Goal
2021 weakness determine the location of
related After two muscle degree of met. The
LEVEL III CCMC-CN 7
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
of his left to your weakness. Injury to (2) hours strength, risk of patient
lower decreased the left side of the brain, of nursing gross and falling, has an
which controls language
extremity lower interventi fine motor altering increased
and speaking, can result in
(LLE) and extremiti on, the coordination coordinatio in lower
right-sided weakness. Left-
decrease es patient • Evaluated n, gait and extremitie
sided weakness results
functional strength from injury to the right side will have client’s balance • s strength
independe of the brain, which controls an cognitive To appraise as
nce nonverbal communication increased status ability to evidenced
and certain behaviors. in lower • Reviewed perceive by
https://www.stroke.org/
extremitie medication own Lovett’s
en/about-stroke/effects-of-
s strength regimen and limitations Scale of
stroke/physical-effects-of-
as how it or UR = 5/5,
stroke/physical-impact/
hemiparesis
evidenced affects recognize UL = 5/5
by patient. danger LR = 5/5,
Lovett’s Monitor • LL = 5/5
Scale of drug’s Furosemide (normal
UR = 5/5, effects or causes strength)
UL = 5/5 side effects headache, Long term:
LR = 5/5, • Instructed weakness, There is
LEVEL III CCMC-CN 8
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
LL = 5/5 the relative confusion, no noted
Long-term to intensify balance and injury
Goal: patient gait caused by
After two supervision disturbance falling
(2) days • Encouraged s • To during her
of nursing patient to monitorsafe stay in
interventi exercise or ty and to the
on, the gradually avoid hospital
patient mobilize her falling • and the
will not lower To help patient is
experience extremities strengthen now
falling such as musculoskel discharged
performing et al .
flexionextens strength
ion exercise, of the
sittingstandi lower
ng exercise extremities
and trying to • To
make few strengthen
LEVEL III CCMC-CN 9
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
small steps physical
alone support and
• Assisted help in
patient in rehabilitat
treatment ion
regimen like • To
early minimize
ambulation • the risk of
Kept side fall from
rails up the bed
b. INTRAOPERATIVE
c. POSTOPERATIVE
NCP # 1
NURSING SCIENTIFIC GOAL OF NURSING
DATE CUES RATIONALE EVALUATION
DIAGNOSIS BASIS CARE INTERVENTION
Novembe Subjective: Ineffective Ineffective After 8 hours Independent After 8 hours
r 24, 2021 “Labad kayo Tissue tissue of Nursing Interventions: of Nursing
akong ulo, ug Perfusion perfusion intervention, 1. Assess for 1. Particular intervention,
nakabati kog related to defines the the patient signs of clusters of the patient
LEVEL III CCMC-CN 10
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
pamoypoy sa insufficient lack of will be able decreased signs and was able to
akong blood flow to oxygenated to engage in tissue symptoms engage in
kalawasan,” as organs and blood flow to actions to perfusion. occur with actions to
verbalized by the tissues as areas of the improve differing improve tissue
patient. evidenced by body. Proper tissue causes. perfusion.
changes in perfusion is perfusion. Evaluation
Objective: speech, detrimental to provides a
Motor difficulty the function of baseline for
weakness swallowing, organs and future
Slurred and motor body systems comparison
speech weakness. as organs and 2. Assess for .
Dysphagia tissues that probable 2. Early
V/S: are not contributing detection of
BP: 126/70 perfusing will factors the source
mmHg die. related to facilitates
PR: 74 bpm Decreased temporarily quick,
RR: 16 bpm tissue impaired effective
Temp: 36.7⁰C perfusion can arterial blood manageme
be temporary, flow. nt.
with few or
minimal 3. Review 3. Blood
LEVEL III CCMC-CN 11
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
consequences laboratory clotting
to the health of data if studies are
the patient, or anticoagulan being used
it can be more ts are to conclude
acute or utilized for or make
protracted, treatment. sure that
with potentially clotting
destructive factors stay
effects on the within
patient. When therapeutic
diminished 4. Submit levels.
tissue patient to 4. This
perfusion diagnostic provides
becomes testing as proper
chronic, it can indicated. assessmen
result in tissue t and
or organ identificatio
damage or n of
death. 5. Note urine appropriate
output. intervention
Source: s.
LEVEL III CCMC-CN 12
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
Ineffective 5. Reduce
Tissue renal
Perfusion – perfusion
Nursing 6. Promote may take
Diagnosis & active/passiv place due
Care Plan - e ROM to vascular
Nurseslabs exercises. occlusion.
6. Exercise
prevents
venous
7. Position stasis and
patient further
properly in a circulatory
semi- compromis
Fowler’s to e.
high-
Fowler’s as 7. Upright
tolerated. positioning
8. Observe for promotes
signs of improved
deep vein alveolar
LEVEL III CCMC-CN 13
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
thrombosis, gas
including exchange.
pain,
tenderness, 8. Thrombosis
swelling in with clot
the calf and formation is
thigh, and usually first
redness in detected as
the in the swelling of
extremities. the
9. Educate involved
patient about leg and
nutritional then as
status and pain.
the
importance
of paying 9. Malnutrition
special contributes
attention to to anemia,
obesity, which
malnutrition, further
LEVEL III CCMC-CN 14
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
and compounds
hyperlipidem the lack of
ia. oxygenatio
n to
tissues.
Obese
patients
encounter
poor
circulation
10. Teach in adipose
patient to tissue,
recognize which can
the signs create
and increased
symptoms hypoxia in
that need to tissue.
be reported 10. Early
to the nurse. assessmen
t facilitates
Dependent immediate
LEVEL III CCMC-CN 15
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
Interventions: treatment.
11. Check for
optimal fluid
balance.
Administer
IV fluid as
ordered. 11. Sufficient
fluid intake
maintains
adequate
filling
pressures
and
optimized
cardiac
output
needed for
tissue
perfusion.
LEVEL III CCMC-CN 16
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
NCP # 2
NURSING SCIENTIFIC GOAL OF NURSING EVALUATIO
DATE CUES RATIONALE
DIAGNOSIS BASIS CARE INTERVENTION N
Novembe Subjective: Impaired A stroke is After 8 hours Independent After 8 hours
r 24, 2021 “Lisud ilihok,” Physical also referred to of Nursing Intervention: of Nursing
as verbalized Mobility as a brain intervention, 1. Assess 1. To identify intervention,
by the patient. related to the attack, and it the patient will functional strengths, the patient will
involvement of occurs when a be able to ability or weaknesses be able to
Objective: neuromuscula blood vessel improve extent of and can improve
Exhibited r weakness as leading to the strength and initial provide strength and
LLE evidenced by brain ruptures function of the damage by information function of the
internal weakness or gets affected body way of through the affected body
rotation hemiplegia blocked due to part or regular, recovery. part or
and foot with plaque compensation classified by 2. Lowering compensation
drop on involvement of deposits. . scale of 0-4. the risk of .
the left upper and When plaque 2. Change trauma/isch
Unable to lower accumulates position at emia area
initiate a extremities. on the wall of least every 2 damaged
step with arteries, it is hours (back, tissue and
LEVEL III CCMC-CN 17
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
his LLE known as oblique) and minimize
Decrease arthrosclerosis if possible, pressure
d ROM of . Impaired more often if sores.
left physical placed in a
dorsiflexio Mobility may compromise 3. Helps to
n be related to d position. maintain a
Decrease neuromuscular 3. Put on the functional
d balance, impairment, tummy one hip
and gait decreased or two feet a extension.
velocity muscle day if the
Decrease strength and patient can 4. Minimizing
d step control, tolerate it. muscle
length possibly 4. Perform the atrophy
bilaterally, evidenced by exercise of helps
and generalized active and increase
weight weakness, passive circulation.
shift to the inability to range of 5. To prevent
left. perform motion. contractures
V/S: desired 5. Chock limb and
BP: activities or in a facilitates
126/70 movements. functional their role if it
LEVEL III CCMC-CN 18
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
mmHg position, use works again.
PR: 74 Source: Nurse a board foot
bpm Health (foot board)
RR: 16 Guides : during the
bpm Impaired period of
Temp: Physical paralysis
36.7⁰C Mobility related flaccid,
to Stroke maintaining
a neutral 6. During
head paralysis
position. flaccid, use
6. Use the of buffers
support arm can reduce
when the the risk of
patient is an shoulder
upright arm
position, as syndrome.
indicated.
7. Maintaining
7. The position a functional
of the knee position.
LEVEL III CCMC-CN 19
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
and hip is in
extension
position.
Collaborative
Intervention
8. Collaboratio 8. A special
n or program can
consultation be
with developed
physiotherap to determine
ists actively or find the
resistive patient’s
exercises needs.
and
ambulation.
LEVEL III CCMC-CN 20
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
NCP # 3
NURSING NURSING
GOAL OF EVALUATI
DATE CUES DIAGNOSI SCIENTIFIC BASIS INTERVENTI RATIONALE
CARE ON
S ON
Novemb Subjective Disturbed This pertains to an After 8 1. Establish 1. Even an After 8 hours
er 24, Cues: Sensory alteration in the response hours of and unrespon of nursing
2021 “Maglisud man Perception stimuli, which can be either nursing maintain sive intervention,
siyag storya related to a weaker or a stronger interventio communic patient the patient
pa,” as altered response to them. n, the ation with may be was able to
verbalized by sensory Cerebrovascular accident, patient will the able to regain usual
the patient’s reception also known as stroke, be able to patient. hear. level of
neighbor. as cerebral infarction, brain regain 2. Protect perceptual
LEVEL III CCMC-CN 21
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
evidenced attack, is any functional or usual level from 2. Promotes functioning.
Objective by structural abnormality of the of extreme patient
Cues: aphasia, brain caused by perceptual temperatur safety,
dense and pathological condition of the functionin es, and reducing
left dysphagia. cerebral vessels of the g. assess risk of
hemiple . entire cerebrovascular environme injury.
gia with system. It is the sudden nt for
involve impairment of cerebral hazards.
ment of circulation in one or more of 3. Observe 3. Individual
upper the blood vessels supplying behavioral responses
and the brain. One of the signs responses: are
lower and symptoms of stroke is crying, variable,
extremiti hemiparesis. Hemiparesis inappropri but
es is weakness on one side of ate affect, commonal
aphasia the body. You can still agitation, ities such
dysphag move the affected side of hostility, as
ia. your body, but with reduced hallucinati emotional
V/S: muscular strength. on. lability,
BP: 126/70 Treatment is focused on lowered
mmHg improving feeling and motor frustration
PR: 74 bpm skills, allowing you to better threshold,
LEVEL III CCMC-CN 22
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
RR: 16 bpm manage your daily living. apathy,
Temp: 36.7⁰C and
Source: impulsive
https://www.stroke.org/we- 4. Eliminate ness may
can-help/survivors/stroke- extraneou complicat
recovery/post-stroke- s noise e care.
conditions/physical/ and stimuli 4. Reduces
hemiparesis as anxiety
necessary. and
exaggerat
ed
emotional
responses
and
5. Speak in confusion
calm, associate
comforting d with
, quiet sensory
voice, overload.
using short 5. Patient
sentences. may have
LEVEL III CCMC-CN 23
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
Maintain limited
eye attention
contact. span or
problems
6. Ascertain with
patient’s comprehe
perception nsion.
s. Reorient
patient 6. Assist
frequently patient to
to identify
environme inconsiste
nt, staff ncies in
and reception
procedure and
s. integratio
n of
stimuli
and may
reduce
perceptua
LEVEL III CCMC-CN 24
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
7. Stimulate l distortion
sense of of reality.
touch. 7. Aids in
Give retraining
patient sensory
objects to pathways
touch, and to
hold. integrate
reception
and
interpretat
8. Note ion of
inattention stimuli.
to body
parts, 8. Agnosia,
segments the loss of
of comprehe
environme nsion of
nt, lack of auditory,
recognition visual, or
of familiar other
LEVEL III CCMC-CN 25
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
objects/per sensation
sons. s, may
lead result
to
unilateral
neglect,
inability to
recognize
environm
ental
cues,
considera
ble self-
care
deficits,
and
disorientat
ion or
bizarre
behavior.
LEVEL III CCMC-CN 26
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
XII. DISCHARGE PLAN
a. Demographic Data
Name
Age
Sex
Civil Status
Educational Attainment
Address
Significant Other
Medical Diagnosis
b. General Objective
After 3 days of nurse-patient interaction, the patient will be able to acquire the desired
wellness on the therapeutic management of his health condition.
c. Specific Objectives
After 3 days of nurse-patient interaction, the patient will achieve:
- The understanding of individual treatment regimen and the need for frequent
monitoring.
- Improved ability to participate in the desired activities but avoid rigorous ones.
- The preparedness for collaboration between family and health professionals that
improves functional outcomes and quality of care.
d. Medications
NAME OF DOSAGE FREQUEN THERAPEU SIDE EFFECTS HEALTH
DRUG CY TIC USE EDUCATION
Simvastatin 40 mg IV Once a day Reduce the Increased serum -Educate the
(Zocor) risk of total transaminase, patient that
LEVEL III CCMC-CN 1
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
mortality by anemia, the 40 mg is
reducing constipation, indicated
CHD deaths abdominal pain, dose for his
and reduce flatulence, condition and
the risk of dyspepsia, that it should
non-fatal diarrhea, be take
myocardial nausea, acid religiously.
infarction, regurgitation,
stroke, and vomiting, -Continuous
the need for headache, monitoring of
revasculariza paranesthesia, the patient’s
tion dizziness and vital signs
procedures peripheral and possible
in patients at neuropathy adverse
high risk of effect.
coronary
events.
NAME OF DOSAGE FREQUEN THERAPEUTI SIDE EFFECTS HEALTH
DRUG CY C USE EDUCATIO
N
Labetalol Initial: Initial: over Labetalol Fatigue, -Tell the
(Normodyne 20mg IV 2 minutes injections are asthenia, patient and
Trandate) bolus indicated to dizziness, the family
Additional: control blood drowsiness, that he may
Additio- Every 10 pressure in insomnia, feel dizzy
nal: minutes severe vasoconstriction, when
40-80 mg hypertension. bradycardia, starting the
IV They are nausea, therapy.
indicated diarrhea,
alone or in
LEVEL III CCMC-CN 2
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
combination rash and pruritus -Instruct the
with patient to
antihypertensi immediately
ves. report
adverse
effects,
such as
easy
bruising,
bleeding or
respiratory
problem.
NAME OF DOSAGE FREQUEN THERAPEUTIC SIDE HEALTH
DRUG CY USE EFFECTS EDUCATION
Alteplase 0.9 Every hour Indicated for cerebral Educate the
(Cathflo mg/kg to patient hemorrhage, client about
Activase) maximum experiencing cerebral the
dose of Acute Ischemic edema, medication
90 mg IV Cerebrovascular hypotension, and its
bolus Accident. This is bradycardia, benefits
also indicated for nausea,
use in acute vomiting, GI Monitor for
myocardial infarc bleeding, possible GI
tion for the flushing and bleeding,
reduction on bruising sepsis and
incidence venous
of heart failure. thrombosis
then report
immediately.
LEVEL III CCMC-CN 3
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
e. Environment
- Provide an environment conducive to the health condition of the patient.
- Make sure to clean the surroundings and practice proper hygiene.
f. Treatment
- Offer physical therapy for improving strength and walking
- Make an appointment for the follow up care
- Undergo speech therapy to practice talking and swallowing
g. Health Teaching
-Provide information regarding any required changes in pain control or management.
-Instruct the patient and family to avoid touching the incision as much as possible.
Do not put any medications or other skin products on the incision unless instructed.
-Inform that the patient cannot drive for 2 to 3 weeks or until the doctor approves for it.
h. Observable Signs and Symptoms
- Nausea
- Fatigue
- Constipation
- Fluid retention
- Heartburn
i. Diet
- The patient can eat a normal and nutritious diet. If the stomach is upset, try bland, low-
fat foods like plain rice, broiled chicken, toast, and yogurt.
- Avoid alcoholic drinks unless the doctor approves.
- If the patient didn’t have a bowel movement after a couple of days, ask the doctor
about taking a mild laxative.
j. Spiritual Care
LEVEL III CCMC-CN 4
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
Encourage the patient and family members to express their feelings, fears and doubt.
Pray and ask for continuous healing from God. Be thankful for daily guidance and
protection.
LEVEL III CCMC-CN 5
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
References:
Bawazeer, A. (n.d.). Ischemic stroke: Radiology case. Radiopaedia Blog RSS. Retrieved
November 23, 2021, from https://radiopaedia.org/cases/ischaemic-stroke-1.
Case study : Normal CT brain with contrast :: How to report. RadioMind. (n.d.). Retrieved
November 23, 2021, from https://www.radiomind.org/2019/02/case-study-normal-ct-brain-
with.html.
Drugbank Online. Labetalol. Retrieved from: https://go.drugbank.com/drugs/DB00598
Ineffective Tissue Perfusion Nursing Diagnosis & Care Plan. (n.d.). Retrieved from
https://rnlessons.com/ineffective-tissue-perfusion/
Katague, D. B. (1970, January 1). The basic metabolic panel blood test. The Basic Metabolic
Panel Blood Test. Retrieved November 23, 2021, from
http://livinginmarinduquephilippines.blogspot.com/2017/02/the-basic-metabolic-panel-blood-
test.html.
MIMS.Simvastatin Generic Medical Info. Retrieved from:
mims.com/philippines/drug/info/simvastatin?mtype=generic
Ogbru, O (n/a). Alteplase ( TPA, ACTIVASE, CATHFLO ACTIVASE). MedicineNet. Retrieved
from:
https://www.medicinenet.com/alteplase/article.htm#what_is_alteplase_tpa_activase_cathflo_acti
vase
(PDF) duplication of the inferior vena cava: A rare case. (n.d.). Retrieved November 23, 2021,
from
https://www.researchgate.net/publication/335707738_Duplication_of_The_Inferior_Vena_
Cava_A_Rare_Case.
LEVEL III CCMC-CN 6
CEBU TECHNOLOGICAL UNIVERSITY
In consortium with
CEBU CITY MEDICAL CENTER- COLLEGE OF NURSING
RobHolland. Labetalol. Retrieved from:
http://www.robholland.com/Nursing/Drug_Guide/data/monographframes/L001.html
RxList (2020). Zocor. Retrieved from: https://www.rxlist.com/zocor-drug.htm#description
Smeltzer, S. C., Bare, B. G., Hinkle, J. L., & Cheever, K. H. (2010). Brunner and Suddarth's
Textbook of Medical-Surgical Nursing. Philadelphia: Wolters Kluwer Health /Lippincott
Williams & Wilkins.
The proximal to the aneurysm aortic ... - researchgate.net. (n.d.). Retrieved November 23, 2021,
from https://researchgate.net/figure/The-proximal-to-the-aneurysm-aortic-segment-is-an-
aneurysm-This-patient-has-no-aortic_fig3_10836467
Wayne, G. (2019). Ineffective Tissue Perfusion Nursing Care Plan. Retrieved from
https://nurseslabs.com/ineffective-tissue-perfusion/
www.zeauw.nl, Z.-. (n.d.). CT abdomen general. Startradiology. Retrieved November 23, 2021,
from https://www.startradiology.com/internships/general-surgery/abdomen/ct-abdomen-
general/.
Yew, K. S., & Cheng, E. M. (2009, July 1). Acute stroke diagnosis. American Family Physician.
Retrieved November 23, 2021, from https://www.aafp.org/afp/2009/0701/p33.html.
LEVEL III CCMC-CN 7
You might also like
- Too Good To Be Truth PDFDocument84 pagesToo Good To Be Truth PDFivica_putNo ratings yet
- A Case Presentation of Diabetes Mellitus Type 2 Uncontrolled Non-Healing WoundDocument67 pagesA Case Presentation of Diabetes Mellitus Type 2 Uncontrolled Non-Healing Woundashamy acolNo ratings yet
- Medical Technologist-On-Duty: Myrna N. Caranto, RMT Brenda I. Rosuman, MD, FPSPDocument9 pagesMedical Technologist-On-Duty: Myrna N. Caranto, RMT Brenda I. Rosuman, MD, FPSPJeng HidalgoNo ratings yet
- SWOT Analysis For Covid-19 Impact: InitiativesDocument2 pagesSWOT Analysis For Covid-19 Impact: InitiativesRaajha MunibathiranNo ratings yet
- 4 - Maintain and Repair Computer Systems and NetworksDocument7 pages4 - Maintain and Repair Computer Systems and NetworksJohnny Pancito RodriguezNo ratings yet
- Pochhacker - Getting Organized in Community InterpretingDocument16 pagesPochhacker - Getting Organized in Community InterpretingMaria Aguilar100% (7)
- Chronic Kidney Disease Secondary To Type 2 Diabetes MellitusDocument84 pagesChronic Kidney Disease Secondary To Type 2 Diabetes Mellituswar5No ratings yet
- NCPDocument3 pagesNCPErica Denice CastilloNo ratings yet
- Acute Vs Chronic Renal FailureDocument7 pagesAcute Vs Chronic Renal FailurePellan Rhey CapuyanNo ratings yet
- UNIT 1 Reaction PaperDocument3 pagesUNIT 1 Reaction PaperDeng Navarro PasionNo ratings yet
- Drug StudyDocument3 pagesDrug StudyGail SantosNo ratings yet
- San Luis, Trio - ActivityDocument4 pagesSan Luis, Trio - ActivityTrio San Luis100% (1)
- NCPDocument10 pagesNCPCristina L. JaysonNo ratings yet
- Technology Good or BadDocument3 pagesTechnology Good or BadRohit Gupta100% (1)
- Evidence-Based Nursing: I. Clinical QuestionDocument4 pagesEvidence-Based Nursing: I. Clinical QuestionRay Jorge MarmetoNo ratings yet
- Assessment Nursing Diagnosis Background Knowledge Planning Intervention Rationale Evaluation Subjective: Short Term: Independent: IndependentDocument4 pagesAssessment Nursing Diagnosis Background Knowledge Planning Intervention Rationale Evaluation Subjective: Short Term: Independent: IndependentAlyssa Marie SantosNo ratings yet
- 5 Case Study Proper and History of Present IllnessDocument4 pages5 Case Study Proper and History of Present IllnessRegiena TamargoNo ratings yet
- FractureDocument71 pagesFractureRegime San Juan AtienzaNo ratings yet
- Week 9: Course Task-Case Analysis Renal DisordersDocument4 pagesWeek 9: Course Task-Case Analysis Renal DisordersBELTRAN, JEANNE MAURICENo ratings yet
- E000779 FullDocument19 pagesE000779 Fullmartina silalahiNo ratings yet
- Operating Room Write UpDocument2 pagesOperating Room Write UpEnrico Sapitula Del RosarioNo ratings yet
- What Is Prednisolone?Document12 pagesWhat Is Prednisolone?Chandni SeelochanNo ratings yet
- Philippine Nursing Law of 2002 Ra # 9173Document15 pagesPhilippine Nursing Law of 2002 Ra # 9173Michael Maunda AmpuanNo ratings yet
- NCM 107-A # 2Document171 pagesNCM 107-A # 2Contessa GabrielNo ratings yet
- Project Proposal-HcfsDocument2 pagesProject Proposal-Hcfsapi-234337058No ratings yet
- Acute Sinusitis 08Document2 pagesAcute Sinusitis 08ativonNo ratings yet
- Journal Surg Ward BorjaDocument4 pagesJournal Surg Ward BorjaYana PotNo ratings yet
- Surgical Ward JournalDocument6 pagesSurgical Ward JournalMa Genille Samporna SabalNo ratings yet
- Cagayan Valley Center For Health Development: Dr. Jose Ildefonso B. Costales JRDocument4 pagesCagayan Valley Center For Health Development: Dr. Jose Ildefonso B. Costales JRKeith Clarence BunaganNo ratings yet
- Test - Management 443 Chapter 5 - QuizletDocument3 pagesTest - Management 443 Chapter 5 - Quizletايهاب غزالةNo ratings yet
- Hemo Glucose TestDocument3 pagesHemo Glucose TestrocheNo ratings yet
- Chapter 1-3Document27 pagesChapter 1-3JellyAnnGomezNo ratings yet
- Hildegard Peplau Theory of Interpersonal RelationsDocument1 pageHildegard Peplau Theory of Interpersonal RelationsTADZMALYN JINANGNo ratings yet
- Case Study CovidDocument6 pagesCase Study CovidAngel Faith TirolNo ratings yet
- Study Questions: Burn InjuriesDocument2 pagesStudy Questions: Burn InjuriesBELTRAN, JEANNE MAURICENo ratings yet
- TCW (Mancera, Dariano, Solsona)Document3 pagesTCW (Mancera, Dariano, Solsona)Vince ManceraNo ratings yet
- Osteogenesis ImperfectaDocument52 pagesOsteogenesis ImperfectaTrias AdnyanaNo ratings yet
- Case Scenario Drug Study - VicenteDocument4 pagesCase Scenario Drug Study - VicenteLouraine VicenteNo ratings yet
- Leg 1 A NCM 107-LMRDocument4 pagesLeg 1 A NCM 107-LMRAleli DoNo ratings yet
- Epidemiology and Pathophysiology of Colonic Diverticular DiseaseDocument8 pagesEpidemiology and Pathophysiology of Colonic Diverticular DiseaseAnonymous Hz5w55No ratings yet
- No. 9 Legal-Responsibility-Of-NurseDocument23 pagesNo. 9 Legal-Responsibility-Of-NursePawan BatthNo ratings yet
- VMGO CompletedDocument15 pagesVMGO CompletedShela RamosNo ratings yet
- Assessment Planning Intervention Rationale EvaluationDocument2 pagesAssessment Planning Intervention Rationale EvaluationIrish Jane GalloNo ratings yet
- NCP 1Document3 pagesNCP 1kat2111993No ratings yet
- Mycophenolate Mofetil (Cellcept) and Mycophenolate Sodium (Myfortic)Document3 pagesMycophenolate Mofetil (Cellcept) and Mycophenolate Sodium (Myfortic)Riksan RiksanNo ratings yet
- CT ColonDocument2 pagesCT Colonjaijai magbanuaNo ratings yet
- 21 - Thyroid Function TestsDocument2 pages21 - Thyroid Function Testshamadadodo7No ratings yet
- Incident Report Form JrubioDocument2 pagesIncident Report Form Jrubioapi-389592662No ratings yet
- COPARDocument21 pagesCOPAREdra VillanuevaNo ratings yet
- Mindanao Sanitarium and Hospital College: School of NursingDocument2 pagesMindanao Sanitarium and Hospital College: School of NursingTarquin TomadaNo ratings yet
- LosartanDocument2 pagesLosartanAngeliqueNo ratings yet
- NCPDocument4 pagesNCPJoseph Dableo ParreñoNo ratings yet
- Acute Head InjuryDocument5 pagesAcute Head InjuryRitesh KumarNo ratings yet
- DELA PEÑA - Bridge of Spies - Movie Analysis GLOBALIZATIONDocument1 pageDELA PEÑA - Bridge of Spies - Movie Analysis GLOBALIZATIONMark Teofilo Dela PeñaNo ratings yet
- Module 1 - Self AssessmentDocument3 pagesModule 1 - Self AssessmentKathleenNo ratings yet
- Nursing Care PlanDocument7 pagesNursing Care PlantinnnnnnnnnnnnnNo ratings yet
- Importance of Honesty in MedicineDocument3 pagesImportance of Honesty in MedicineSuiweng WongNo ratings yet
- Bea Case StudyDocument19 pagesBea Case StudyBea Flor Rapisura-PegadNo ratings yet
- Health Education ExampleDocument11 pagesHealth Education ExampleSbs Nhanxzkie Jountey MushroomxzNo ratings yet
- Review of Related Literature and Studies: EducationDocument19 pagesReview of Related Literature and Studies: EducationKatherine 'Chingboo' Leonico LaudNo ratings yet
- Case Study ReportDocument23 pagesCase Study Reportapi-290866384No ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Basic Understanding of PBPK: Principles & Connection To The Broader Scope of Systems PharmacologyDocument28 pagesBasic Understanding of PBPK: Principles & Connection To The Broader Scope of Systems PharmacologyBenni IskandarNo ratings yet
- Recommendations For Standards of Monitoring During Anaesthesia and Recovery 2021Document14 pagesRecommendations For Standards of Monitoring During Anaesthesia and Recovery 2021Ahmad Fairuz Abdul ShokriNo ratings yet
- International Public Safety Association InfoBrief TECC V TCCCDocument16 pagesInternational Public Safety Association InfoBrief TECC V TCCCepraetorianNo ratings yet
- BrexitDocument6 pagesBrexitSunit BhalshankarNo ratings yet
- WEEK 2 August 29 - Sep 02Document3 pagesWEEK 2 August 29 - Sep 02Dian LegaspiNo ratings yet
- 5W Vdec Dinkes 01sd10dec2018 10dec2018Document238 pages5W Vdec Dinkes 01sd10dec2018 10dec2018ihwan Ukhrawi AlyNo ratings yet
- Ganser Syndrome: A Case Report From ThailandDocument4 pagesGanser Syndrome: A Case Report From ThailandYuyun Ayu ApriyantiNo ratings yet
- Group 10: 1. Describe The Journey of Shahnaz HussainDocument3 pagesGroup 10: 1. Describe The Journey of Shahnaz HussainShyamsunder SharmaNo ratings yet
- Blood Research and DisordersDocument5 pagesBlood Research and Disordersdr_joe23No ratings yet
- Current Good Manufacturing Practice - Fda CGMPDocument3 pagesCurrent Good Manufacturing Practice - Fda CGMPckbhaiNo ratings yet
- PTSD WorksheetDocument6 pagesPTSD WorksheetJoe JoeNo ratings yet
- Classsification of RPDDocument37 pagesClasssification of RPDdranandmds100% (2)
- 2003 White PaperDocument26 pages2003 White PaperShreeNo ratings yet
- OET Writing Criteria 2019 PDFDocument11 pagesOET Writing Criteria 2019 PDFJohn MontyNo ratings yet
- Reproductive Cycles in MammalsDocument9 pagesReproductive Cycles in MammalsSeemal shahidNo ratings yet
- 16052020DWSGS9ZFEIAEMPDocument390 pages16052020DWSGS9ZFEIAEMPwongjonny1358No ratings yet
- English Assorted Practice TestDocument20 pagesEnglish Assorted Practice TestMinh Hòa83% (6)
- CMS 3000 High Frequency Surgical Unit: FeatureDocument1 pageCMS 3000 High Frequency Surgical Unit: Feature-Nurman Hidayat-No ratings yet
- Total Quality Management (890) : Presented By: Salman Ahmad Khan Roll No: W-588058Document25 pagesTotal Quality Management (890) : Presented By: Salman Ahmad Khan Roll No: W-588058Mustafa Khuzema GangerdiwalaNo ratings yet
- Deliberative Systematic Phase of The Nursing Process That Involves Decision-Making and Problem-SolvingDocument10 pagesDeliberative Systematic Phase of The Nursing Process That Involves Decision-Making and Problem-SolvingLove Jovellanos ÜNo ratings yet
- What Is Interventional RadiologyDocument8 pagesWhat Is Interventional RadiologyNIMKY EMBER B. CLAMOHOYNo ratings yet
- Speaking Sample Test 5 (Dentistry)Document2 pagesSpeaking Sample Test 5 (Dentistry)Jia SunNo ratings yet
- Assessment of Patients in Emergency DepartmentDocument22 pagesAssessment of Patients in Emergency DepartmentClaudine PadillonNo ratings yet
- Filipino Nurses Have Always Been Highly Sought After GloballyDocument3 pagesFilipino Nurses Have Always Been Highly Sought After GloballyElizer ConjeladoNo ratings yet
- The Impact of Artificial Intelligence On HealthcareDocument2 pagesThe Impact of Artificial Intelligence On Healthcaremohammedezrouil100% (1)
- Health Wellbeing Final ReportDocument265 pagesHealth Wellbeing Final ReportPreeti GoelNo ratings yet
- TLFDocument4 pagesTLFPanchdev KumarNo ratings yet
- Last Child in The Woods - Overview - Richard LouvDocument1 pageLast Child in The Woods - Overview - Richard LouvGengjiaqi CHANGNo ratings yet