Download as pdf or txt
You might also like
- Diagnosis of Vaginosis by of Fluid: VaginalDocument8 pagesDiagnosis of Vaginosis by of Fluid: VaginalGunay AliyevaNo ratings yet
- Bvblue Test For Diagnosis of Bacterial Vaginosis: Linda Myziuk, Barbara Romanowski, and Stephen C. JohnsonDocument4 pagesBvblue Test For Diagnosis of Bacterial Vaginosis: Linda Myziuk, Barbara Romanowski, and Stephen C. JohnsonPiEI20tAkUNo ratings yet
- PJM 71 509Document10 pagesPJM 71 509Vivek mandalNo ratings yet
- Articulo de VaginosisDocument5 pagesArticulo de VaginosisLololo LololoNo ratings yet
- BV Blue TestDocument4 pagesBV Blue TestElvan Dwi WidyadiNo ratings yet
- Bacterial Vaginosis PaperDocument4 pagesBacterial Vaginosis Paperobakhit91No ratings yet
- Ijmmtd 24 171-174Document5 pagesIjmmtd 24 171-174prabaNo ratings yet
- Vaginal DischargeDocument7 pagesVaginal DischargeAbid SiddiquiNo ratings yet
- Abbas - 2016 - Bacteriological Study of Puerperal Sepsis in Al-Najaf CityDocument9 pagesAbbas - 2016 - Bacteriological Study of Puerperal Sepsis in Al-Najaf CityAbdu GodanaNo ratings yet
- 2006 C MicrosDocument5 pages2006 C MicrosKhairul WaraNo ratings yet
- Colonization of The Upper Genital Tract by Vaginal Bacterial Species in Nonpregnant WomenDocument9 pagesColonization of The Upper Genital Tract by Vaginal Bacterial Species in Nonpregnant WomenAna AdamNo ratings yet
- Evidencia Metro 2Document11 pagesEvidencia Metro 2diegoxxxaNo ratings yet
- Detection and Genomic Analysis of Genital Group B Streptococcus in Pregnant Korean WomenDocument9 pagesDetection and Genomic Analysis of Genital Group B Streptococcus in Pregnant Korean WomenEka Novita WNo ratings yet
- Vaginal MicrobiomeDocument9 pagesVaginal MicrobiomeRika Yulizah GobelNo ratings yet
- Jaqt 06 I 3 P 203Document2 pagesJaqt 06 I 3 P 203Dewi LarasatiiNo ratings yet
- Archivos de Medicina Veterinaria - Comparación de Tres Métodos de Diagnóstico de Paratuberculosis Bovina en Rebaños Lecheros inDocument8 pagesArchivos de Medicina Veterinaria - Comparación de Tres Métodos de Diagnóstico de Paratuberculosis Bovina en Rebaños Lecheros inguadialvarezNo ratings yet
- Vaginal Microbiota E150-1Document56 pagesVaginal Microbiota E150-1shomowwNo ratings yet
- Manifestasi Klinis 2Document9 pagesManifestasi Klinis 2avely NathessaNo ratings yet
- Bacterial Vaginosis GuidelineDocument3 pagesBacterial Vaginosis Guidelinemikrobiologi rsuaNo ratings yet
- MelitusDocument6 pagesMelituswulan faddhylanNo ratings yet
- Cox 2016Document7 pagesCox 2016Bety MartinescuNo ratings yet
- Educational Commentary - Clue Cell Morphology: Diagnostic ConsiderationsDocument5 pagesEducational Commentary - Clue Cell Morphology: Diagnostic ConsiderationsNia chatarinaNo ratings yet
- Jurnal AborsiDocument6 pagesJurnal Aborsimakiyatul madaniaNo ratings yet
- Natalie Williams-Bouyer, Barbara S. Reisner, Gail L. WoodsDocument4 pagesNatalie Williams-Bouyer, Barbara S. Reisner, Gail L. WoodsBaruna AtmajaNo ratings yet
- Jurnal BVDocument3 pagesJurnal BVEnvhy WinaNo ratings yet
- Practical Guide To Diagnosing and Treating Vaginitis (Medscape)Document16 pagesPractical Guide To Diagnosing and Treating Vaginitis (Medscape)Nur Ilmi SofiahNo ratings yet
- Rea 4Document7 pagesRea 4Sushila ModelNo ratings yet
- Clinical Microscopy V.SDocument6 pagesClinical Microscopy V.SJoey MagnoNo ratings yet
- tmpC1AA TMPDocument3 pagestmpC1AA TMPFrontiersNo ratings yet
- Isolation and Identification of Avibacterium Paragallinarum From Layer Chickens in Gazipur, BangladeshDocument3 pagesIsolation and Identification of Avibacterium Paragallinarum From Layer Chickens in Gazipur, BangladeshMd. Ehsanul Haque100% (1)
- Prevalence of Vaginitis Among Women Attending Antenatal Care Centre of Wudil General Hospital, Kano State NigeriaDocument6 pagesPrevalence of Vaginitis Among Women Attending Antenatal Care Centre of Wudil General Hospital, Kano State NigeriaUMYU Journal of Microbiology Research (UJMR)No ratings yet
- Vaginal SecretionsDocument52 pagesVaginal SecretionsKim BuguinaNo ratings yet
- Jfaa 056Document6 pagesJfaa 056VhaNo ratings yet
- Bartholins Gland AbscessesDocument5 pagesBartholins Gland AbscessesDianaAryantiNo ratings yet
- 6726 18912 1 PB PDFDocument6 pages6726 18912 1 PB PDFFadli ArdiansyahNo ratings yet
- Microbiology and Immunology - 2010 - Iorio - A Combination of Methods To Evaluate Biofilm Production May Help To DetermineDocument6 pagesMicrobiology and Immunology - 2010 - Iorio - A Combination of Methods To Evaluate Biofilm Production May Help To DetermineAriane Barcellos Dos SantosNo ratings yet
- 1 s2.0 S0140673684918166 MainDocument5 pages1 s2.0 S0140673684918166 MainjimbojandersonNo ratings yet
- 1b BV ReviewDocument5 pages1b BV Reviewrisda aulia putriNo ratings yet
- Rea 3Document4 pagesRea 3Sushila ModelNo ratings yet
- Vet Pathol-1990-Barr-354-61Document9 pagesVet Pathol-1990-Barr-354-61Leah DayNo ratings yet
- Artigo de Infusao UterinaDocument15 pagesArtigo de Infusao UterinaRhayane CoelhoNo ratings yet
- Physiology and Molecular BiologyDocument16 pagesPhysiology and Molecular BiologymuthiajayantiNo ratings yet
- Lembar Jawaban SoalDocument5 pagesLembar Jawaban SoalWahyuNo ratings yet
- Peled 2004Document2 pagesPeled 2004drpranaykumar5529No ratings yet
- 4582-Article Text-40623-1-10-20150415Document3 pages4582-Article Text-40623-1-10-20150415Ingrid DuarteNo ratings yet
- ТКМ-12 пац-статья-engl-140124Document14 pagesТКМ-12 пац-статья-engl-140124Sergey SidorenkoNo ratings yet
- Laboratory Diagnosis of Streptococcus PyogenesDocument16 pagesLaboratory Diagnosis of Streptococcus PyogenesRima Carolina Bahsas ZakyNo ratings yet
- Pengaruh Kontrasepsi Hormonal Terhadap Kejadian Bakterial VaginosisDocument7 pagesPengaruh Kontrasepsi Hormonal Terhadap Kejadian Bakterial VaginosisEso SolihinNo ratings yet
- Educational Commentary - Basic Vaginal Wet PrepDocument6 pagesEducational Commentary - Basic Vaginal Wet PrepAhmed MostafaNo ratings yet
- Vaginal SecretionsDocument33 pagesVaginal SecretionsMatthew BaluyotNo ratings yet
- JCM 00044-16Document7 pagesJCM 00044-16Renata PrimasariNo ratings yet
- Artículo Científico de InflamaciónDocument5 pagesArtículo Científico de InflamaciónROLANDO FRANCISCO CACERES CONTRERASNo ratings yet
- CandidaDocument3 pagesCandidaayanNo ratings yet
- Endoscopic Jejunal Biopsy Culture: A Simple and Effective Method To Study Jejunal MicrofloraDocument34 pagesEndoscopic Jejunal Biopsy Culture: A Simple and Effective Method To Study Jejunal MicrofloraAqua Rius JudarNo ratings yet
- Medmicro 43 6 452Document6 pagesMedmicro 43 6 452api-296333585No ratings yet
- Identifying Causes of Vaginal Discharge: The Role of Gynecologic Symptoms and SignsDocument7 pagesIdentifying Causes of Vaginal Discharge: The Role of Gynecologic Symptoms and SignsEviza K. NadyaNo ratings yet
- 34 557 ElhaDocument8 pages34 557 ElhaYosi Dwi Saputro Part IINo ratings yet
- 1 s2.0 S009042951930963X Main PDFDocument8 pages1 s2.0 S009042951930963X Main PDFCris FischerNo ratings yet
- Infectious DiseasesDocument6 pagesInfectious DiseasesyutefupNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Modification and Characterization of PolypropyleneDocument7 pagesModification and Characterization of PolypropyleneSaba MalikNo ratings yet
- SamsungLTE Table - RAN Call Release Causes 1.5Document137 pagesSamsungLTE Table - RAN Call Release Causes 1.5gargee502No ratings yet
- Guide: Daily ReferenceDocument8 pagesGuide: Daily ReferenceGalina TodorovaNo ratings yet
- Ganesh Balasubramanian (Eds.) - Advances in Nanomaterials - Fundamentals, Properties and Applications-Springer International Publishing (2018)Document181 pagesGanesh Balasubramanian (Eds.) - Advances in Nanomaterials - Fundamentals, Properties and Applications-Springer International Publishing (2018)Jesus Moreno Castillo100% (1)
- Effects of Handling On Animals Welfare During TranDocument54 pagesEffects of Handling On Animals Welfare During TranNikhilesh WaniNo ratings yet
- NKK Handbook For ISM AuditsDocument29 pagesNKK Handbook For ISM Auditsbill baileyNo ratings yet
- EN Quick Reference Guide Fabian HFOi-V4.0Document30 pagesEN Quick Reference Guide Fabian HFOi-V4.0Tanzimul IslamNo ratings yet
- AphishmDocument1 pageAphishmAmit RajputNo ratings yet
- Army Aviation Digest - Jan 1982Document52 pagesArmy Aviation Digest - Jan 1982Aviation/Space History LibraryNo ratings yet
- FBS Pre TestDocument4 pagesFBS Pre TestEvelyn Santos100% (1)
- Full Project ReportDocument46 pagesFull Project ReportRakeshNo ratings yet
- Grade 8 Integrated Science Week 2 Lesson 2Document5 pagesGrade 8 Integrated Science Week 2 Lesson 2Balram HaroldNo ratings yet
- Perceptual Stability in Atonal MusicDocument30 pagesPerceptual Stability in Atonal Musicmarcela pavia100% (1)
- MA 231 MATHEMATICS III 2006 Question PaperDocument3 pagesMA 231 MATHEMATICS III 2006 Question Paperyasin muhamedNo ratings yet
- Order 3726049-Vietnam WarDocument6 pagesOrder 3726049-Vietnam WarShaban KimuyuNo ratings yet
- Combiflam Tablets PI - 08072019Document13 pagesCombiflam Tablets PI - 08072019ArunNo ratings yet
- A. RAPID Research Grant: Total Faculty Costs 0Document3 pagesA. RAPID Research Grant: Total Faculty Costs 0Uzma TahirNo ratings yet
- BT08 PDFDocument4 pagesBT08 PDFAfdhalNo ratings yet
- Sobha LTD Q2 FY 2020 21 Investor PresentationDocument47 pagesSobha LTD Q2 FY 2020 21 Investor PresentationAdarsh Reddy GuthaNo ratings yet
- Matrix - An IntroductionDocument10 pagesMatrix - An IntroductionMajid AbNo ratings yet
- BAUR Cable Locator: Data SheetDocument2 pagesBAUR Cable Locator: Data Sheetwinston11No ratings yet
- 11 HUMSS JQR - Family Earthquake PreparednessDocument4 pages11 HUMSS JQR - Family Earthquake PreparednessCLARIZZE JAINE MANALONo ratings yet
- Series HDocument6 pagesSeries HAviation World100% (3)
- Attila Ilhan, Poems Translated Into English, Oct 2007Document20 pagesAttila Ilhan, Poems Translated Into English, Oct 2007Mrs Nilufer Mizanoglu Reddy100% (4)
- Immersion PaperDocument21 pagesImmersion PaperCarl Justin BallertaNo ratings yet
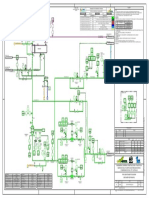
- HE-210 P-2604A-B - DEBUTANIZER FEED PREHEATING - Rev 0CxDocument1 pageHE-210 P-2604A-B - DEBUTANIZER FEED PREHEATING - Rev 0CxMariaNo ratings yet
- Conviction in Cheque Bounce CaseDocument24 pagesConviction in Cheque Bounce CaseArvind PatilNo ratings yet
- BIO Genetics Eukaryote TranscriptionDocument23 pagesBIO Genetics Eukaryote TranscriptionAnonymous SVy8sOsvJDNo ratings yet
- SPWLA Log IntegrationDocument14 pagesSPWLA Log IntegrationpahlawankemalemanNo ratings yet
- Sea Food DishesDocument60 pagesSea Food DishesOliver FabonNo ratings yet