
Professional Documents
Culture Documents
Module II: Care of At-Risk / High Risk and Sick Mother (Part I)
Module II: Care of At-Risk / High Risk and Sick Mother (Part I)
Uploaded by
Hakdog ShermolangCopyright:
Available Formats
You might also like
- Costa Leona Series 1 Scorching LoveDocument27 pagesCosta Leona Series 1 Scorching LoveHakdog Shermolang67% (3)
- A Community Diagnosis in Level III Group 2Document89 pagesA Community Diagnosis in Level III Group 2Jenny Agustin FabrosNo ratings yet
- Science Grade 3 Activity SheetDocument9 pagesScience Grade 3 Activity SheetEllanie Pujalte MontebonNo ratings yet
- Selenereese - RUTHLESS MEN SERIES 1 Hellions Possession 1Document198 pagesSelenereese - RUTHLESS MEN SERIES 1 Hellions Possession 1Hakdog Shermolang100% (2)
- Topic 2 ExercisesDocument6 pagesTopic 2 ExercisesRaniel Pamatmat0% (1)
- Prelim Reviewer 2023Document83 pagesPrelim Reviewer 2023jakexsanchez1515No ratings yet
- Finals Exam Ncm209Document91 pagesFinals Exam Ncm209Shang MarianoNo ratings yet
- Prelim Outline - Bioethics BSNDocument11 pagesPrelim Outline - Bioethics BSNSheenaNo ratings yet
- Ncma219 Lec MidtermDocument51 pagesNcma219 Lec MidtermMacababbad Joshua MiguelNo ratings yet
- BIOETHICS ABCDE Compilation WK 2 6Document268 pagesBIOETHICS ABCDE Compilation WK 2 6Sexbomb Adela KirstenNo ratings yet
- Group 2 - Technology As A Way of RevealingDocument50 pagesGroup 2 - Technology As A Way of Revealinggenar greg tubogNo ratings yet
- NCM 108 Bioethics Finals 1Document10 pagesNCM 108 Bioethics Finals 1Martina MedranoNo ratings yet
- Minutes) Everybody WritesDocument15 pagesMinutes) Everybody WritesRanes AndyNo ratings yet
- Quality of Prenatal Care Questionnaire: Instrument Development and TestingDocument17 pagesQuality of Prenatal Care Questionnaire: Instrument Development and TestingGreat CoassNo ratings yet
- Ra 7600Document5 pagesRa 7600WeGovern InstituteNo ratings yet
- Psych-Midterm ReviewerDocument12 pagesPsych-Midterm ReviewerPia Rose RoqueNo ratings yet
- Ethics ConsequentialismDocument19 pagesEthics ConsequentialismJibfrho SagarioNo ratings yet
- NCM209Document94 pagesNCM209Gummy BearsNo ratings yet
- Ncam219 Lec PDFDocument102 pagesNcam219 Lec PDFDAVE BARIBENo ratings yet
- Older AdultsDocument10 pagesOlder AdultsMia Grace GarciaNo ratings yet
- Module 11, Chapter 27:: University of Cebu-BaniladDocument10 pagesModule 11, Chapter 27:: University of Cebu-BaniladSuzanne Kyla CabuenasNo ratings yet
- CHN Reviewer IDocument21 pagesCHN Reviewer IApple Mae AuxteroNo ratings yet
- NCM 112 Prefinal LectureDocument10 pagesNCM 112 Prefinal LectureFatima-Ridziana AbdurahmanNo ratings yet
- MCN Lec MidtermDocument29 pagesMCN Lec Midtermnaomie manaliliNo ratings yet
- Marquez - Case Study 114Document6 pagesMarquez - Case Study 114Caren MarquezNo ratings yet
- The Voluntary and Nonvoluntary Acts of ManDocument2 pagesThe Voluntary and Nonvoluntary Acts of ManJohn Michael SorianoNo ratings yet
- NCM 207 Lecture 1 PDFDocument127 pagesNCM 207 Lecture 1 PDFkrizza abellanosaNo ratings yet
- CONSEQUENTIALISMDocument26 pagesCONSEQUENTIALISMAngelica TañedoNo ratings yet
- Rle Module Rle Unit Week: Bachelor of Science in Nursing: Rle NCM 105 - Psychiatric NursingDocument4 pagesRle Module Rle Unit Week: Bachelor of Science in Nursing: Rle NCM 105 - Psychiatric NursingGabriel VillegasNo ratings yet
- OB GYN CasePre FinalDocument82 pagesOB GYN CasePre FinalMarjorie Lahaylahay AlabataNo ratings yet
- NCM 112 Lec NotesDocument10 pagesNCM 112 Lec NotesCamille GuintoNo ratings yet
- Hes 005 Session 16 SasDocument7 pagesHes 005 Session 16 SasJose Melmar Autida AutenticoNo ratings yet
- Kidney Disease and PregnancyDocument11 pagesKidney Disease and PregnancyAndreaNo ratings yet
- Pharma Notes MidsDocument17 pagesPharma Notes MidsMa. Rita Concepcion TungulNo ratings yet
- Congenital Hydrocephalus: Case PresentationDocument35 pagesCongenital Hydrocephalus: Case PresentationIan Mizzel A. DulfinaNo ratings yet
- DS (Ibuprofen)Document6 pagesDS (Ibuprofen)Mary April MendezNo ratings yet
- Chapter 12: Nursing Care To Promote Fetal and Maternal HealthDocument9 pagesChapter 12: Nursing Care To Promote Fetal and Maternal HealthAlyssaGrandeMontimorNo ratings yet
- Week 1 RUBRICS Wound Care and DressingDocument2 pagesWeek 1 RUBRICS Wound Care and DressingPaola CruzNo ratings yet
- NCM 109 FinalsDocument68 pagesNCM 109 FinalsJHOANA MARIE LOONo ratings yet
- Module 7 Student Activity SheetDocument7 pagesModule 7 Student Activity SheetJenny Agustin FabrosNo ratings yet
- Ncm105 Nutrition ReviewerDocument24 pagesNcm105 Nutrition ReviewerJeon CookyNo ratings yet
- OB - Postterm PregnancyDocument6 pagesOB - Postterm PregnancyDarren Mae MosadaNo ratings yet
- CHN ReviewerDocument8 pagesCHN Revieweralyssaaaaa1234885No ratings yet
- Aparicio Ryan Shane Y. Toddler AssessmentDocument24 pagesAparicio Ryan Shane Y. Toddler AssessmentThea DuoNo ratings yet
- Rle Activity 107 MMDSTDocument12 pagesRle Activity 107 MMDSTMaxene Reyes ValdezNo ratings yet
- Funda RLEDocument29 pagesFunda RLECharisse CaydanNo ratings yet
- Appearance of A NewbornDocument33 pagesAppearance of A NewbornGeguirra, Michiko SarahNo ratings yet
- Case Study NCM 109 ApacibleDocument9 pagesCase Study NCM 109 ApacibleJade CentinoNo ratings yet
- Ncma217 Lec MidtermDocument21 pagesNcma217 Lec Midtermcaitie miracleNo ratings yet
- Neutralizes The Acidity of The UrethraDocument12 pagesNeutralizes The Acidity of The Urethracresia hidalgoNo ratings yet
- UntitledDocument6 pagesUntitledDada Tin GoTanNo ratings yet
- Rle FinalsDocument9 pagesRle FinalsMary Florence VelardeNo ratings yet
- Nursing Care of The Developing FetusDocument52 pagesNursing Care of The Developing FetusKyrriel CNo ratings yet
- CHN211 Week 8 WORD - Integrated Management of Childhood IllnessDocument28 pagesCHN211 Week 8 WORD - Integrated Management of Childhood IllnessYrah Elaine SanchezNo ratings yet
- ImmunizationDocument4 pagesImmunizationAshley ValdezNo ratings yet
- Book Onco ConceptDocument42 pagesBook Onco ConceptJulia Rae Delos SantosNo ratings yet
- Rhu d1 Compiled December LatestDocument169 pagesRhu d1 Compiled December LatestDilausan B MolukNo ratings yet
- Martha Rogers, Dorothea Orem, Imogene KingDocument9 pagesMartha Rogers, Dorothea Orem, Imogene KingCASTRO, ANDREI KARL Z.No ratings yet
- NCM 107 RLE 1F - Labor and DeliveryDocument68 pagesNCM 107 RLE 1F - Labor and DeliveryNotur BarbielatNo ratings yet
- Case PresDocument100 pagesCase PresJoj BagnateNo ratings yet
- RABE 1 CHN 2semDocument6 pagesRABE 1 CHN 2semBasa, Rica Mae P.No ratings yet
- Transes MCN Laboratory Week 1Document17 pagesTranses MCN Laboratory Week 1Akira Pineda100% (1)
- Sas 11 LectureDocument3 pagesSas 11 LectureFretchel Grace Silverado MesaNo ratings yet
- Muscle LabDocument7 pagesMuscle LabHakdog ShermolangNo ratings yet
- Bed Making: Occupied Bed Unoccupied BedDocument16 pagesBed Making: Occupied Bed Unoccupied BedHakdog ShermolangNo ratings yet
- C C C V C C C V C C C V C C C C C V C C C V C C C V C C C V C C C V C C C VDocument1 pageC C C V C C C V C C C V C C C C C V C C C V C C C V C C C V C C C V C C C VHakdog ShermolangNo ratings yet
- Biofuel Ft. KantutayDocument21 pagesBiofuel Ft. KantutayHakdog Shermolang100% (1)
- Heat Transfer Class Project: Powerpoint Presentation File Name It: Project2014-# in Class Roll-#In Class RollDocument3 pagesHeat Transfer Class Project: Powerpoint Presentation File Name It: Project2014-# in Class Roll-#In Class RollSwapnil BhattacharyaNo ratings yet
- SULIT 4551/3 Biologi Kertas 3 Sept 2007 SeptemberDocument13 pagesSULIT 4551/3 Biologi Kertas 3 Sept 2007 SeptemberhasimahazitNo ratings yet
- A Hybrid Cutting Force Model For High-Speed Milling of Titanium AlloysDocument4 pagesA Hybrid Cutting Force Model For High-Speed Milling of Titanium Alloysabdsu75No ratings yet
- 1Document10 pages1Shashank PathakNo ratings yet
- Transient Results and Response Spectra: Sofistik 2020Document25 pagesTransient Results and Response Spectra: Sofistik 2020Chris LumyNo ratings yet
- Rooms DivisionDocument19 pagesRooms Divisionনিয়াজ মাহমুদNo ratings yet
- Hawthorne ExperimentsDocument7 pagesHawthorne ExperimentsAbhishek MishraNo ratings yet
- KERENDIA Doctor Discussion Guide - FINALDocument2 pagesKERENDIA Doctor Discussion Guide - FINALajaygajaNo ratings yet
- Performance Assesment-A Shift From Intangibles To TangiblesDocument25 pagesPerformance Assesment-A Shift From Intangibles To Tangibles2005ravi100% (1)
- Describe The Appearance and Uses Uniform and Non-Uniform Mixtures (S6MT-Ia-c-1)Document4 pagesDescribe The Appearance and Uses Uniform and Non-Uniform Mixtures (S6MT-Ia-c-1)Nerissa de LeonNo ratings yet
- Discourse Analysis of Lilith PDFDocument30 pagesDiscourse Analysis of Lilith PDFJorge BelinskyNo ratings yet
- Women EntrepreneursDocument19 pagesWomen Entrepreneursmohit_roy_8No ratings yet
- A Guide To Transformer Maintenance by S D Myers J J Kelly R H Parrish 0939320002Document5 pagesA Guide To Transformer Maintenance by S D Myers J J Kelly R H Parrish 0939320002N4Y CHANNELNo ratings yet
- Callista Roy The Adaptation Model of NursingDocument8 pagesCallista Roy The Adaptation Model of Nursingapi-640980201No ratings yet
- AWNMag6 02Document57 pagesAWNMag6 02Michał MrózNo ratings yet
- English Answer Sheet First Quarter Module 2Document6 pagesEnglish Answer Sheet First Quarter Module 2Jakecob Mejillano JacobNo ratings yet
- 이휘소 논문 PDFDocument4 pages이휘소 논문 PDFjemin12798No ratings yet
- Trigonometry Exam QuestionsDocument9 pagesTrigonometry Exam Questionsnsprior1659No ratings yet
- Dada Vaswani SpeechDocument15 pagesDada Vaswani SpeechTheresa WestNo ratings yet
- A Comparative Study On Fundamental and Technical AnalysisDocument34 pagesA Comparative Study On Fundamental and Technical AnalysisTarun Chawla0% (1)
- York County Court Schedule For May 4, 2015Document10 pagesYork County Court Schedule For May 4, 2015York Daily Record/Sunday NewsNo ratings yet
- 01 Reading PTEDocument5 pages01 Reading PTEUsha ShresthaNo ratings yet
- Romeo and Juliet 2023 WorkbookDocument62 pagesRomeo and Juliet 2023 WorkbooklstewardNo ratings yet
- P12y en T C74Document572 pagesP12y en T C74spakumaranNo ratings yet
- FRC Essays - Comply or ExplainDocument64 pagesFRC Essays - Comply or ExplainRahat TabassumNo ratings yet
- Manual For Audi A3Document2 pagesManual For Audi A3Anonymous mXONwr1c4No ratings yet
- Stresses in Soil 161208Document67 pagesStresses in Soil 161208Tuan Jalai100% (1)
- Aging Management Program Effectiveness: NEI 14-12 (Revision 0)Document16 pagesAging Management Program Effectiveness: NEI 14-12 (Revision 0)naveedNo ratings yet































































































Module II: Care of At-Risk / High Risk and Sick Mother (Part I)
Module II: Care of At-Risk / High Risk and Sick Mother (Part I)
Uploaded by
Hakdog ShermolangOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Module II: Care of At-Risk / High Risk and Sick Mother (Part I)
Module II: Care of At-Risk / High Risk and Sick Mother (Part I)
Uploaded by
Hakdog ShermolangCopyright:
Available Formats
Module II: Care of At-Risk / High Risk
and Sick Mother (Part I)
Lesson 1: Nursing Care of the Pregnant Client
Lesson 2: Nursing Care of Clients with Sudden
Pregnancy Complication
Lesson 3: Nursing Care of Client with Special
Needs
Module II: Care of At-Risk / High Risk and Sick Mother
(Part I)
INTRODUCTION
This module presents nursing care of high risk mothers. Identifying high risk clients through
screening and assessment will be discussed along with the conditions that may affect pregnancy.
LEARNING OBJECTIVES
1. Define high-risk pregnancy, including preexisting factors that contribute to its development
such as diabetes mellitus or cardiovascular disease.
2. Describe sudden complications of pregnancy that place a pregnant woman and her fetus at
high risk.
3. Implement nursing care specific to a woman who has developed a sudden complication of
pregnancy, such as teaching her how to recognize the symptoms of preterm labor.
4. Identify the characteristics and the risks of pregnancy for a pregnant woman who has
special needs, such as one who has been injured, an adolescent, a woman over age 40
years, one who is physically or cognitively challenged, or a woman who is substance
dependent.
5. Implement nursing care for a woman with special needs, such as encouraging her to remain
ambulatory during pregnancy.
DIRECTION/MODULE ORGANIZER
There are three lessons in the module. Read each lesson carefully then answer the summative test
to find out how much you have benefited from it. Submit your output to your instructor or to the
CCHAMS Office.
In case you encounter difficulty, discuss this with your instructor during the face-to-face
meeting. If not contact your instructor at the CCHAMS office.
Good luck and happy reading!!!
NUPC 110 Module II Page 2
LESSON 1: Nursing Care of the Pregnant Client
I. HIGH RISK PREGNANCY
one in which a concurrent disorder, pregnancy-related complication, or external factor
jeopardizes the health of the woman, the fetus, or both
Three major causes of maternal death:
o Hypertensive Disorders
o Infection
o Hemorrhage
Factors related to maternal death
o Age (Younger than 20 years and 35 years older)
o Lack of prenatal care.
o Low educational attainment
o Unmarried Status
Leading cause of death in the neonatal period is congenital anomalies
o Other causes:
Disorders related to short gestation and low birth weight
Sudden Infant Death
Respiratory Distress Syndrome
Effects of Maternal Complications
Factors that place a pregnancy at risk can be divided into four categories:
1. Existing Health Conditions
2. Age
3. Lifestyle Factors
4. Conditions of Pregnancy
II. ASSESSMENT OF HIGH-RISK FACTORS
1. History and Physical Examination
a. Biophysical Factors
Genetic considerations
o Genetic factors may interfere with normal fetal or neonatal
development, result in congenital anomalies, or create difficulties
for the mother.
o These factors include defective genes, transmissible inherited
disorders and chromosomal anomalies, multiple pregnancy, large
fetal size, and ABO incompatibility.
Nutritional Status
o Adequate nutrition, without which fetal growth and development
cannot proceed normally, is one of the most important determinants
of pregnancy outcome.
Medical and Obstetric Disorders:
o Complications of current and past pregnancies, obstetric-related
illnesses, and pregnancy losses put the patient at risk.
b. Psychosocial Factor
Smoking:
o A strong, consistent, causal relation has been established between
maternal smoking and reduced birth weight. Risks include low-birth-
weight infants, higher neonatal mortality rates, increased
miscarriages, and in- creased incidence of premature rupture of
membranes.
Caffeine:
NUPC 110 Module II Page 3
oBirth defects in humans have not been related to caffeine
consumption. High intake (three or more cups of coffee per day) has
been related to a slight decrease in birth weight.
Alcohol:
o Although its exact effects in pregnancy have not been quantified and
its mode of action is largely unexplained, alcohol exerts adverse
effects on the fetus, resulting in fetal alcohol syndrome, fetal alcohol
effects, learning disabilities, and hyperactivity.
Drugs:
o Drugs may adversely affect the developing fetus through several
mechanisms. They can be teratogenic, cause metabolic disturbances,
and produce chemical effects, or cause depression or alteration of
central nervous system function.
Psychological Status:
o Childbearing triggers profound and complex physiologic,
psychological, and social changes, with evidence to suggest a relation
between emotional distress and birth complications.
c. Socio-Demographic Factor
Low Income
o Poverty underlies many other risk factors and leads to inadequate
financial resources for food and prenatal care, poor general health,
increased risk of medical complications of pregnancy, and greater
prevalence of adverse environmental influences.
Age
o Women at both ends of the childbearing age spectrum have a higher
incidence of poor outcomes; however, age may not be a risk factor in
all cases. Both physiologic and psychological risks should be
evaluated.
o Adolescents: More complications are seen in young mothers (younger
than 15 years), who have a 60% higher mortality rate than those older
than 20 years, and in pregnancies occurring less than 6 years after
menarche. Complications include anemia, preeclampsia, prolonged
labor, and contracted pelvis and cephalo-pelvic disproportion. Long-
term social implications of early motherhood are lower educational
status, lower income, and increased dependence on government
support programs, higher divorce rates, and higher parity.
o Mature Mothers. The risks to older mothers are not from age alone
but from other considerations such as number and spacing of previous
pregnancies; genetic disposition of the parents; and medical history,
lifestyle, nutrition, and prenatal care. Medical conditions more likely
to be experienced by mature women include hypertension and
preeclampsia, diabetes, extended labor, cesarean birth, placenta
previa, abruptio placentae, and mortality. Her fetus is at greater risk
for low birth weight and macrosomia, chromosomal abnormalities,
congenital malformations, and neonatal mortality.
o Parity. The number of previous pregnancies is a risk factor associated
with age and includes all first pregnancies, especially a first
pregnancy at either end of the child- bearing age continuum. The
incidence of preeclampsia and dystocia is higher with a first birth.
o Marital Status. The increased mortality and morbidity rates for
unmarried women, including a greater risk for preeclampsia, are
often related to inadequate prenatal care and a younger childbearing
age.
NUPC 110 Module II Page 4
o Residence. The availability and quality of prenatal care varies widely
with geographic residence. Women in metropolitan areas have more
prenatal visits than do those in rural areas, who have fewer
opportunities for specialized care and consequently a higher
incidence of maternal mortality. Health care in the inner city, where
residents are usually poorer and begin childbearing earlier and
continue for longer, may be of lower quality than in a more affluent
neighborhood.
o Ethnicity. Although ethnicity by itself is not a major risk, race is an
indicator of other socio-demographic risk factors. Nonwhite women
are more than 3 times as likely as Caucasian women to die of
pregnancy-related causes. African-American babies have the highest
rates of pre- maturity and low birth weight, with the infant mortality
rate among African-Americans being more than double that among
Caucasians.
d. Environmental Factor
Various environmental substances can affect fertility and fetal development,
the chance of a live birth, and the child’s subsequent mental and physical
development.
Environmental influences include infections, radiation, and chemicals such
as pesticides, therapeutic drugs, illicit drugs, industrial pollutants, cigarette
smoke, stress, and diet.
Paternal exposure to mutagenic agents in the work- place has been
associated with an increased risk of miscarriage
2. Biophysical Monitoring
a. Daily Fetal Movement Count/ “kick counts”
It can be done at home, A non-invasive, a simple to understand, and usually
does not interfere with a daily routine
frequently used to monitor the fetus in pregnancies complicated by
conditions that may affect fetal oxygenation like gestational hypertension or
chronic hypertension and diabetes
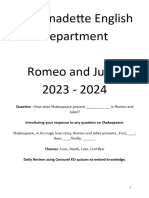
b. Ultrasonography
an important, safe Figure 1.
technique in antepartum Ultrasound
fetal surveillance, which
provides critical in-
formation to health care
providers regarding fetal
activity and gestational age,
normal versus abnormal
fetal growth curves, visual
assistance with which
invasive tests may be performed more safely, fetal and placental anatomy,
and fetal well- being and can be done abdominally or transvaginally
Can be demonstrated as early as 6 – 7
weeks by real-time echo scanners and at 10
Figure
– 12 weeks by Doppler mode 2.MRI
c. Magnetic Resonance Imaging (MRI)
A noninvasive radiologic technique for
obstetric and gynecologic diagnosis that
provides excellent pictures of soft tissue
Evaluates the following:
o Fetal structure, CNS, thorax,
abdomen, GUT, musculoskeletal
system, overall growth
NUPC 110 Module II Page 5
o Placenta: position, density, presence of gestational trophoblastic dse
o Quantity of amniotic fluid
o Maternal structures: uterus, cervix, adnexa, pelvis
o Biochemical status: ph, adenosine triphosphate content of tissues
and organs
o Soft tissue, metabolic or functional anomalies
3. Biochemical Assessment
are invasive and carry risks to the mother and fetus
a. Amniocentesis
Done after 14th week of pregnancy
Indications: diagnosis of genetic or
congenital anomalies and hemolytic
disease of the fetus and newborn
(HDFN), assessment of pulmonary
maturity, and presence of meconium
Because of the possibility of feto-
maternal hemorrhage, it is standard
practice after an amniocentesis to
administer RhoD immune globulin to
the woman who is Rh negative
Figure 3. Amniocentesis
b. Chorionic Villi Sampling (CVS)
procedure is performed between 10
and 12 weeks of gestation and
involves the removal of a small
tissue specimen from the fetal
portion of the placen ta because
chorionic villi originate in the
zygote, this tissue reflects the
genetic makeup of the fetus
An indication for CVS are similar to
those for amniocentesis but on
second-trimester amniocentesis
appears to be safer than CVS Figure 4. CVS
Types:
o Transcervically Sampling
A sterile catheter is introduced into the cervix under
continuous ultrasonographic guidance, and a small portion of
the chorionic villi is aspirated with a syringe
o Transabdominally Sampling
An 18-gauge spinal needle with stylet is inserted under sterile
conditions through the abdominal wall into the chorion
frondosum under ultrasound guidance
Figure 5.CVS and
amniocentesis
NUPC 110 Module II Page 6
c. Percutaneous Umbilical Blood Sampling (PUBS)/Cordocentesis
Direct access to fetal circulation
during the 2nd and third
trimester, widely used method
for fetal blood sampling and
transfusion
1-4 ml of blood is extracted and
tested through the Kleihauer-
Betke procedure to ensure that
is fetal in origin
Kleihauer-Betke is a blood test used to measure
Figure the amount of fetal hgb
6. PUBS
transferred from fetus to a
mother’s bloodstream
d. Maternal Assay
Figure 7. Intrauterine Transfusion
Alpha-fetoprotein
- Maternal Serum AFP levels
have been used as a
screening tool for neural
tube defects
- 80% to 85 % of NTDs and
abdominal wall defects can
be detected
- increasing levels are
detectable in pregnant
women from 14 to 34 weeks
Coomb’s Test
- indirect coomb’s test is a
screening for Rh incompatibility. If the maternal titer for Rh antibodies is
greater than 1:8, amniocentesis for determination of bilirubin in amniotic
fluid is indicated to establish the severity of fetal hemolytic anemia.
- this test also detects other antibodies that may place the fetus at risk for
incompatibility with maternal antigens
III. HIGH RISK PREGNANCY FACTORS
1. Existing Health Conditions
a. Cardiovascular Disorder and Pregnancy
complicates only approximately 1% of all pregnancies
responsible for 5% of maternal deaths during pregnancy
Blood volume and Cardiac output increase 30% to 50% during pregnancy
Functional (innocent) murmurs are present because of the increase in blood vol.
and cardiac output
Most common disorders: valve damage caused by rheumatic fever or Kawasaki
disease and congenital anomalies such as atrial septal defect or uncorrected
coarctation of the aorta.
Increasing age of pregnancy increases the incidence of coronary artery disease
and varicosities during pregnancy
Peripartum heart disease rarely occurs
NUPC 110 Module II Page 7
CLASSIFICATION OF HEART DISEASE
a.1. Left-sided Heart Failure
left ventricle cannot move the volume of blood forward that it has received by
the left atrium from the pulmonary circulation.
heart becomes so overwhelmed it fails to function
Because of the limited oxygen exchange, women with pulmonary hypertension
are at extremely high risk for spontaneous miscarriage, preterm labor, or
maternal death
A woman experiences increased fatigue, weakness, and dizziness (specifically
from lack of oxygen in brain cells)
pulmonary edema becomes severe, a woman cannot sleep in any position except
with her chest and head elevated (orthopnea)
paroxysmal nocturnal dyspnea—suddenly waking at night short of breath
With the more effective heart action, interstitial fluid returns to the circulation
and overburdens the circulation, causing increased left-side failure and
increased pulmonary edema
a.2. Right-Sided Heart Failure
occurs when the output of the right ventricle is less than the blood volume
received by the right atrium from the vena cava
Back-pressure from this results in congestion of the systemic venous circulation
and decreased cardiac output to the lungs.
Blood pressure decreases in the aorta because less blood is reaching it; pressure
is high in the vena cava from back-pressure of blood;
Both jugular venous distention and increased portal circulation occur
The liver and spleen become distended
Liver enlargement can cause extreme dyspnea and pain in a pregnant woman
because the enlarged liver, as it is pressed upward by the enlarged uterus, puts
extreme pressure on the diaphragm.
Distention of abdominal vessels can lead to exudate of fluid from the vessels
into the peritoneal cavity (ascites)
Fluid also moves from the systemic circulation into lower extremity interstitial
spaces (peripheral edema).
Eisenmenger Syndrome – congenital anomaly most apt to cause right-sided
heart failure in women
of reproductive age
a.3. Peripartum Heart Disease
An extremely rare
condition, peripartal
NUPC 110 Module II Page 8
cardiomyopathy can originate in pregnancy in women with no previous history
of heart disease
Mortality rate as high as 50%
occurs most often in African American multiparas in conjunction with
hypertension of pregnancy
signs of myocardial failure such as shortness of breath, chest pain, and edema
a.4. Assessment of Woman with Cardiac Disease
Check for signs of poor circulation
Assess edema
Right-sided heart failure – assess for liver enlargment
Left-sided heart failure – assess foo pulmonary symptoms like cough
ECG, chest radiography, echocardiography
Fetal Assessment
o poor perfusion level may also lead to an acidotic fetal environment if the
blood flow becomes inadequate for carbon dioxide exchange
o Preterm labor; prematurity
o Late deceleration patterns
a.5. Implementation
Promote rest
Promote healthy nutrition
Educate regarding medication
Close to the anticipated day of birth, some physicians begin a course of
an antibiotic for women with heart disease such as penicillin because the
postpartum period always involves some mild invasion of bacteria from
the denuded placental site on the uterus into the blood-stream.
Educate Regarding Avoidance of Infection
Be Prepared for Emergency Actions
b. Hematologic Disorders and Pregnancy
1. Anemia
Pseudo-anemia of early pregnancy – blood volume expands during pregnancy
slightly ahead of the red cell count
True anemia – when a woman’s hemoglobin concentration is less than 11 g/dL
(hematocrit 33%) in the first or third trimester of pregnancy or hemoglobin
concentration is less than 10.5 g/dL (hematocrit 32%)in the second trimester
2. Iron-Deficiency Anemia
Most common anemia of pregnancy, complicating as many as 15% to 25% of all
pregnancies
Ineffective oxygen transport – fatigue and poor exercise tolerance
Associated with LBW and preterm birth
Some women develop pica (ice chips/starch)
iron supplement of 60 mg elemental iron as prophylactic therapy during
pregnancy/ therapeutic– 120 to 200 mg elemental iron/day)
Intake of iron-rich foods
Severe IDA – iron injections
Side effect (iron supp) – constipation and gastric irritation/ black stools
o Increase roughage/ take pills with food
3. Folic Acid-Deficiency Anemia
Folic acid – normal RBC formation in mothers and prevents NTDs in fetus
o occurs most often in multiple pregnancies because of the increased fetal
demand
o in women with a secondary hemolytic illness in which there is rapid
destruction and production of new red blood cells
o in women who are taking hydantoin, an anticonvulsant agent that interferes
with folate absorption
o in women who have been taking oral contraceptives; and in women who
have had a gastric bypass for morbid obesity
Megaloblastic Anemia
NUPC 110 Module II Page 9
may be a contributory factor in early miscarriage or premature separation of the
placenta.
Tx – folic Acid supplement of 400 microgram (TTC) daily to 600 microgram
(pregnancy)
4 Sickle Cell Anemia
a recessively inherited hemolytic anemia caused by an abnormal amino acid in
the beta chain of hemoglobin [sickle hemoglobin (HbS) if valine is replaced and
nonsickling hemoglobin (HbC) if lysine is replaced]
majority of red blood cells are irregular or sickle shaped so they cannot carry as
much hemoglobin as can normally shaped red blood cells
Approximately 1 in every 10 African Americans has the sickle cell trait (i.e.,
carries a recessive gene for S hemoglobin but is asymptomatic)
Women with the homozygous disease is at risk for miscarriage, prematurity or
perinatal mortality rates
Women with SCA are more prone to bacteriuria – periodic U/A
May cause low birth weight and possibly fetal death
Treatment: Exchange transfusion, Folic Acid, adequate hydration
• Avoid standing for long periods
Elevate legs to facilitate venous return
5.Thalassemia
a group of autosomal recessively inherited blood disorders that lead to poor
hemoglobin formation and severe anemia
Treatment: folic acid supplementation and blood transfusion to infuse
hemoglobin rich red blood cells
6. Malaria
a protozoan infection that is transmitted to people by Anopheles mosquitoes
infection causes red blood cells to stick to the surface of capillaries causing
obstruction of these vessels
This can result in end organ anoxia when blood cannot reach organs effectively
Treatment: Chloroquine
7. Coagulation Disorders
Most coagulation disorders are sex linked or occur only in males and so have
little effect on pregnancies.
Von Willebrand disease – autosomal dominant d/o which also occurs in females
(factor VIII deficiency)
May cause spontaneous miscarriage or postpartum hemorrhage
Prolonged bleeding time
Cryoprecipitate or fresh-frozen plasma before labor to prevent excessive
bleeding
8. Hemophilia B (Christmas Disease)
Sex-linked disorder and occurs only in males
Factor IX deficiency
Carrier women may have reduced factor IX level making them prone to bleeding
May cause spontaneous miscarriage or hemorrhage during labor
Tx – infusion of factor IX concentrate or fresh-frozen plasma
PUBS can be done to detect hemophilia in male fetus
o Check for the presence of coagulation disorder in fetus and if present, this
procedure will be contraindicated as it may result in extensive fetal blood
loss
9. Idiopathic Thrombocytopenic Purpura (ITP)
assumed to be an autoimmune disease where the body releases antibodies to
platelets causing decreased platelet count
minute petechiae or large ecchymoses appear on a woman’s body
Frequent nosebleeds may occur
Laboratory studies reveal a marked
thrombocytopenia (platelet count may be as low as 20,000/mm3 from a usual
count of 150,000 mm3)
Treatment: Platelet transfusion or plasmapheresis to increase platelet count;
oral prednisone
May cause bleeding at birth
Antiplatelet may cross placenta
NUPC 110 Module II Page 10
c. Renal And Urinary Disorders And Pregnancy
1. Urinary Tract Infection
As many as 4% to 10% of non pregnant women have asymptomatic bacteriuria
In a pregnant woman, because the ureters dilate from the effect of
progesterone, stasis of urine occurs
minimal glucosuria that occurs with pregnancy allows more than the usual
number of organisms to grow
Asymptomatic infection may progress to pyelonephritis and is associated with
preterm labor and premature rupture of membranes
Women with vesicouereteral reflux tend to develop UTI or pyelonephritis more
often
E. coli – most common cause of ascending infections
Strep B – may cause descending infection and is associated with pneumonia in
NB.
Assessment
o Pain on urination
o Pain on lumbar region (right)
o nausea and vomiting, malaise, pain, and frequency of urination
o Fever
o Treatment: antibitiotics such
as amoxicillin, ampicillin and
caphalosphorins are safe
during pregnancy
2. Chronic Renal Disease
Women with chronic renal disease
may develop severe anemia
during pregnancy because their
diseased kidneys do not produce
erythropoietin, which is
necessary for red cell formation
Treatment: synthetic
erythropoeitin
o Dialysis may cause preterm
labor
o For women with kidney
transplant, criteria to be
evaluated include:
– A woman’s general health
and the time since the
trans-plant (preferably +2
years)
– Serum creatinine level
– The presence of
proteinuria or
hypertension or signs of
graft rejection
– Medications taken to
reduce graft rejection
d. Respiratory Disorders And Pregnancy
Any respiratory condition can worsen in pregnancy because the rising uterus
compresses the diaphragm, reducing the size of the thoracic cavity and available
lung space.
o Common cold
o Severe pneumonia
o TB
o COPD
1. Acute Nasopharyngitis
Common cold
estrogen stimulation normally causes some degree of nasal congestion
2. Influenza
Caused by virus (A, B, C)
NUPC 110 Module II Page 11
S/S: high fever, extreme prostration, aching pains in the back and extremities, and
generally a sore, raw throat
Associated with preterm labor
not been clearly correlated with congenital anomalies in children
Treatment: antibiotics, antipyretics, influenza vaccine
3. Pneumonia
bacterial or viral invasion of lung tissue by pathogens such as S. pneumoniae,
Haemophilus influenzae, and Mycoplasma pneumoniae
Inflammatory response confines the bacteria or virus within segments of the lobes
of the lungs but also fills alveoli with fluid, blocking off breathing space
Treatment: antibiotic and oxygen therapy
May cause preterm labor in late pregnancy due to decreased oxygen supply
4. Severe Acute Respiratory Syndrome
a newly emerged infectious disease with the clinical symptoms of persistent fever,
chills, muscle aches, malaise, dry cough, headache, and dyspnea; decreased
lymphocyte and platelet counts.
Caused by corona virus which originated from China
associated with high incidences of spontaneous miscarriage, preterm birth, and
intrauterine growth restriction.
no evidence of perinatal SARS infection among infants born to these mothers.
5. Asthma
reversible airflow obstruction, airway hyperreactivity, and airway inflammation
complicates about 5% to 9% of pregnancies and is potentially associated with an
increased risk of perinatal complications
reduced oxygen supply to a fetus leads to preterm birth or fetal growth restriction
if a major attack should occur during pregnancy
6. Tuberculosis
caused by Mycobacterium tuberculosis,an acid-fast bacillus
Symptoms of tuberculosis include:
o Chronic cough
o Weight loss
o Hemoptysis (coughing blood)
o Night sweats
o Low-grade fever
o Chronic fatigue
PPD to be done in high risk areas
Treatment: Isoniazid (INH) and ethambutol hy-drochloride (Myambutol)
7. Chronic Obstructive Pulmonary Disease
– constriction of the airway associated most often with long-term cigarette smoking
– If a woman have severe symptoms, pregnancy is not advised
8. Cystic Fibrosis
a recessively inherited disease in which there is generalized dysfunction of the
exocrine glands, this dysfunction leads to mucous secretions, particularly in the
pancreas and lungs, becoming so viscid or thick that normal lung and pancreatic
function is compromised
men with cystic fibrosis are sterile because their semen is so thick that sperm
cannot be motile
Women may have lessened fertility due to thickened cervical mucus
inability to digest fat and protein because the pancreas cannot release amylase.
Increased risk of preterm labor and perinatal death
Treatment: pancrelipase to supply pancreatic enzyme,, bronchodilator, chest
physiotherapy
Because pancrelipase may interfere with iron absorption, a woman is at greater risk
for iron-deficiency anemia during pregnancy than other women
Persons with cystic fibrosis have a higher-than-usual incidence of developing
diabetes mellitus because of pancreas involvement
e. Rheumatic Disorders And Pregnancy
1. Rheumatoid Arthritis
Juvenile rheumatoid arthritis (chronic rheumatoid arthritis), a disease of
connective tissue with joint inflammation and contracture, is most likely the result
of an autoimmune response
NUPC 110 Module II Page 12
pathology involves synovial membrane destruction, inflammation with effusion,
swelling, erythema, and painful motion of the joints
granulation tissue can fill the joint space
Treatment: corticosteroids, NSAIDs, aspirin
*use of salicylates (prolonged) may cause bleeding at birth and prolonged pregnancy
Salicylates interfere with prostaglandin synthesis
infant may be born with a bleeding defect and may also experience premature
closure of the ductus arteriosus because of the drug’s effects.
Symptoms of the disease may improve during pregnancy because of the naturally
increased circulating level of corticosteroids in the maternal bloodstream during
pregnancy
2. Systemic Lupus Erythematosus
a multisystem chronic disease of connective tissue that can occur in women of
child-bearing age: its highest incidence is in women aged 20 to 40 years
heart, kidneys, blood vessels, spleen, skin, and retroperitoneal tissue are affected
erythematous butterfly-shaped rash on the face
In the kidneys, fibrin deposits develop, plugging and blocking the glomeruli and
leading to necrosis and scarring.
thickening of collagen tissue in the blood vessels causes vessel obstruction
Treatment:
corticosteroid,
NSAIDs, heparin,
and salicylates
f. Gastrointestinal
Disorders And Pregnancy
1. Appendicitis
typical sharp,
peristaltic, lower
right quadrant
pain (McBurney’s
point), nausea and
vomiting
Advise a woman
not to take food,
liquid, or
laxatives while
she is waiting to CHANGE IN POSITION OF APPENDIX DURING
PREGNANCY
be evaluated for
possible appendicitis, because increasing peristalsis could cause an inflamed
appendix to rupture
• Surgery may be done if past 36 weeks and UTZ reveals a mature fetus
• Ruptured appendicitis may cause fecal material reach fetus thru fallopian tube;
generalized peritonitis may be difficult for a woman to combat and even
maintain pregnancy; peritoneal adhesions may cause subferility due to changes
in the location of fallopian tube
2. Gastroesophageal Reflux Disease or Hiatal Hernia
GERD refers to the reflux of acid stomach secretions into the esophagus
Hiatal hernia is a condition in which a portion of the stomach extends and
protrudes up through the diaphragm into the chest cavity, trapping stomach acid
and causing it to reflux into the esophagus
Symptoms include:
o Heartburn, which is particularly extreme when lying supine after a full meal
NUPC 110 Module II Page 13
o Gastric regurgitation
o Dysphagia (difficulty swallowing)
o Possible weight loss because of the inability to eat
o Hematemesis (vomiting of blood) if extreme esophageal irritation occurs from
the reflux of hydrochloric acid from the stomach
Treatment: Antacids, PPI, Histamine receptos antagonist
3. Cholecystitis and Cholelithiasis
most frequently associated with women older than 40 years, obesity, multiparity,
and ingestion of a high-fat diet
Signs and symptoms :constant aching and pressure in the right epigastrium,
perhaps accompanied by jaundice
Treatment: low-fat diet, surgery if nonsurgical management fails
4. Pancreatitis
inflammation of the pancreas
diagnosis may be difficult as serum amylase, which rises with pancreatitis, is also
normally elevated during pregnancy.
nasogastric suction, bowel rest, analgesia (pancreatic pain is sharp), and
intravenous hydration through parenteral nutritional supplementation.
acidosis, hypovolemia, and fetal hypoxia
5. Hepatitis
Hepatitis is a liver disease that may occur from invasion of the A, B, C, D, or E
virus.
Hepatitis A is spread mainly by fecal–oral contact
o benign course and is not known to be transmitted to the fetus.
Hepatitis B and C are spread by exposure to contaminated blood or blood products.
Hepatitis D and E are apparently spread by the same methods as hepatitis B but are
rarely seen in pregnant women.
may lead to spontaneous miscarriage or preterm labor.
6. Inflammatory Bowel Disease
Crohn’s disease (inflammation of the terminal ileus) and ulcerative colitis
(inflammation of the distal colon) can also be seen in pregnancy
associated with passiveand active smoking
A woman experiences chronic diarrhea, weight loss, occult blood in stool, and
nausea and vomiting
with Crohn’s disease, malabsorption, particularly of vitamin B occurs
Management: Monitor for weight gain,TPN, sulfasalazine
g. Neurologic Disorders And Pregnancy
1. Seizure Disorder
anoxia may deprive fetus of oxygen
The risk of adverse maternal or fetal outcome from seizures during pregnancyis
greater than the risk of teratogenicity from taking anticonvulsant drugs
Drugs used: Trimethadione, Valproic acid, Carbamazepine, Ethosuximide, Phenytoin
sodium
o Dilantin can cause a syndrome involving fetal cognitive impairment and a
peculiar facial proportion not unlike that of fetal alcohol syndrome. This
may occur because of competition for folic acid binding sites. Some
infants have an increased danger of neural tube disorders as a result of
this folic acid displacement. An ultrasound can rule out the possibility of
this.
o Infants are also prone to hemorrhagic disease of the newborn because
of decreased levels of vitamin K coagulation factors at birth from
phenytoin. To counteract this, women maybe prescribed vitamin K
during labor or the last 4 weeks of gestation. Women who have been
taking phenytoin (Dilantin) may have developed chronic hypertension.
NUPC 110 Module II Page 14
o
2. Myasthenia Gravis
an autoimmune disorder characterized by the presence of an IgG antibody
against acetylcholine receptors in striated muscle.
treated with anticholinesterase drugs such as pyridostigmine (Mestinon) or
neostigmine(Prostigmin) and a corticosteroid prednisone; Plasmapheresis
Smooth muscles are not affected
NO MgSO4
3. Multiple Sclerosis
occurs predominantly in women of childbearing age, usually between 20 and 40
years of age
nerve fibers become demyelinated and therefore lose function
Women develop symptoms of fatigue, numbness, blurred vision, and loss of
coordination
Tx: ACTH or corticosteroid to strengthen nerve function
May improve during pregnancy
h. Musculoskeletal Disorders And Pregnancy
1. Scoliosis
lateral curvature of the spine
Deformity interferes with respiration and heart action because of chest compression
Pelvic distortion can interfere with childbirth, especially at the pelvic inlet
If a woman’s spine is extremely curved, spinal or epidural anesthesia may be
difficult to administer for pain management in labor
o cephalopelvic disproportion
Treatment: stainless steel rods and correction brace
i. Endocrine Disorders And Pregnancy
1. Thyroid Dysfunction
thyroid slightly increase in size during pregnancy
Hypothyroidism
– a rare condition in young adults and especially in pregnancy
– May lead to early spontaneous miscarriage
– may be associated with an increased incidence of extreme nausea and vomiting
– Treatment: levothyroxine
o her dose of levothyroxine will need to be increased as much as 20% to 30%
for the du-ration of the pregnancy to simulate the increase that would
normally occur in pregnancy
o separate thyroxine ingestion from any medication containing iron, calcium,
or soy products by about 4 hours to be sure that there is no problem with
the absorption of thyroxine
o Dose should be tapered back after pregnancy
Hyperthyroidism (Grave’s Disease)
– overproduction of thyroid hormone
– more prone to symptoms of hypertension of pregnancy, fetal growth restriction,
and preterm labor than the average woman
– Radioactive
Iodine uptake
(RAIU) to test
thyroid function,
should not be
done during
pregnancy as it
may destroy
fetal thyroid
NUPC 110 Module II Page 15
– Treatment: PTU to reduce thyroid activity, methimazole during pregnancy
– infant may be born with symptoms of hyperthyroidism
– Woman with minimal dose may breastfeed their infant, but not with woman
taking large dose as it may be passed into the breastmilk.
2. Diabetes Mellitus
an endocrine disorder in which
the pancreas cannot produce
adequate insulin to regulate
body glucose levels
leading cause of kidney failure,
non-traumatic lower-limb
amputations, and new cases of
blindness among adults in the
United States
Gestational diabetes occurs at
20th week of pregnancy; affects
3% to 5% of all pregnancies and
is the most frequently seen
medical condition in pregnancy,
Before insulin was produced
synthetically in 1921, women
with type 1 diabetes, or diabetes
acquired in childhood, died
before reaching childbearing
age, were infertile, or had
spontaneous miscarriages early
in pregnancy
Now that diabetes can be well
managed and type 2 diabetes is
occurring more frequently in
young adults, four new problems have developed:
o How to care for women with both type 1 and type 2 diabetes during pregnancy
o How to bring a woman with type 1, type 2, and gestational diabetes through a
pregnancy with good glucose and insulin control
o How to protect an infant in utero from the adverse effects of the increased glucose
levels
o How to care for the infant in the first 24 hours after birth until the infant’s insulin-
glucose regulatory mechanism stabilizes
Infants of diabetic women are five times more apt to be born with heart anomalies
Type 1 diabetes (DM I) is due to pancreatic islet B cell destruction predominantly by an
autoimmune process, and these persons are prone to ketoacidosis
Type 2 diabetes (DM II) is the more prevalent form and results from insulin resistance
with a defect in compensatory insulin secretion
o As the need for insulin rises, the pancreas gradually loses its ability to produce it.
o hyperglycemia and resulting from the combination of resistance to insulin action,
inadequate insulin secretion, and excessive or inappropriate glucagon secretion
All women appear to develop an insulin resistance as pregnancy progresses or insulin
does not seem as effective during pregnancy, a phenomenon that is probably caused by
the presence of the hormone human placental lactogen (chorionic
NUPC 110 Module II Page 16
somatomammotropin)and high levels of cortisol, estrogen, progesterone, and
catecholamines
3 P’s of DM
o Polyuria
o Polyphagia
o Polydipsia
continued use of glucose by the fetus may lead to hypoglycemia for the mother
between meals
An increase in the amount of amniotic fluid occurs in at least 25% of diabetic women
a woman is at greater risk for pregnancy-induced hypertension and infection
Infants of women with poorly controlled diabetes tend to be large(>10 lb) because the
increased insulin the fetus must produce to counteract the overload of glucose he or
she receives acts as a growth stimulant
o A macrosomic infant may create birth problems like cephalopelvic disproportion
and shoulder dystocia, thus, CS birth
o There is a high incidence of congenital anomaly, especially caudal regression
syndrome (failure of the lower extremities to develop), spontaneous miscarriage,
and stillbirth in infants of women with uncontrolled diabetes
o At birth, the neonates are more prone to hypoglycemia, respiratory distress
syndrome,hypocalcemia, and hyperbilirubinemia
Monitoring DM patients
o glycosylated haemoglobin (HbA1C) is used to detect the degree of hyperglycemia
present
o The upper normal level of HbA is 6% of total hemoglobin
o Fasting plasma glucose 126 mg/dL or nonfasting of 200 mg/dL – Diabetes
o Opthalmic examination to be done every trimester as DM causes retinal changes
o Treatment: insulin, blood glucose monitoring (A fasting blood glucose level below
95 to 100 mg/dL and a 2-hour postprandial level below 120 mg/dL are well-
adjusted values)
Hypoglycemia – intake of complex carbs and less concentrated fluid to prevent
rebound hyperglycemia
Acidosis should be prevented as maternal acidosis may lead to fetal anoxia
The most common time during pregnancy for hypoglycemia is the second and third
months, before insulin resistance peaks; for hyperglycemia, it is the 6th month, or the
time insulin resistance is becoming most pronounced.
Tests for Placental Function and Fetal Well-Being
o MSAFP
o UTZ
o Creatinine clearance
– A normal creatinine clearance rate suggests that a woman’s vascular system
is intact because kidney function is normal, this implies that uterine
perfusion is also adequate
o Nonstress test
o Daily movements of fetus (atleast 10 movements per hour)
o Oligohydramnios may indicate fetal growth restriction or fetal renal abnormality,
whereas hydramnios may indicate gastrointestinal malformation or poorly
controlled disease
o L-S Ratio for fetal maturity (>2.0 to 2.5)
CS birth for macrosomic babies/ shoulder dystocia
CS poses increased risk for RDS in newborns due to immature lung surfactant
Termination of pregnancy before was done to prevent fetal loss from placental
insufficiency
i. Mental Illness And Pregnancy
NUPC 110 Module II Page 17
Schizophrenia tends to have its highest incidence in adolescents and young adults and
so occurs in young pregnant women
Depression occurs almost four times more commonly in women than in men, and often
in young adults.
It is the most common mental illness seen in pregnant women.
lithium, a mainstay of therapy for mood disorders such as bipolar disorder (manic
depression),and serotonin-reuptake inhibitors used to counteract depression, are
potentially teratogenic
j. Cancer And Pregnancy
Cancer occurs in about 1 in 1000 pregnancies
most commonly seen with pregnancy are:
o Cervical
o Breast
o Ovarian
o Thyroid
o Leukemia
Melanoma
o Lymphomas
If a woman is in the first trimester of pregnancy when a malignancy is diagnosed, she
and her partner are asked to make a difficult decision: to delay treatment to avoid
teratogenic risks to a fetus from treatment (possibly increasing a woman’s risk); to end
the pregnancy to allow chemotherapy or radiation treatment to be initiated; or to
choose chemotherapy or radiation treatment with the knowledge that they may cause
birth anomalies in the fetus
As a rule, women can receive chemotherapy in the second and third trimesters without
adverse fetal effects
Radiation therapy, in contrast, puts the fetus at risk throughout pregnancy ift he fetus
is directly exposed
Melanoma is the only type of cancer that seems capable of spreading to the fetus
Placenta serves as a barrier to other types of cancer and fetus has the ability to resist
invading foreign cells
LESSON 2: Nursing Care of Clients with Special Needs
THE PREGNANT ADOLESCENT
• Reasons for the high number of teenage pregnancy:
– Earlier age of menarche in girls (the average age is 12.4 years; many girls begin
menstruating at age 10 and so are ovulating and able to conceive by age 11)
– Increase in the rate of sexual activity among teenagers
– Lack of knowledge about (or failure to use) contraceptives or abstinence
– Desire by young girls to have a child
• Developmental Task of Adolescent:
– to establish a sense of self-worth or a value system, to emancipate from parents, to
adjust to a new body image, and to choose a vocation (Erikson, 1963)
NUPC 110 Module II Page 18
– Adolescents are emancipated minor or mature minor —a person capable of making
health care decisions—and so may sign permission for her own care
• Prenatal Assessment
– high incidence of pregnancy-induced hypertension, iron-deficiency anemia, and
premature labor
– higher incidence of low-birth-weight infants, a disproportion between fetal and
pelvic size, and a high rate of intimate partner abuse
– Health History
– Physical Examination
Pregnancy Education
– Proper nutrition
– Enough activity and rest
– Educate about physiologic changes
– Childbirth Preparation
• Childbirth education classes
– Birth Decisions
– Plans for the Baby
• Factors contributing to the lack of prenatal care include:
– Denial she is pregnant
– Lack of knowledge of the importance of prenatal care
– Dependence on others for transportation
– Feeling awkward in a prenatal setting (an adult setting)
– Fear of a first pelvic examination
– Difficulty relating to authority figures
• Complications of Adolescent Pregnancy
– PIH
• Promote bed rest
– IDA
• their low protein intake cannot balance the amount of iron lost with
menstrual flows
• reticulocyte count may be obtained in 2 weeks to evaluate these levels and
provide evidence that the iron supplement is being taken
• Associated with pica
– Preterm Labor
• explain the process of true labor and report any vaginal bleeding
Complications of Adolescent Labor, Birth, and the Postpartum Period
1. Cephalopelvic Disproportion
• suggested by lack of engagement at the beginning of labor, a prolonged first stage
of labor, and poor fetal descent
• Graphing labor progress is a good way to detect labor that is becoming abnormal
2. Pospartum Hemorrhage
• Immature uterus overdistends causing ineffective contractions and bleeding
3. Inability to Adapt Postpartally
• Postpartum Depression is more apt to occur in adolescent particularly frightened
by labor
• Urge her to talk about labor and birth to make the happening real to her
4. Lack of Knowledge About Infant Care
• Educate teenage mother the importance of breastfeeding and how to incorporate it
into a busy lifestyle
• Demonstrate bathing and changing the baby as appropriate
THE PREGNANT WOMAN OVER AGE 40
• A woman over age 40 is more likely than a younger woman to have a previously diagnosed
condition, such as hypertension, varicosities, or hemorrhoids
• Developmental Tasks and Pregnancy:
– to expand their awareness or develop generativity—that is, a sense of moving away
from themselves and becoming involved with the world or community (Erikson,
1963)
• Prenatal Assessment
– Health History
– Physical Examination
NUPC 110 Module II Page 19
– Chromosomal Assessment
• triple-screen (alpha-fetoprotein [AFP], human chorionic gonadotropin,
and unconjugated estriol levels) at the 15th week to detect whether an
open spinal cord or chromosomal defect could be present in the fetus,
• Pregnancy Education
– Nutrition
• substitute a caffeine-free soft drink in place of an alcoholic beverage.
• Puddings or yogurt in place of milk as Ca supplement
– Prenatal classes
• join a childbirth preparation or prenatal exercise class where she is “one of
the groups”
Complications of Pregnancy for a Woman Over Age 40
• PIH
– possibly related to blood vessel inelasticity or because hypertension tends to occur
more frequently in nulliparas than in multiparas as well as those with already
elevated blood pressure
– rest for a good portion of each day to reduce symptoms
Complications of Labor, Birth, and the Postpartum Period for a Woman Over Age 40
1. Failure to Progress in Labor
– cervical dilatation may not occur as spontaneously as in a younger woman
– Graphing labor progress is a good method to use to determine when labor is
becoming prolonged
2. Difficulty Accepting the Event
– Women over age 40 may begin to have second thoughts about childbearing this late
in life as the reality of a new baby registers with them during the intrapartal and
postpartum periods
3. Postpartum Hemorrhage
– Uterus does not contract effectively due to inelasticity
THE PREGNANT WOMAN WHO IS PHYSICALLY OR COGNITIVELY CHALLENGED
• women with conditions such as vision, hearing, cognitive, neurologic, or orthopedic
challenges
• women with a physical or cognitive disability or illness should come for preconceptual
care so medicines they are taking can be evaluated and careful planning for safe
pregnancy care can be started early
• Rights of the Physically or Cognitively Challenged Person
• Physically disabled persons must have freedom of access to public buildings by means of
ramps or handrails
• All public health care facilities must be in compliance with these laws both in terms of
physical facilities and in the true spirit of the law: that is, people should be made to feel
psychologically welcome as well as physically able to reach the inside of the building
• a hospital cannot deny care to a person with a disability even though the disabling
condition complicates treatment considerably, possibly requiring extra personnel and time.
• A woman with a disability has full rights to her child, so the baby cannot be taken from her
at birth without her full consent
• she cannot be forced to terminate a pregnancy or undergo sterilization unless that is her
informed decision
• Modifications for Pregnancy
• Explore with women at a first prenatal visit the exact nature of their disability and their
general self-image to identify what modifications they may need in care during pregnancy
• If a woman is housebound, be certain that she is taking a prenatal vitamin containing
vitamin D as she is probably not receiving as much sun exposure as usual
• Safety Measures to Explore
– Emergency contacts
– Transportation
• Wheelchair – risk for pressure ulcer, poor venous return, thrombosis,
varicosities
• Use crutches or wheelchair for those who have problems with balance
– Elimination
• Encourage high fluid intake and frequent urination
NUPC 110 Module II Page 20
– Autonomic Responses
• Observe for Autonomic Dysreflexia, an exaggerated autonomic response to
stimuli
• Autonomic Dysreflexia
o Any irritating condition, such as a distended bladder, increasing uterine
size, labor contractions, or breastfeeding, may initiate the response
o severe hypertension (300/160 mm Hg), throbbing headache, flushing
of the skin and profuse diaphoresis above the level of the spinal lesion,
nausea, and bradycardia may occur
o Immediate action is necessary to protect against cerebrovascular
accident or intraocular damage
o Elevate a woman’s head to reduce cerebral pressure and locate the
irritating stimulus (usually a distended bladder or bowel)
o antihypertensive agent to alleviate the extreme hypertension
• Prenatal Care Modifications to Meet Specific Needs
– Adjust table level for easy access (from wheelchair)
– Explain the procedure (e.g., pelvic exam) and its importance
– always alert a woman (visually challenged) when you are going to touch her, so as
not to startle her
• Pregnancy Education
– tape recording of any information you particularly want a woman to remember, or
she seems concerned about (visually challenged)
– Limit instructions to those few items crucial for safety (cognitively challenged)
– Use printed words (hearing challenged)
– Nutritional education
– Activity and exercise
• Modifications for Labor and Birth
– A woman with a spinal cord injury may not be able to feel uterine contractions.
Late in pregnancy, she will need to palpate her abdomen periodically for tightening
or the presence of contractions, so she is aware of beginning labor.
– Women with muscle spasticity or spinal cord injury may not be able to push
effectively for the second stage of labor and so may need cesarean or forceps birth.
– If a woman cannot assume a lithotomy position because of hip contracture, vaginal
delivery from a Sims’ or dorsal recumbent position is best.
– Braille watches used by visually challenged persons may not have second hands.
They may need to time the length of contractions by counting rather than timing
them by a watch.
– During labor, the hearing-challenged woman cannot hear information on how she is
progressing if you are not directly facing her. If she needs to communicate with her
support person in sign language, act as an advocate to keep her hands
unencumbered by equipment such as intravenous lines. Remember she cannot hear
her infant cry at birth. Hand the infant to her as soon as possible after birth so she
can see and feel the baby is crying and breathing well.
– Be certain to identify the usual sounds of birthing rooms (the beeping of a monitor,
the swish of a central supply routing system, and so forth) for the visually
challenged woman. Hearing sounds and not being able to identify them can be
frightening.
• Modifications for Postpartum Care
– After birth, be sure to assess and teach:
o Whether a woman desires contraceptive information.
o Whether she needs additional support to be successful at breastfeeding.
o Whether she has a return appointment for both herself and her infant for
follow-up care and that the arrangements are within her capabilities,
transportation, and understanding.
• Modifications for Planning Child Care
– Allow for extra time during the first days after birth for mother–child interaction
– Breastfeeding has special advantages for women who are physically or cognitively
challenged because it is the method of feeding that is not only best for the baby,
but also requires the least preparation effort on the mother’s part
– Encourage women to think through what baby care equipment will be best for them
– Using an anterior baby sling is usually effective with a wheelchair.
NUPC 110 Module II Page 21
– Encourage a woman to develop a habit of turning on lights after dinner because her
infant will need light to develop vision
– You have a legal obligation to investigate whether a newborn will receive safe care
before hospital discharge. Be certain to ask enough questions so that you are sure a
woman who is severely cognitively challenged, for example, has a responsible
friend or partner to help her with child care
A WOMAN WHO IS SUBSTANCE DEPENDENT
• Substance abuse is defined as the inability to meet major role obligations, an increase in
legal problems or risk-taking behavior, or exposure to hazardous situations because of an
addicting substance
• A person is substance dependent when he or she has withdrawal symptoms following
discontinuation of the substance, combined with abandonment of important activities,
spending increased time in activities related to substance use, using substances for a
longer time than planned, or continued use despite worsening problems because of
substance use.
• As many as 10% to 20% of pregnant women use illegal drugs during pregnancy
• Adolescents have an increased rate of inhalant abuse and binge drinking
• Illicit drugs tend to be of small molecular weight, so they readily cross the placenta
– a fetus of an addicted mother has a drug concentration of about 50% that of the
mother
• drug abuse can account for fetal abnormalities or preterm birth
• Injected drugs pose higher risk of hepatitis and HIV infections
• a woman may earn money to buy drugs through prostitution, which increases the risk for
sexually transmitted infection and poses an additional threat to a fetus.
Common Substances Abused During Pregnancy
• Cocaine
– derived from Erythroxylum coca, a plant grown almost exclusively in South
America
– cocaine is absorbed across the mucous membranes to affect the central nervous
system – sudden vasoconstriction occurs
• Respiratory and cardiac rates and blood pressure increase rapidly in
response to the vasoconstriction
• Immediate death may result from cardiac failure
– Alkaloidal cocaine (crack) – more concentrated, causing more rapid and intense
effect when inhaled
• extreme vasoconstriction can severely compromise placental circulation,
leading to premature separation of the placenta, which then results in
preterm labor or fetal death
– Infants born to cocaine-dependent women may suffer the immediate effects of
intracranial hemorrhage and a withdrawal syndrome of tremulousness, irritability,
and muscle rigidity
– Learning defects as long-term effects
– Cocaine metabolites can be detected in urine up to 1 week after use
• Amphetamines
– Methamphetamine (speed) has a pharmacologic effect similar to cocaine.
– Its use is becoming more common because it is easily and cheaply manufactured
– Ice, a rock type of methamphetamine that is smoked, can produce high
concentrations of drug in the maternal circulation.
• Newborns whose mothers used the drug show jitteriness and poor feeding at
birth and may be growth restricted
• Marijuana and Hashish
– obtained from the hemp plant, cannabis
– produce tachycardia and a sense of well-being
– some women use marijuana to counteract nausea in early pregnancy
– associated with loss of short-term memory and an increased incidence of
respiratory infection in adults
– Causes reduced milk production; can be excreted in breastmilk
• Phencyclidine
– Phencyclidine (PCP) is an animal tranquilizer that is a frequently used street drug
in polydrug abuse.
– It causes increased cardiac output and a sense of euphoria.
– It has the potential for causing long-term hallucinations (flashback episodes).
NUPC 110 Module II Page 22
– PCP tends to leave the maternal circulation and concentrate in fetal cells, so it may
be particularly injurious to a fetus.
• Narcotic Agonists
– Narcotic agonists, used for the treatment of pain (e.g., morphine or meperidine
[Demerol]) and cough suppression (codeine), are also widely abused because of
their potent analgesic and euphoric effect
– Heroin – A short-acting narcotic, is inactive until it crosses the blood–brain barrier
(which it does more quickly than morphine)
• may be administered intradermally (“skin popping”), through inhalation
(“snorting”), or intravenously (“shooting”)
• produces an immediate and short-lived feeling of euphoria followed by
sedation
• Pregnancy complications related to its use include pregnancy-induced
hypertension and, because narcotics are often injected with shared needles,
phlebitis, subacute bacterial endocarditis, and hepatitis B and HIV infection
– Withdrawal symptoms include nausea, vomiting, diarrhea, abdominal pain,
hypertension, restlessness, shivering, insomnia, body aches, and muscle jerks
• Withdrawal symptoms may begin as soon as 6 hours after the last drug dose
and can continue for several days
– Heroin abuse in the pregnant woman can result in fetal opiate dependence and
severe withdrawal symptoms in the infant after birth
– Infants tend to be small for gestational age and have an increased incidence of
fetal distress and meconium aspiration
– fetal liver is forced to mature faster than normal because it forced to process the
drugs taken by the mother
– Fetal lung tissue also appears to mature more rapidly than usual, apparently from
the stress of the intrauterine drug exposure
• newborns of substance-abusing women seem better able to cope with
bilirubin at birth than other babies; hyperbilirubinemia is therefore rarely a
problem
– Infants of women taking methadone do not escape withdrawal symptoms at birth
• Inhalants
– Inhalant abuse refers to the “sniffing” or “huffing” of aerosol drugs.
– Frequently abused substances include airplane glue, cooking sprays, and computer
keyboard cleaner.
– Most of these substances contain freon as a propellant and can lead to severe
respiratory and cardiac irregularities.
– The effect of these drugs during pregnancy is not well documented, but they
appear to have effects similar to alcohol abuse.
– The respiratory depression they can cause could be enough to limit the fetal oxygen
supply to a serious level.
• Alcohol
– just as detrimental to fetal growth as illegal drugs.
– Excessive use tends to occur in women with impulsive personalities
– There is little documentation regarding how much alcohol must be ingested before
fetal alcohol syndrome, a syndrome with significant facial features, possible
cognitive challenges and memory deficits, occurs, so women are advised to drink no
alcohol during pregnancy
– When discussing alcohol ingestion with young adults, be certain to talk about binge
drinking (five or more alcohol drinks on one occasion) to be certain a woman does
not believe this type of occasional drinking is safe during pregnancy
TRAUMA AND PREGNANCY
• Trauma – injury by force
• automobile accidents, homicide, and suicide are among the leading causes of death
• incidence of trauma is 6% to 7% (as many as 250,000 pregnant women experience trauma
per year)
• A high incidence occurs during the last trimester because of poor balance and fainting from
hyperventilation
• Trauma from intimate partner abuse
• Preventing Accidents
– Accidents occur more frequently in people under stress
NUPC 110 Module II Page 23
– Pregnancy counseling should include education about ways to avoid accidents and
trauma such as automobile seat belt use
• Physiologic Changes in Pregnancy That Affect Trauma Care
– A primary rule to remember is that after a traumatic injury, a woman’s body will
maintain her own homeostasis at the expense of the fetus
– A woman’s total plasma volume increases during pregnancy from approximately
2600 mL to 4000 mL at term
– Central venous pressure (normal is 0 to 5 cm H2O in a nonpregnant state) is
increased to 2 to 7 cm H2O
– cardiac output increases from 1 L/min early in pregnancy to 6 to 7 L/min in the
second trimester
– heart rate increases 15 to 20 beats above normal
– Peripheral venous pressure in the pregnant woman is unchanged. However, it
tends to be higher in the lower extremities because of compression by the uterus on
the vena cava that causes back-pressure
• lacerations of the legs or perineum bleed much more profusely than usual
– Peripheral blood flow in general is increased because of decreased peripheral
vascular resistance (the effect of estrogen and decreased sympathetic activity all
through pregnancy).
• the pregnant woman can be in severe shock, yet her extremities will still
not feel cold and clammy
– leukocyte count rises (to 20,000 mm3 at term)
– serum albumin level decreases during pregnancy
– Serum liver enzyme levels (i.e., serum glutamicoxaloacetic transaminase, serum
glutamate pyruvate transaminase, and lactate dehydrogenase) remain the same
– Abdominal pain is difficult to localize during pregnancy because organs are pushed
aside by the growing uterus
• Culdocentesis, or needle aspiration through the posterior vaginal fornix into
the peritoneal cavity, may be done to assess for peritoneal bleeding
• Peritoneal lavage (the process of inserting a peritoneal dialysis catheter
into the abdominal cavity, adding a quantity of an isotonic solution,
aspirating it again, and analyzing it for blood or urine) may reveal bleeding
or bladder rupture best
– The bladder of a pregnant woman is extremely susceptible to rupture because it
is the most anterior organ and is elevated abnormally.
• After abdominal trauma, an indwelling bladder catheter is often inserted to
assess for blood in the urine
• Psychosocial Considerations
– A feeling of guilt lowers her self-esteem and can increase her level of stress.
• people under stress do not process information well and may not perceive
correctly the information given to them
• Assessment
– include both her psychological and physical status
– Have her support people around
– Health History
• Document the circumstances of the trauma: what happened, the time of
the injury, signs and symptoms of injury she is experiencing, and actions
she has taken to counteract these
• evaluate whether a woman’s degree of injury is in proportion to the history
• Physical Examination
– Accidents become fatal when lung, heart, kidney, or brain function becomes
inadequate; fetal health is in jeopardy when uteroplacental function is impaired
• After trauma, evaluate these systems first
– Following trauma:
• NGT to empty the stomach
• IFC to empty bladder and rule out a ruptured bladder
• To prevent supine hypotension syndrome, be certain a woman does not lie
supine for an examination
• Therapeutic Management
– Assess for consciousness
– Assess ABC
– (+) pulse, (-) breathing
• Rescue breathing
NUPC 110 Module II Page 24
– (-) pulse (-) breathing
• CPR
• 30:2
– Central line for IVF
– Ephedrine (drug of choice) to restore blood pressure
• Dopamine (second drug) at low doses
1. Open Wounds
– Lacerations
• A laceration (a jagged cut) may involve only the skin layer or may penetrate
to deeper subcutaneous tissue or tendons.
• Lacerations generally bleed profusely.
• Halt bleeding by putting pressure on the edges of the laceration
• After cleaning, the area is sutured through each layer of tissue involved to
approximate the edges.
• Lidocaine as local anesthesia can be used
• Butterfly strip for superficial lacerations
– Puncture Wounds
• penetration of a sharp object such as a nail, splinter, nail file, or knife.
• Puncture wounds bleed little
• If a woman has had a tetanus immunization within the past 10 years,
tetanus toxoid is administered.
• If a woman has not had a tetanus immunization within 10 years (the usual
condition), tetanus toxoid plus immune tetanus globulin are administered
– Fistulogram to determine the depth and extent of a wound
• involves inserting a thin catheter into the wound; the wound is then filled
with a radiopaque solution.
• A radiograph of the area filled by the solution reveals the extent of the
puncture
– Exploratory surgery if abdominal bleeding is suspected
– Diaphragmatic hernia may result from a cut in the diaphragm
• cesarean birth may be planned to avoid strain on the newly repaired
diaphragm during labor
2. Animal or Snake Bites
– Animal bites produce a form of puncture wound, so if the rabies immunization
status of the dog is known, the wound is washed and treated as a puncture wound.
• If the dog cannot be located or is proved to be rabid after 48 hours of
observation, a woman must be administered rabies immune globulin and
vaccine
– anti-venom serum for snake bites
3. Blunt Abdominal Trauma
– occurs generally from automobile accidents, when a woman’s abdomen strikes the
steering wheel or dashboard, or from someone kicking or punching her abdomen
– No visible break in the skin
– Edema or ecchymosis or hematoma on site
– Peritoneal lavage or UTZ to check for internal bleeding
– May cause abruptio or preterm labor
• Assess FHT, palpate uterus for abnormal contours
• Terbutaline to halt labor
• Pelvic exam to assess for vaginal bleeding or PROM
• Isoimmunization may occur: RhIG to Rh negative mother
4. Gunshot Wounds
– inspection for the point where the bullet entered the body and the point where it
exited (the entry wound is small but the exit wound is large because as a bullet
slows, it begins to tumble, enlarging the space it occupies)
– The uterine wall is so thick during pregnancy that it may trap a bullet
– Gunshot wounds are surgically cleaned and débrided, and a woman is treated with a
high-dose antibiotic (Ampicillin)
– If a bullet enters the uterus, the incidence of fetal mortality is high, especially if
the placenta is torn by the bullet
– investigate carefully the circumstances of the injury
5. Poisoning
– Food poisoning from inadequately refrigerated or undercooked foods
6. Suicide attempt
NUPC 110 Module II Page 25
– Activated charcoal is the drug of choice to neutralize stomach poison
– investigate carefully the circumstances of the poisoning
7. Choking
– If a pregnant woman chokes on a piece of meat or any foreign object blocks her
airway, attempting to dislodge the object with a sudden upward thrust to the upper
abdomen is difficult.
– This is because of a lack of space between the uterus and the end of the sternum
and because the average person cannot reach from the rear around a woman’s
enlarged abdomen.
– Late in pregnancy, therefore, a rescuer might use successive chest thrusts instead.
8. Orthopedic Injuries
– Colles fracture – a serious wrist injury
• Apply ice to the area
• Radiograph to check for fracture
– Adolescent women have higher incidence of weakened knee cartilage or ligaments
(formerly thought of only as a football injury)
• During pregnancy, when all body cartilage softens, combined with the
excessive abdominal weight a woman carries, a woman may dislocate her
knee or strain a knee ligament again
• support device such as a knee immobilizer may be required for the last 3
months of pregnancy to keep the joint from dislocating or the ligament from
tearing again
• laxness of body cartilage may also cause separation of the symphysis pubis
if a woman falls with her legs outspread
• Bedrest to relieve pain and promote healing
• Very painful if present during labor
9. Burns
– Burns are dangerous in the pregnant woman not only because of the thermal injury
that occurs but because of inhalation of carbon monoxide gases from the fire,
which could lead to extreme fetal hypoxia as carbon monoxide crosses the
placenta in place of oxygen
– smoke is irritating to lung tissue and can result in extensive lung edema
• Additional fetal hypoxia
– Hypotension from hypovolemia due to fluid and electrolyte loss occurs
– Prostaglandin are produced and may cause preterm labor
– Both maternal and fetal prognoses are poor if burns cover more than 50% of body
surface area.
– burn tissue heals more quickly than normal during pregnancy
10. Postmortem Cesarean Birth
– If a pregnant woman does not survive serious trauma, it may still be possible for her
child to be born safely by a postmortem cesarean
– This is usually attempted if the fetus is past 24 weeks and less than 20 minutes
has passed since the mother died.
– Infant survival is best in these circumstances if no more than 5 minutes has
passed.
– By general practice, no consent is necessary for this procedure because the fetus is
assumed to want to live but cannot give consent.
– A classic cesarean incision is used.
– Personnel should be available to resuscitate the newborn immediately.
KEY POINTS
• Adolescent pregnancy is a major concern, because although it is decreasing in incidence, it
still occurs at a high rate and can interfere with the development of both an adolescent
and fetus. Nursing care needs to be individualized to meet the prepartal, intrapartal, and
postpartum needs of this age group. Helping adolescents view a pregnancy as a growth
experience can help them mature in their ability to parent.
• Women who delay childbearing until age 40 may need additional discussion time at
prenatal visits to help them incorporate a pregnancy into their lifestyle. They may need
NUPC 110 Module II Page 26
reminders to save time during the day for rest, particularly if at risk for pregnancy-induced
hypertension or varicosities.
• Women who are physically, cognitively, visually, or hearing challenged or who have a
spinal cord injury are apt to have special needs during pregnancy that must be addressed
by health care providers. Providing time for discussion early in pregnancy so these needs
can be identified and anticipated is an important role for nurses.
• Women who are physically or cognitively challenged may need help in adjusting their usual
regimen to pregnancy. Be certain they are aware of how to contact help in an emergency.
Ensure that all medications they are taking for their primary disorder are safe for use
during pregnancy.
• A woman who is substance dependent presents a unique challenge during pregnancy.
Encouraging her to decrease or halt her drug intake to safeguard the health of a fetus is a
short-term goal. Addressing her need to decrease drug intake for the remainder of her life
so she can be a quality parent is a long-term goal.
• A fetus of a woman who is substance dependent is at high risk because of the direct effects
of the drug and the indirect effects of an unhealthy lifestyle. Women should be encouraged
to join drug reduction maintenance programs if possible, to reduce fetal risk.
• Trauma in pregnancy results from sources such as violence, automobile accidents, and
falls. Women with traumatic injuries need to be carefully assessed to determine if intimate
partner abuse was the cause of the trauma
LESSON 3: Nursing Care of Clients with Sudden Pregnancy
Complication
The leading complications related directly to the pregnancy are thromboembolism,
hemorrhage, infection, pregnancy-induced hypertension, and ectopic pregnancy
A. BLEEDING DURING PREGNANCY
Hypovolemic shock occurs when 10% of blood volume, or approximately 2 units of blood,
have been lost; fetal distress occurs when 25% of blood volume is lost.
Important to know the baseline BP of patient
NUPC 110 Module II Page 27
1. SPONTANEOUS MISCARRIAGE
Abortion is the medical term for any interruption of a pregnancy before a fetus is
viable
viable fetus is usually defined as a fetus of more than 20 to 24 weeks of gestation or
one that weighs at least 500 g
A fetus born before this point is considered a miscarriage or premature or immature
birth
If interrupted spontaneously – miscarriage
Spontaneous miscarriage occurs in 15% to 30% of all pregnancies and arises from natural
causes
early miscarriage if it occurs before week 16 of pregnancy and a late miscarriage if it
occurs between weeks 16 and 24
Causes of Spontaneous Miscarriage
o most frequent: abnormal fetal development (teratogenic or chromosomal)
o Between 50% and 80% of fetuses aborted early have structural abnormalities
o rejection of the embryo through an immune response may occur
o implantation abnormalities, as up to 50% of zygotes probably never implant
securely because of inadequate endometrial formation or from an inappropriate
site of implantation
o Miscarriage may also occur if the corpus luteum on the ovary fails to produce
enough progesterone to maintain the decidua basalis
o Rubella, syphilis, poliomyelitis, cytomegalovirus, and toxoplasmosis
infections cross the placenta and may also cause early miscarriage
o Low production of estrogen and progesterone may cause endometrial lining to
slough off, PG are released and contractions and cervical dilatation occur
o Intake of Isotretinoin in first tri may cause miscarriage or fetal abnormality
o alcohol – may cause abnormal fetal growth and lead to miscarriage
Assessment:
o Presence of vaginal spotting
Treatment depends of symptoms
2. THREATENED ABORTION
Management:
o HCG levels may be tested (should be doubled, if not, poor placental function may
be suspected)
o Avoid strenuous activities for the next 48 hrs
o Coitus is restricted for two weeks
3. IMMINENT/INEVITABLE MISCARRIAGE
Threatened miscarriage occur with contractions and cervical dilatation
(-) FHT, (-) fetus on UTZ needs Vacuum extraction or D&C
After D&C, woman should be monitored for bleeding (# of pads used)
4. COMPLETE MISCARRIAGE
the entire products of conception (fetus, membranes, and placenta) are expelled
spontaneously without any assistance.
bleeding usually slows within 2 hours and then ceases within a few days after passage
of the products of conception.
5. INCOMPLETE ABORTION
part of the conceptus (usually the fetus) is expelled, but the membrane or placenta is
retained in the uterus
there is a danger of maternal hemorrhage as long as part of the conceptus is retained
in the uterus because the uterus cannot contract effectively
D&C to evacuate other products of conception
6. MISSED MISCARRIAGE
NUPC 110 Module II Page 28
AKA early pregnancy failure
fetus dies in the utero but not expelled
Fetus died 4-6 weeks before the onset of miscarriage (spontaneously occurs within two
weeks
if pregnancy is at 14 weeks, PG or cytotec may be given to induce labor.
Recurrent Pregnancy Loss
7. HABITUAL ABORTERS
Possible causes:
o Defective spermatozoa or ova
o Endocrine factors such as lowered levels of protein-bound iodine (PBI), butanol-
extractable iodine (BEI), and globulin-bound iodine (GBI); poor thyroid function; or
luteal phase defect
o Deviations of the uterus, such as septate or bicornuate uterus
o Resistance to uterine artery blood flow
o Chorioamnionitis or uterine infection
o Autoimmune disorders such as those involving lupus anticoagulant and
antiphospholipid antibodies
Complications of Miscarriage
Hemorrhage
o Spontaneous complete – Hemorrhage is rare
o Incomplete – major haemorrhage if with coagulation D/O like DIC
o WOF signs of Shock
Unusual odor or passing of large clots is abnormal
Bleeding – dark color to color serous fluid
Physician may give Methergin for uterine contraction
Infection
o tends to develop in women who have lost appreciable amounts of blood
o danger signs of infection: fever (>38˚C) , abdominal pain or tenderness, and a
foul vaginal discharge
o Usually caused by E. Coli
o Caution a woman to wipe her perineal area from front to back after voiding and
particularly after defecation to prevent the spread of bacteria from the rectal
area.
o Caution her not to use tampons to control vaginal discharge, because stasis of
any body fluid increases the risk of infection
o Most common: Endometritis – infection of the uterine lining
Septic Abortion
o an abortion that is complicated by infection
o uterus is a warm, moist, dark cavity, infectious organisms, once introduced,
grow rapidly in this environment, particularly if products of conception such as
necrotic membranes are still present.
o Symptoms: fever and crampy abdominal pain, and her uterus feels tender to
palpation.
o Infection, if not treated, can lead to toxic shock syndrome, septicemia,
kidney failure, and death
o Management:
– complete blood count, serum electrolytes, serum creatinine, blood type
and crossmatch, and cervical, vaginal, and urine cultures are obtained
– IFC to monitor urine output
– IVF to restore fluid volume
– high-dose, broad-spectrum antibiotic therapy (penicillin, gentamicin,
clindamycin)
NUPC 110 Module II Page 29
– CVP to monitor left atrial filling pressure and hemodynamic status.
– TT or tetanus immune globulin as prophylaxis
– D & C/ D & E to remove infected and necrotic tissue
– Infection following a septic abortion can be so severe that a woman
needs to be admitted to an intensive care setting for continuing care.
– Dopamine and digitalis may be necessary to maintain sufficient cardiac
output.
– Oxygen and perhaps ventilatory support may be necessary to maintain
respiratory function.
– uterine scarring or fibrotic scarring of the fallopian tubes may cause
infertility
Isoimmunization
o the production of antibodies against Rh-positive blood
o mother is Rh-negative and the fetus is Rh-positive
o After a miscarriage, because the blood type of the conceptus is unknown, all
women with Rh-negative blood should receive Rh (D antigen) immune globulin
(RhIG) to prevent the build up of antibodies in the event the conceptus was Rh-
positive
Powerlessness or Anxiety
o Assess a woman’s adjustment to a spontaneous miscarriage. Sadness and grief over
the loss or a feeling that a woman has lost control of her life is to be expected.
o Do not forget to assess a partner’s feelings as well, or that person’s grief over the
pregnancy loss can be missed.
B. ECTOPIC PREGNANCY
implantation occurs outside the uterine cavity
2nd most frequent cause of bleeding in first trimester
Most Common in fallopian tube (95%), but may also occur in the ovary or cervix
80% occur in the ampullar portion, 12% occur in the isthmus, and 8% are interstitial or
fimbrial
Risk factors: PID, smoking, IUD use, History of ectopic pregnancy
Assessment: UTZ or MRI will reveal an ectopic pregnancy
At 6-8 weeks, zygote grows large enough cause rupture of the FT.
If implantation is in the interstitial portion of the tube, rupture can cause severe
intraperitoneal bleeding which may lead to shock
a ruptured ectopic pregnancy is serious regardless of the site of implantation
Signs and Symptoms:
o sharp, stabbing pain in one of her lower abdominal quadrants at the time of
rupture, followed by scant vaginal spotting
o With placental dislodgment, progesterone secretion stops and the uterine
decidua begins to slough, causing additional bleeding
o Leukocytosis due to trauma
o Cullen’s Sign (umbilicus may develop a bluish tinge) may also be present
o Chandelier’s Sign – cervical motion tenderness/pain
o pain in her shoulders from blood in the peritoneal cavity causing irritation to the
phrenic nerve.
o A tender mass is usually palpable in Douglas’ cul-de-sac on vaginal examination
Treatment: oral – methotrexate, then leucovorin; mifepritone (abortifacient)
o Methotrexate – a folic acid antagonist chemotherapeutic agent
o Oral meds until hCG titer becomes negative
o If ruptured, surgical intervention is done (removal or ligation of the affected
tube)
Isoimmunization may occur
NUPC 110 Module II Page 30
Abdominal Pregnancy
o Fetus grows in pelvic cavity
o The danger of abdominal pregnancy is that the placenta will infiltrate and erode
a major blood vessel in the abdomen, leading to hemorrhage
o If implanted on the intestine, it may erode so deeply that it causes bowel
perforation and peritonitis.
o Fetus is also at high risk because without a good uterine blood supply, nutrients
may not reach the fetus in adequate amounts.
o The survival rate in an abdominal pregnancy is only approximately 60% because
of poor nutrient supply
o Increased threat of fetal deformity growth restriction if infant survives
o Laparotomy as birth procedure
o Placenta may be difficult to remove, it may be left in place and be absorbed in
2 – 3 months
C. GESTATIONAL TROPHOBLASTIC DISEASE(HYDATIDIFORM MOLE)
abnormal proliferation and then degeneration of the trophoblastic villi
As the cells degenerate, they become filled with fluid and appear as clear fluid-filled,
grape-sized vesicles; embryo fails to develop
Abnormal trophoblast cells must be identified because they are associated with
choriocarcinoma, a rapidly metastasizing malignancy
Risk Factors: tends to occur most often in women who have a low protein intake, in
women older than age 35 years, in women of Asian heritage, and in blood group A
women who marry blood group O men
Complete mole – all trophoblastic villi swell and become cystic
Partial mole – some of the villi form normally; a macerated embryo of approximately 9
weeks’ gestation may be present and fetal blood may be present in the villi
A partial mole has 69 chromosomes (a triploid formation in which there are three
chromosomes instead of two for every pair, one set supplied by an ovum that
apparently was fertilized by two sperm or an ovum fertilized by one sperm in which
meiosis or reduction division did not occur)
Assessment: uterus expand faster than normal
o Serum hCG: 1 to 2 million IU compared with a normal pregnancy level of
400,000 IU
o Symptoms of pregnancy-induced hypertension such as hypertension, edema, and
proteinuria may appear
o At approximately week 16 of pregnancy, it will identify itself with vaginal
bleeding.
Treatment: suction curettage
o hCG to be monitored every 2 weeks until normal then every 4 weeks for 6-12
months
Gradual declining hCG- no complication
3 times increase may suggest a malignant transformation occurring
Woman should use contraceptive for 1 year to prevent pregnancy
D. PREMATURE CERVICAL DILATATION/ INCOMPETENT CERVIX/ TRACHELOPLASTY/
CERVICAL STITCH
a cervix that dilates prematurely and therefore cannot hold a fetus until term
painless
first symptom is show (a pink-stained vaginal discharge) or increased pelvic pressure,
which may be followed by rupture of the membranes and discharge of the amniotic
fluid
occurs at approximately week 20 of pregnancy
Treatment: Cervical cerclage – done at 12 – 14 weeks
NUPC 110 Module II Page 31
o Mc Donald or Shirodkar Tie
o After cerclage surgery, women remain on bed rest (perhaps in a slight or
modified Trendelenburg position) for a few days to decrease pressure on the
new sutures.
E. PLACENTA PREVIA
placenta is implanted abnormally in the uterus
Most Common cause of painless bleeding in the third trimester
Four degrees:
o implantation in the lower rather than in the upper portion of the uterus (low-
lying placenta)
o Marginal implantation (the placenta edge approaches that of the cervical os)
o implantation that occludes a portion of the cervical os(partial placenta previa);
o implantation that totally obstructs the cervical os (total placenta previa)
Risk Factors: Increased parity, advanced maternal age, past cesarean births, past
uterine curettage, multiple gestation, and a male fetus are all associated with placenta
previa
increase in congenital fetal anomalies may occur if the low implantation does not
allow optimal fetal nutrition or oxygenation
Assessment: abrupt painless bright red vaginal bleeding
Complications: maternal hge, because placenta is loosened, fetal oxygen supply may
be compromised, preterm labor
Immediate care measures:
Be sure to assess:
o Duration of the pregnancy
o Time the bleeding began
o Woman’s estimation of the amount of blood—ask her to estimate in terms of
cups or tablespoons (a cup is 240 mL; a tablespoon is 15 mL)
o Whether there was accompanying pain
o Color of the blood (red blood indicates bleeding is fresh or is continuing)
o What she has done for the bleeding (if she inserted a tampon to halt the
bleeding, there may be hidden bleeding)
o Whether there were prior episodes of bleeding during the pregnancy
NUPC 110 Module II Page 32
o Whether she had prior cervical surgery for premature cervical dilatation
o Assess VS every 5 – 15 minutes
o Kleihauer-Betke Test
o IV therapy with large-gauge catheter
o Monitor urine output every hour
o Assess FHT
o Hemoglobin, hematocrit, prothrombin time, partial thromboplastin time,
fibrinogen, platelet count, type and cross-match, and antibody screen will be
assessed to establish baselines, detect a possible clotting disorder
Continuing Care Measures
o If bleeding continues, fetus is compromised and labor has begun, birth must be
accomplished regardless of the AOG
o If bleeding stopped, maternal VS stable, fetus is not compromised, AOG is less
than 36 weeks, birth may be delayed
F. ABRUPTIO PLACENTA
premature separation of the placenta
Occurs in about 10% of pregnancies
Most frequent cause of perinatal death
Predisposing factors: high parity, advanced maternal age, a short umbilical cord,
chronic hypertensive disease, pregnancy-induced hypertension, direct trauma (as from
an automobile accident or intimate partner abuse), vasoconstriction from cocaine or
cigarette use, and thrombophilitic conditions that lead to thrombosis such as
autoimmune antibodies, protein C, and factor V Leiden (a common inherited
thrombophilia that occurs in 5% of whites and 1% of blacks
May be caused by chrorioamnionitis
Assessment
o sharp, stabbing pain high in the uterine fundus as the initial separation occurs
o Uterine tenderness
o Couvelaire Uterus – hard or board like uterus
o May lead to DIC
Management
o Large-gauge IV catheter for fluid replacement
o oxygen to limit fetal anoxia.
o Monitor FHT
o Monitor maternal VS
o Fibrinogen determination
o Keep woman in lateral position
o No abdominal, vaginal and pelvic exam
o DIC – bleeding may occur (CS); fibrinogen or cryoprecipitate with fibrinogen to
elevate woman’s fibrinogen level
o Hysterectomy – to prevent exsanguination
NUPC 110 Module II Page 33
G. DISSEMINATED INTRAVASCULAR COAGULATION
an acquired disorder of blood clotting in which the fibrinogen level falls to below
effective limit
Signs ang Symptoms: easy bruising or bleeding from an intravenous site
Risk Factors: premature separation of the placenta, pregnancy-induced hypertension,
amniotic fluid embolism, placental retention, septic abortion, and retention of a dead
fetus
o currently thought to be initiated by tissue factor or thromboplastin, which is
released from trophoblastic or fetal tissue, or maternal decidua or
endothelium
Abnormal D-dimer result (fibrin) – occurs in 90% of patients with DIC
To stop the process of DIC, the underlying insult that began the phenomenon must be
halted
Heparin to stop clotting cascade
Platelet transfusion to restore platelets lost
H. PRETERM LABOR
labor that occurs before the end of week 37 of gestation
occurs in approximately 9% to 11% of all pregnancies
responsible for almost two-thirds of all infant deaths in the neonatal period
Preterm labor is always serious because if it results in the infant’s birth, the infant will
be immature
associated with dehydration, urinary tract infection, periodontal disease, and
chorioamnionitis
Other Risk Factors: those who receive inadequate prenatal care, those who continue
to work at strenuous jobs during pregnancy or perform shift work that leads to extreme
fatigue, intimate partner abuse, small born women (mother) with overweight partner
Sign and symptoms: persistent, dull, low backache; vaginal spotting; a feeling of pelvic
pressure or abdominal tightening; menstrual-like cramping; increased vaginal
discharge; uterine contractions; and intestinal cramping
Treatment/Management:
o Presence of shortened cervix and fibronectin, a protein produced by
trophoblast cells, in vaginal mucus predicts preterm contractions are ready to
occur
NUPC 110 Module II Page 34
o Bed rest to relieve pressure on the cervix
o IVF to maintain hydration
o DHN may lead to release of ADH and oxytocin
o vaginal and cervical culture to rule out infection
o Tocolytic agent (terbutaline, ritodrine) to halt labor
o limit strenuous activities
o adequate nutrition
o Corticosteroid for lung surfactant formation
o Betamethasone is preferred as it leads to lower rates of respiratory distress
syndrome or bronchopulmonary dysplasia in newborns
o Terbutaline should not be given to patients with GDM
o Oral tocolytics until 37 weeks or until fetal lung maturity is achieved
Fetal Assessment
o Daily fetal movement count
o FHT
Labor that cannot be halted
o ruptured membranes
o 50% effaced cervix, 3-4 cm dilated
o NSD with Episiotomy or CS to reduce pressure on the fetal head and reduce the
possibility of subdural or intra-ventricular hemorrhage from a vaginal birth
o Increased risk of cord prolapse with AROM
o Epidural for pain relief
o Immediate cord clamping to prevent additional blood in circulation
I. PRETERM RUPTURE OF MEMBRANES
rupture of fetal membranes with loss of amniotic fluid during pregnancy before 37
weeks
associated with infection of the membranes (chorioamnionitis)
occurs in 5% to 10% of pregnancies
Increased risk of uterine and fetal infection and cord prolapse (could also interfere
with fetal circulation)
Potter-like syndrome or distorted facial features and pulmonary hypoplasia from
pressure may occur with loss of amniotic fluid
Preterm labor may follow rupture of the membranes and end the pregnancy
Assessment:
o sudden gush of clear fluid from her vagina, with continued minimal leakage
o Nitrazine paper test to test the fluid
o Yellow to blue – amniotic fluid
o Yellow to yellow – urine
o Fern Test
o amniotic fluid – positive ferning on microscopic exam
o High levels of AFP in vagina confirms PROM
o cultures for Neisseria gonorrhoeae, Streptococcus B, and Chlamydia are
usually taken
o WBC and C-reactive protein increase with membrane rupture
o Avoid routine vaginal exam to decrease the risk for infection
o If labor dos not occur within 24 hours, it is induced (Oxytocin IV) as long as fetus
is mature enough to survive
Treatment/ Management
o Bed rest if fetus is not viable
o Corticosteroid
o Prophylactic antibiotics
NUPC 110 Module II Page 35
o Tocolytics if labor begins
o membranes can be resealed by use of a fibrin-based commercial sealant so they
are again intact
J. PREGNANCY-INDUCED HYPERTENSION
a condition in which vasospasm occurs during pregnancy in both small and large arteries
Signs and symptoms: HPN, proteinuria, edema
unique to pregnancy and occurs in 5% to 7% of pregnancies
highly correlated with the antiphospholipid syndrome or the presence of antiphospholipid
antibodies
Previously called Toxemia
occur most frequently in:
o Multiple pregnancy
o primiparas younger than 20 years or older than 40 years
women from low socioeconomic backgrounds (perhaps because of poor nutrition)
o those who have had five or more pregnancies
o those who have hydramnios
o those who have an underlying disease such as heart disease, diabetes with vessel
or renal involvement, and essential hypertension
Effects of PIH:
o There is reduced blood supply to organs, most markedly the kidney, pancreas,
liver, brain, and placenta.
o Poor placental perfusion
o Ischemia in the pancreas may result in epigastric pain and an elevated amylase–
creatinine ratio
o Spasm of the arteries in the retina leads to vision changes
o Vasospasm in the kidney increases blood flow resistance
o Extreme edema can lead to cerebral and pulmonary edema and seizures
(eclampsia)
o Thrombocytopenia occurs as platelets rush to sites of endothelial damage
Assessment
o Classic signs of PIH: vision changes, typically hypertension, proteinuria, and edema
o classified as gestational hypertension, mild pre-eclampsia, severe pre-eclampsia,
and eclampsia
Gestational Hypertension
o elevated blood pressure (140/90 mm Hg) but has no proteinuria or edema
Mild Pre-eclampsia
o has proteinuria (1+ or 2+) and blood pressure rises to 140/90 mm Hg, taken on
two occasions at least6 hours apart
o A second criterion for evaluating blood pressure is a systolic blood pressure greater
than 30 mm Hg and a diastolic pressure greater than 15 mm Hg above prepregnancy
values
o Orthostatic proteinuria – on long periods of standing, they excrete protein; at bed
rest, they do not
o Ask for as morning urine sample to confirm what causes proteinuria
o Edema because of the protein loss, sodium retention, and lowered glomerular
filtration rate
o weight gain of more than 2 lb/wk in the second trimester or 1 lb/wk in the third
trimester usually indicates abnormal tissue fluid retention
Severe Preeclampsia
o blood pressure rises to 160 mm Hg systolic and 110 mmHg diastolic or above on at
least two occasions 6 hours apart at bed rest (the position in which blood pressure
is lowest) or her diastolic pressure is 30 mm Hg above her prepregnancy level
NUPC 110 Module II Page 36
o Marked proteinuria, 3+ or 4+ on a random urine sample or more than 5 g in a 24-
hour sample, and extensive edema are also present.
o extreme edema (pitting edema)
o Some women have severe epigastric pain and nausea and vomiting, possibly
because of abdominal edema or ischemia to the pancreas and liver
o Shortness of breath if pulmonary edema develops
o visual disturbances such as blurred vision or seeing spots before the eyes, severe
headache and marked hyperreflexia and perhaps ankle clonus (a continued motion
of the foot) if cerebral edema develops
Eclampsia
o most severe classification of PIH
o cerebral edema is so acute that a grand-mal seizure (tonic-clonic) or coma occurs
o maternal mortality rate is as high as 20% from causes such as cerebral
hemorrhage, circulatory collapse, or renal failure
o Hypoxia and fetal acidosis – Poor fetal prognosis
o Vasospasm may cause premature separation of placenta
Nursing Interventions for a Woman With Mild PIH
o Monitor Antiplatelet Therapy
o Promote Bed Rest
o Promote Good Nutrition
o Provide Emotional Support
Nursing Interventions for a Woman With Severe PIH
o Support Bed Rest
o Monitor Maternal Well-being
o VS q 4
o Lab test
o Daily Hct (to monitor edema)
o Plasma Estriol levels to test placenta function
o Daily weight same time each day
o IFC to monitor urine output
o Monitor fetal well being
o Support a Nutritious Diet
o high in protein and moderate in sodium
o Administer Medications to Prevent Eclampsia
o hydralazine (Apresoline), labetalol (Normodyne), or nifedipine
o can cause maternal tachycardia. Therefore, assess pulse and blood pressure before
and after administration
o MgSO4
o a cathartic, reduces edema by causing a shift in fluid from the extracellular spaces
into the intestine
o Reduces blood pressure
o a central nervous system depressant (blocks peripheral neuromuscular transmission)
-- lessens the possibility of seizures
Magnesium Sulfate overdose
o decreased urine output, depressed respirations, reduced consciousness, and
decreased deep tendon reflexes
o If oliguria (less than 100 mL in 4 hours) results, excessively high serum levels of
magnesium can result
o Antidote: Calcium gluconate
o Before administration:
– urine output above 25 to 30 mL/hr, specific gravity of 1.010 or lower.
– Respirations above 12 per minute,
NUPC 110 Module II Page 37
– a woman should be able to answer questions asked of her such as her name
or address,
– ankle clonus (a continued motion of the foot) should be minimal,
– deep tendon reflexes should be present
Deep Tendon Reflexes
Pattelar reflex or knee jerk
Biceps or triceps reflex if with epidural anesthesia
o Oliguria – intravenous infusion of salt-poor albumin
o high-colloid solution will call fluid into the bloodstream from interstitial tissue by
osmotic pressure; the kidneys will then excrete the extra fluid along with
magnesium sulfate levels
MgSO4 IV
o crosses placenta and may cause respiratory depression
o Monitor FHT, WOF late decelerations
o UTZ to show fetal breathing movements
o Continued after delivery then tapered down
o Delay BF until drug is discontinued
o May cause osteoporosis
o Ca supplements
Nursing Interventions for a Woman With Eclampsia
o eclampsia occurs when cerebral irritation from increasing cerebral edema becomes
so acute that a seizure occurs
o happens late in pregnancy but can happen up to 48 hours after childbirth
o Immediately before a seizure:
o blood pressure rises suddenly from additional vasospasm.
o temperature rises sharply to 103° to 104° F (39.4° to 40° C) from increased
cerebral pressure
o blurring of vision or severe headache (from the increased cerebral edema)
o reflexes become hyperactive
o may experience a premonition that “something is happening”
o Vascular congestion of the liver or pancreas can lead to severe epigastric pain and
nausea
o Urinary output may decrease abruptly to less than 30 mL/hour
o Tonic-Clonic Seizures
– Tonic phase – After the preliminary signal or aura that something is
happening, all the muscles of the woman’s body contract
Respirations stop – cyanosis
Might bite her tongue from rapid closing of jaw
Lasts approx. 20 secs
– Clonic (second) phase – the woman’s bladder and bowel muscles contract
and relax; incontinence of urine and feces may occur
Breathing begins but ineffective, pt may remain cyanotic
Lasts up to 1 minute
– Postictal stage
woman is semicomatose and cannot be roused except by painful
stimuli for 1 to 4 hours
If placental separation occurs, labor may begin
painful stimulus of contractions may initiate another seizure
Keep NPO
Continuously assess fetal heart sounds and uterine contractions
Birth
NUPC 110 Module II Page 38
o There is some evidence that a fetus does not continue to grow after eclampsia
occurs, so terminating the pregnancy at this point is appropriate for both mother
and child.
o For an unexplained reason, fetal lung maturity appears to advance rapidly with
PIH (possibly from the intrauterine stress), so even though the fetus is younger than
36 weeks, the lecithin–sphingomyelin ratio may indicate fetal lung maturity
o a woman with eclampsia is not a good candidate for surgery
o Vaginal birth is preferred
Nursing Interventions During the Postpartum Period
o Postpartum hypertension may occur up to 10 to 14 days after birth, although it
usually occurs no more than 48 hours after birth
o Advise woman to return for postpartum check up
o Management of Seizure
o Maintain patent airway
o O2 via face mask to protect the fetus
o Turn to side to allow drainage of secretions
o MgSO4 or Diazepam (Valium)
o Assess O2 sat
o Fertal monitor to asses fetal status
o Check for vaginal bleeding (abruptio)
o Evidence of placental separation appears first in fetal status, then vaginal bleeding
K. HELLP SYNDROME
a variation of PIH named for the common symptoms that occur: hemolysis that leads to
anemia,elevated liver enzymes that lead to epigastric pain, and low platelets that lead
to abnormal bleeding/clotting and petechia
occurs in 4% to 12% of patients with PIH
May result in maternal mortality rate as high as 24% and an infant mortality rate as
high as 35%
occurs in both primigravidas and multigravidas
may be associated with an-tiphospholipid syndrome or the presence of antiphopholipid
antibodies
Signs and Symptoms: proteinuria, edema and increased blood pressure, additional
symptoms of nausea, epigastric pain, general malaise, and right upper quadrant
tenderness from liver inflammation
o hemolysis of red blood cells; thrombocytopenia; elevated liver enzyme levels
(alanine aminotransferase [ALT]and serum aspartate aminotransferase [AST]
close observation for bleeding
Complications: subcapsular liver hematoma, hyponatremia, renal failure, and
hypoglycemia from poor liver function.
o Mothers are at risk for cerebral hemorrhages, aspiration pneumonia, and hypoxic
encephalopathy
Fetal complications: growth restriction and preterm birth
Treatment/Management:
o FFP or platelets
o If hypoglycemic – glucose infusion
o Birth of baby as soon as feasible
o No epidural anesthesia due to clotting problem, bleeding at the site may occur
L. MULTIPLE PREGNANCY
Multiple gestation is considered a complication of pregnancy because a woman’s body
must adjust to the effects of more than one fetus.
occurs in 2% to 3% of all births
NUPC 110 Module II Page 39
Identical (monozygotic) twins begin with a single ovum and spermatozoon
Single-ovum twins usually have one placenta, one chorion, two amnions, and two
umbilical cords
o Always same sex
Two thirds of twins are fraternal(dizygotic, nonidentical), the result of the
fertilization of two separate ova by two separate spermatozoa (possibly not from the
same sexual partner)
Double-ova twins have two placentas, two chorions, two amnions, and two umbilical
cords
o The twins may be of the same or different sex
Assessment
o uterus begins to increase in size at a rate faster than usual
o Alpha-fetoprotein levels are elevated
o multiple sets of fetal heart sounds are heard
o ultrasound can reveal multiple gestation sacs early in pregnancy
o In some instances, early ultrasound examinations reveal multiple amniotic sacs
but then later in pregnancy, in as many as 30% of women, only one fetus
remains
o vanishing twin syndrome
Therapeutic Management
o susceptible to complications of pregnancy such as PIH, hydramnios, placenta
previa, preterm labor, and anemia than are women carrying one fetus
o more prone to postpartum bleeding because of the additional uterine stretching
that must occur
o 25% of low-birth-weight babies are from multiple pregnancies
o higher risk of congenital anomalies in twins, such as spinal cord defect, than
with single births
o higher incidence of velamentous cord insertion (the cord inserted into the
fetal membranes) with twins than with single births
o With monozygotic twins, the fetuses can share vascular communication, possibly
leading to overgrowth of one fetus and undergrowth of the second (a twin-to-
twin transfusion), resulting in discordant infants
o If a single amnion is present, there can be knotting and twisting of umbilical
cords, causing fetal distress or difficulty with birth
o Early and close observation of the pregnant woman
M. HYDRAMNIOS
Amniotic fluid is formed by a combination of the cells of the amniotic membrane and
from fetal urine
NUPC 110 Module II Page 40
amniotic fluid volume during pregnancy is 500 to 1000 mL at term
Occurs with hyperglycemia
Excess fluid more than 2000 mL or an amniotic fluid index above 24 cm is considered
hydramnios
can cause fetal malpresentation (transverse)
can lead to premature rupture of the membranes from the increased pressure with
possible prostaglandin release
Assessment:
o unusually rapid enlargement of the uterus
o Palpation of parts of the fetus and FHT auscultation is difficult
o extreme shortness of breath as the overly distended uterus pushes up against
her diaphragm
o may develop lower extremity varicosities and hemorrhoids because of poor
venous return from the extensive uterine pressure
o Increased weight gain
o UTZ to document presence of hydramnios
Management
o maintaining bed rest helps to increase uteroplacental circulation and reduces
pressure on the cervix, which may help prevent preterm labor
o report any sign of ruptured membranes or uterine contractions
o Assess VS and edema
o Amniocentesis daily to remove extra AF
o Avoid constipation
o High fiber diet
o Stool softeners if diet is not enough
o PROM and preterm birth may occur because of excessive pressure,
o After birth, the infant must be assessed carefully for factors that may have
interfered with the ability to swallow in utero
N. OLIGOHYDRAMNIOS
refers to a pregnancy with less than the average amount of amniotic fluid
usually caused by a bladder or renal disorder in the fetus that interferes with voiding
can occur from severe growth restriction
NUPC 110 Module II Page 41
Because the fetus is so cramped for space, muscles are left weak at birth, lungs fail to
develop (hypoplastic lungs), leading to severe difficulty breathing after birth, and
features of the face become distorted (termed Potter’s syndrome)
Assessment/ Management
o Slow growth of uterus
o Revealed by UTZ
o Amniotransfusion or instillation of fluid into the uterus by amniocentesis
procedure can help relieve this concern
o Infants need careful inspection at birth to rule out kidney disease and
compromised lung development.
O. POST TERM PREGNANCY
A pregnancy that exceeds 38-42 weeks is prolonged (post term pregnancy, postmature,
or postdate)
occurs in 3% to 12% of all pregnancies
Prolonged pregnancy can occur in a woman receiving a high dose of salicylates,
because it interferes with the synthesis of prostaglandins
also associated with myometrial quiescence, or a uterus that does not respond to
normal labor stimulation
Fetal complications:
o meconium aspiration
o Macrosomia and/or Lack of growth
o Decreased blood perfusion due to decreased placental function
o Lack of oxygen, fluid and nutrients supply to the fetus
o Oligohydramnios – variable decelerations
If labor has not begun by 41 weeks, a maternal vaginal fibronectin level, a nonstress
test, and/or a biophysical profile may be ordered to document the state of placental
perfusion and the amount of amniotic fluid present
If lab exams are normal – miscalculation of due date
If lab exams are abnormal – labor is induce by PG or misoprostol, oxytocin
CS if oxytocin is ineffective
NUPC 110 Module II Page 42
P. PSEUDOCYESIS
or false pregnancy, nausea and vomiting, amenorrhea, and enlargement of the
abdomen occur in either a nonpregnant woman or a man
several theories regarding why the phenomenon occurs:
wish-fulfillment theory suggests a woman’s desire to be pregnant actually causes
physiologic changes to occur;
conflict theory suggests a desire for and fear of pregnancy create an internal conflict
leading to physiologic changes;
and depression theory attributes the cause to major depression
(+) Breast and abdominal enlargement but UTZ reveals (-) pregnancy
Counseling of patient to help them better handle their needs
Q. ISOIMMUNIZATION (RH INCOMPATIBILITY)
occurs when an Rh-negative mother (one negative for a D antigen or one with a dd
genotype) carries a fetus with an Rhpositive blood type (DD or Dd genotype)
the father of the child must either be homozygous (DD) or heterozygous (Dd ) Rh-
positive
people who have Rh-positive blood have a protein factor (the D antigen) that Rh-
negative people do not have
After sensitization, mother forms antibodies against D antigen
Antibodies cross placenta and cause hemolysis of RBCs – hemolytic disease of the
newborn or erythroblastosis fetalis
amniocentesis or percutaneous umbilical blood sampling may cause fetal blood to
enter maternal circulation
Assessment/Management:
o All mothers with Rh negative blood should have anti-D antibody titer during first
prenatal visit
o If the results are normal or the titer is minimal (normal is 0; a ratio below 1:8
is minimal), the test will be repeated at week 28 of pregnancy, if this is also
normal, no therapy is needed
o If a woman’s anti-D antibody titer is elevated at a first assessment (1:16 or
greater), the well-being of the fetus in this potentially toxic environment will
be monitored every 2 weeks (or more often) by Doppler velocity of the fetal
middle cerebral artery, a technique that can predict when anemia is present
or fetal red cells are being destroyed
o If the artery velocity remains high, a fetus is not developing anemia and most
likely is an Rh-negative fetus
o If the reading is low, it means a fetus is in danger
o Rh (D) immune globulin (RhIG), a commercial preparation of passive Rh (D)
antibodies against the Rh factor, is administered to women who are Rh-negative
at 28 weeks of pregnancy
o RhIG cannot cross placenta
o RhIG is injected to a mother with Rh positive baby within 72 hours to prevent
formation of normal antibodies
o RhIG is a passive antibody protection and is destroyed in 2 weeks to 2 months
o Coomb’s Test
Direct – detects antibodies that are stucked in the RBC surface
Indirect – detects antibodies that are floating freely in blood
o Intrauterine Transfusion
done by injecting red blood cells, by amniocentesis technique, directly
into a vessel in the fetal cord or depositing them in the fetal abdomen
where they migrate into the fetal circulation
75 to 150 mL of washed red cells are used, depending on fetal age
Mother to rest for 30 mins with fetal and uterine activity monitoring
NUPC 110 Module II Page 43
Transfusion is sometimes done only once during pregnancy, or it may be
repeated as often as every 2 weeks
Risks (Transfusion):
cord blood vessel could be lacerated by the needle
uterus may be so irritated that labor contractions begin
o After Birth
exchange transfusion to remove hemolyzed red blood cells and replace
them with healthy blood cells
R. FETAL DEATH
most severe complications of pregnancy
most likely causes include chromosomal abnormalities, congenital malformations,
infections such as hepatitis B, immunologic causes, and complications of maternal
disease
KEY POINTS
● Vaginal bleeding during pregnancy is always serious until ruled otherwise because it has the
potential to diminish the blood supply of both the mother and fetus.
● The amount of bleeding which is evident may not be truly indicative of the amount of
bleeding occurring as hidden, internal bleeding may also be happening. As a rule, women with
bleeding during pregnancy should be positioned on their side to improve placental circulation.
● Spontaneous miscarriage is the loss of a pregnancy before viability of the fetus (20 to 24
weeks). The majority of these early pregnancy losses are attributed to chromosomal
abnormalities. Miscarriages are classified as threatened, imminent, complete, incomplete,
missed, or recurrent pregnancy loss. Women who have a spontaneous miscarriage at home
should bring any tissue passed to the hospital for an analysis for gestational trophoblastic
disease.
● Ectopic pregnancy is pregnancy implantation outside the uterus, usually in a fallopian tube.
If discovered before the tube ruptures, methotrexate or mifepristone can be administered to
cause the conceptus to be reabsorbed. If not discovered early, sharp lower quadrant pain
occurs at about 6 to 12 weeks as the tube ruptures. Surgery is done to remove the conceptus
and repair the tube to halt bleeding.
● Gestational trophoblastic disease is abnormal overgrowth of trophoblast cells. If not
discovered by an ultrasound early in pregnancy, bleeding and expulsion of the abnormal
growth occur at about the 16th week of pregnancy. Women need close follow-up after this
because it can lead to choriocarcinoma, a malignancy.
● Premature cervical dilatation occurs when the cervix dilates early in pregnancy, before
viability of the fetus. Sutures (cervical cerclage) can be placed to prevent the cervix from
dilating prematurely this way again in a second pregnancy.
● Placenta previa is low implantation of the placenta so that it crosses the cervical os. If this is
not discovered before labor, cervical dilatation may cause the placenta to tear, causing severe
blood loss. Women who have symptoms of placenta previa (painless vaginal bleeding in the
third trimester) should not have vaginal examinations done to prevent disruption of the low-
implanted placenta.
● Premature separation of the placenta (abruptio placentae), placental separation from the
uterus before the fetus is born, usually occurs late in pregnancy. This separation immediately
cuts off blood supply to the fetus. Women with increased parity, those with previous uterine
surgery, and those who use cocaine are at highest risk for this. Often it is manifested by
sudden, sharp fundal pain, then a continuing dull pain and vaginal bleeding.
● Disseminated intravascular coagulation is a blood disorder that may occur with any trauma,
so it can accompany such conditions as premature separation of the placenta and pregnancy-
induced hypertension. Blood coagulation is so extreme at one point in the circulatory system
that clotting factors are used up, resulting in their absence in the remainder of the system.
NUPC 110 Module II Page 44
Beginning symptoms of this include easy bruising, petechiae, and oozing from intravenous
sites. Heparin is used to stop the local coagulation and free up clotting factors for systemic use
. ● Preterm labor is labor that occurs after 20 weeks and before the end of the 37th week of
pregnancy. A woman is said to be in preterm labor when she has had uterine contractions
every 10 minutes for 1 hour and cervical dilatation begins. Common tocolytics, drugs that can
halt labor, are betasympathomimetic agents such as terbutaline (Brethine).
● Preterm rupture of the membranes is tearing of the fetal membranes with loss of amniotic
fluid before the pregnancy is at term. After rupture, there is a high risk of fetal and uterine
infection (chorioamnionitis) and preterm birth.
● Pregnancy-induced hypertension is a unique disorder that occurs with pregnancy with three
classic symptoms: hypertension, edema, and proteinuria. It is categorized as pre-eclampsia or
eclampsia. If mild (blood pressure not over 140/90), treatment is bed rest and perhaps low-
dose aspirin. If severe (blood pressure over 160/110), bed rest plus administration of
magnesium sulfate is necessary. If a seizure occurs, the condition becomes eclampsia. Helping
prevent the disease from progressing to this stage is an important nursing responsibility.
MODULE SUMMARY
This module presented three lessons. Lesson 1 defined what a high risk pregnancy is and
included identification of such cases. Lesson 2 tackled sudden pregnancy complications or those
problems that may arise during pregnancy. Lesson 3 discussed problems that may arise during
labor and delivery. Management of such problems were also discoursed.
SUMMATIVE TEST
I. True or False
TRUE 1. Abortion usually happens during the second trimester of pregnancy.
FALSE 2.Gestational Hypertension may happen to any woman, even in nonpregnant
women.
TRUE 3. Slight bleeding during the first trimester of pregnancy is normal.
TRUE 4. Macrosomia may cause dystocia.
TRUE 5. Identifying high risk pregnancy is a crucial part in the pre-pregnancy phase.
TRUE 6. Abnormal presentation may complicate birth.
FALSE 7. In missed abortion, fetus is still alive with weak heart rate.
NUPC 110 Module II Page 45
TRUE 8. Abruptio placenta is the early separation of the placenta.
FALSE 9. In Isoimmunization, a Rhesus positive mother may cause reaction to a Rhesus
negative fetus.
FALSE 10. Oxytocic drugs should be administered in case of inverted uterus to replace it in
normal position.
II. Multiple Choice
1. Women who have had a complication of pregnancy have the potential to develop
depression in the postpartal period because their pregnancy did not go the way they
wanted or imagined. To see what factors tend to be associated with depression in women
who develop gestational diabetes, researchers administered a questionnaire to 71 women
at 4 to 15 weeks postpartum. Results of the study showed that 34% of the women who
developed gestational diabetes showed depressive symptoms; factors most associated with
depression were cesarean birth and more weight gain than expected during pregnancy
(Nicklas, Miller, Zera, et al., 2013). Based on the previous study, which statement by
Angelina would worry the nurse most that she might develop postpartum depression?
a. “I want to shed some pounds so I’ll fit into the new dress I bought for New Year’s Eve.”
b. “I hated giving insulin to myself; I’m relieved to not be doing that anymore.”
c. “My baby is bigger than I expected, but his eyes are beautiful and he’s cute.”
d. “I think my husband adjusted better to my having diabetes than I did.”
2. Angelina is prescribed an insulin pump to administer insulin for her gestational diabetes.
What patient education would the nurse want to provide to explain why nighttime is a
particularly hazardous time for her fetus during pump therapy?
a. The fetus can develop hyperglycemia from excessive insulin administration.
b. Continuous insulin administration with no food intake can lead to hypoglycemia.
c. Her lack of exercise at night tends to lead to hypercalcemia from muscle disuse.
d. Her lack of fluid intake during the night causes a relative increase in serum insulin
levels.
3. Rosann’s baby is not only large but also in an occipitoposterior position. The nurse would
want the team members to know which position is best for a woman whose baby is in the
occipitoposterior position during labor?
a. On her right side to stretch the pelvic inlet
b. Walking about to encourage fetal descent
c. Sitting in a rocking chair to aid presentation
d. On her hands and knees to help fetal rotation
4. Women over the age of 40 years are at increased risk for developing gestational
hypertension. As a result, routine screenings for this health problem have been emphasized
on the maternal unit for older mothers. What is the rationale for this change in nursing
practice?
a. Many women over 40 years are underweight before they begin pregnancy.
b. Older women tend to have a higher fluid intake than do younger women.
c. Many older women are prone to edema due to their lower activity levels.
d. The blood vessels of older women may not be as elastic as those of younger women.
5. Mindy makes friends with another adolescent at the prenatal clinic: a 19-year-old who has
a cognitive deficit. When planning care for this patient, what would be the best way to
meet this woman’s educational needs?
a. Provide simple, written materials rather than providing verbal instructions.
b. Provide education to the woman’s partner or another person with full cognitive
function.
c. Ensure that teaching is appropriate to the woman’s level of cognition
d. Enlist the help of a social worker when teaching the woman.
NUPC 110 Module II Page 46
CONGRATULATIONS! YOU COMPLETED MODULE II!
NUPC 110 Module II Page 47
You might also like
- Costa Leona Series 1 Scorching LoveDocument27 pagesCosta Leona Series 1 Scorching LoveHakdog Shermolang67% (3)
- A Community Diagnosis in Level III Group 2Document89 pagesA Community Diagnosis in Level III Group 2Jenny Agustin FabrosNo ratings yet
- Science Grade 3 Activity SheetDocument9 pagesScience Grade 3 Activity SheetEllanie Pujalte MontebonNo ratings yet
- Selenereese - RUTHLESS MEN SERIES 1 Hellions Possession 1Document198 pagesSelenereese - RUTHLESS MEN SERIES 1 Hellions Possession 1Hakdog Shermolang100% (2)
- Topic 2 ExercisesDocument6 pagesTopic 2 ExercisesRaniel Pamatmat0% (1)
- Prelim Reviewer 2023Document83 pagesPrelim Reviewer 2023jakexsanchez1515No ratings yet
- Finals Exam Ncm209Document91 pagesFinals Exam Ncm209Shang MarianoNo ratings yet
- Prelim Outline - Bioethics BSNDocument11 pagesPrelim Outline - Bioethics BSNSheenaNo ratings yet
- Ncma219 Lec MidtermDocument51 pagesNcma219 Lec MidtermMacababbad Joshua MiguelNo ratings yet
- BIOETHICS ABCDE Compilation WK 2 6Document268 pagesBIOETHICS ABCDE Compilation WK 2 6Sexbomb Adela KirstenNo ratings yet
- Group 2 - Technology As A Way of RevealingDocument50 pagesGroup 2 - Technology As A Way of Revealinggenar greg tubogNo ratings yet
- NCM 108 Bioethics Finals 1Document10 pagesNCM 108 Bioethics Finals 1Martina MedranoNo ratings yet
- Minutes) Everybody WritesDocument15 pagesMinutes) Everybody WritesRanes AndyNo ratings yet
- Quality of Prenatal Care Questionnaire: Instrument Development and TestingDocument17 pagesQuality of Prenatal Care Questionnaire: Instrument Development and TestingGreat CoassNo ratings yet
- Ra 7600Document5 pagesRa 7600WeGovern InstituteNo ratings yet
- Psych-Midterm ReviewerDocument12 pagesPsych-Midterm ReviewerPia Rose RoqueNo ratings yet
- Ethics ConsequentialismDocument19 pagesEthics ConsequentialismJibfrho SagarioNo ratings yet
- NCM209Document94 pagesNCM209Gummy BearsNo ratings yet
- Ncam219 Lec PDFDocument102 pagesNcam219 Lec PDFDAVE BARIBENo ratings yet
- Older AdultsDocument10 pagesOlder AdultsMia Grace GarciaNo ratings yet
- Module 11, Chapter 27:: University of Cebu-BaniladDocument10 pagesModule 11, Chapter 27:: University of Cebu-BaniladSuzanne Kyla CabuenasNo ratings yet
- CHN Reviewer IDocument21 pagesCHN Reviewer IApple Mae AuxteroNo ratings yet
- NCM 112 Prefinal LectureDocument10 pagesNCM 112 Prefinal LectureFatima-Ridziana AbdurahmanNo ratings yet
- MCN Lec MidtermDocument29 pagesMCN Lec Midtermnaomie manaliliNo ratings yet
- Marquez - Case Study 114Document6 pagesMarquez - Case Study 114Caren MarquezNo ratings yet
- The Voluntary and Nonvoluntary Acts of ManDocument2 pagesThe Voluntary and Nonvoluntary Acts of ManJohn Michael SorianoNo ratings yet
- NCM 207 Lecture 1 PDFDocument127 pagesNCM 207 Lecture 1 PDFkrizza abellanosaNo ratings yet
- CONSEQUENTIALISMDocument26 pagesCONSEQUENTIALISMAngelica TañedoNo ratings yet
- Rle Module Rle Unit Week: Bachelor of Science in Nursing: Rle NCM 105 - Psychiatric NursingDocument4 pagesRle Module Rle Unit Week: Bachelor of Science in Nursing: Rle NCM 105 - Psychiatric NursingGabriel VillegasNo ratings yet
- OB GYN CasePre FinalDocument82 pagesOB GYN CasePre FinalMarjorie Lahaylahay AlabataNo ratings yet
- NCM 112 Lec NotesDocument10 pagesNCM 112 Lec NotesCamille GuintoNo ratings yet
- Hes 005 Session 16 SasDocument7 pagesHes 005 Session 16 SasJose Melmar Autida AutenticoNo ratings yet
- Kidney Disease and PregnancyDocument11 pagesKidney Disease and PregnancyAndreaNo ratings yet
- Pharma Notes MidsDocument17 pagesPharma Notes MidsMa. Rita Concepcion TungulNo ratings yet
- Congenital Hydrocephalus: Case PresentationDocument35 pagesCongenital Hydrocephalus: Case PresentationIan Mizzel A. DulfinaNo ratings yet
- DS (Ibuprofen)Document6 pagesDS (Ibuprofen)Mary April MendezNo ratings yet
- Chapter 12: Nursing Care To Promote Fetal and Maternal HealthDocument9 pagesChapter 12: Nursing Care To Promote Fetal and Maternal HealthAlyssaGrandeMontimorNo ratings yet
- Week 1 RUBRICS Wound Care and DressingDocument2 pagesWeek 1 RUBRICS Wound Care and DressingPaola CruzNo ratings yet
- NCM 109 FinalsDocument68 pagesNCM 109 FinalsJHOANA MARIE LOONo ratings yet
- Module 7 Student Activity SheetDocument7 pagesModule 7 Student Activity SheetJenny Agustin FabrosNo ratings yet
- Ncm105 Nutrition ReviewerDocument24 pagesNcm105 Nutrition ReviewerJeon CookyNo ratings yet
- OB - Postterm PregnancyDocument6 pagesOB - Postterm PregnancyDarren Mae MosadaNo ratings yet
- CHN ReviewerDocument8 pagesCHN Revieweralyssaaaaa1234885No ratings yet
- Aparicio Ryan Shane Y. Toddler AssessmentDocument24 pagesAparicio Ryan Shane Y. Toddler AssessmentThea DuoNo ratings yet
- Rle Activity 107 MMDSTDocument12 pagesRle Activity 107 MMDSTMaxene Reyes ValdezNo ratings yet
- Funda RLEDocument29 pagesFunda RLECharisse CaydanNo ratings yet
- Appearance of A NewbornDocument33 pagesAppearance of A NewbornGeguirra, Michiko SarahNo ratings yet
- Case Study NCM 109 ApacibleDocument9 pagesCase Study NCM 109 ApacibleJade CentinoNo ratings yet
- Ncma217 Lec MidtermDocument21 pagesNcma217 Lec Midtermcaitie miracleNo ratings yet
- Neutralizes The Acidity of The UrethraDocument12 pagesNeutralizes The Acidity of The Urethracresia hidalgoNo ratings yet
- UntitledDocument6 pagesUntitledDada Tin GoTanNo ratings yet
- Rle FinalsDocument9 pagesRle FinalsMary Florence VelardeNo ratings yet
- Nursing Care of The Developing FetusDocument52 pagesNursing Care of The Developing FetusKyrriel CNo ratings yet
- CHN211 Week 8 WORD - Integrated Management of Childhood IllnessDocument28 pagesCHN211 Week 8 WORD - Integrated Management of Childhood IllnessYrah Elaine SanchezNo ratings yet
- ImmunizationDocument4 pagesImmunizationAshley ValdezNo ratings yet
- Book Onco ConceptDocument42 pagesBook Onco ConceptJulia Rae Delos SantosNo ratings yet
- Rhu d1 Compiled December LatestDocument169 pagesRhu d1 Compiled December LatestDilausan B MolukNo ratings yet
- Martha Rogers, Dorothea Orem, Imogene KingDocument9 pagesMartha Rogers, Dorothea Orem, Imogene KingCASTRO, ANDREI KARL Z.No ratings yet
- NCM 107 RLE 1F - Labor and DeliveryDocument68 pagesNCM 107 RLE 1F - Labor and DeliveryNotur BarbielatNo ratings yet
- Case PresDocument100 pagesCase PresJoj BagnateNo ratings yet
- RABE 1 CHN 2semDocument6 pagesRABE 1 CHN 2semBasa, Rica Mae P.No ratings yet
- Transes MCN Laboratory Week 1Document17 pagesTranses MCN Laboratory Week 1Akira Pineda100% (1)
- Sas 11 LectureDocument3 pagesSas 11 LectureFretchel Grace Silverado MesaNo ratings yet
- Muscle LabDocument7 pagesMuscle LabHakdog ShermolangNo ratings yet
- Bed Making: Occupied Bed Unoccupied BedDocument16 pagesBed Making: Occupied Bed Unoccupied BedHakdog ShermolangNo ratings yet
- C C C V C C C V C C C V C C C C C V C C C V C C C V C C C V C C C V C C C VDocument1 pageC C C V C C C V C C C V C C C C C V C C C V C C C V C C C V C C C V C C C VHakdog ShermolangNo ratings yet
- Biofuel Ft. KantutayDocument21 pagesBiofuel Ft. KantutayHakdog Shermolang100% (1)
- Heat Transfer Class Project: Powerpoint Presentation File Name It: Project2014-# in Class Roll-#In Class RollDocument3 pagesHeat Transfer Class Project: Powerpoint Presentation File Name It: Project2014-# in Class Roll-#In Class RollSwapnil BhattacharyaNo ratings yet
- SULIT 4551/3 Biologi Kertas 3 Sept 2007 SeptemberDocument13 pagesSULIT 4551/3 Biologi Kertas 3 Sept 2007 SeptemberhasimahazitNo ratings yet
- A Hybrid Cutting Force Model For High-Speed Milling of Titanium AlloysDocument4 pagesA Hybrid Cutting Force Model For High-Speed Milling of Titanium Alloysabdsu75No ratings yet
- 1Document10 pages1Shashank PathakNo ratings yet
- Transient Results and Response Spectra: Sofistik 2020Document25 pagesTransient Results and Response Spectra: Sofistik 2020Chris LumyNo ratings yet
- Rooms DivisionDocument19 pagesRooms Divisionনিয়াজ মাহমুদNo ratings yet
- Hawthorne ExperimentsDocument7 pagesHawthorne ExperimentsAbhishek MishraNo ratings yet
- KERENDIA Doctor Discussion Guide - FINALDocument2 pagesKERENDIA Doctor Discussion Guide - FINALajaygajaNo ratings yet
- Performance Assesment-A Shift From Intangibles To TangiblesDocument25 pagesPerformance Assesment-A Shift From Intangibles To Tangibles2005ravi100% (1)
- Describe The Appearance and Uses Uniform and Non-Uniform Mixtures (S6MT-Ia-c-1)Document4 pagesDescribe The Appearance and Uses Uniform and Non-Uniform Mixtures (S6MT-Ia-c-1)Nerissa de LeonNo ratings yet
- Discourse Analysis of Lilith PDFDocument30 pagesDiscourse Analysis of Lilith PDFJorge BelinskyNo ratings yet
- Women EntrepreneursDocument19 pagesWomen Entrepreneursmohit_roy_8No ratings yet
- A Guide To Transformer Maintenance by S D Myers J J Kelly R H Parrish 0939320002Document5 pagesA Guide To Transformer Maintenance by S D Myers J J Kelly R H Parrish 0939320002N4Y CHANNELNo ratings yet
- Callista Roy The Adaptation Model of NursingDocument8 pagesCallista Roy The Adaptation Model of Nursingapi-640980201No ratings yet
- AWNMag6 02Document57 pagesAWNMag6 02Michał MrózNo ratings yet
- English Answer Sheet First Quarter Module 2Document6 pagesEnglish Answer Sheet First Quarter Module 2Jakecob Mejillano JacobNo ratings yet
- 이휘소 논문 PDFDocument4 pages이휘소 논문 PDFjemin12798No ratings yet
- Trigonometry Exam QuestionsDocument9 pagesTrigonometry Exam Questionsnsprior1659No ratings yet
- Dada Vaswani SpeechDocument15 pagesDada Vaswani SpeechTheresa WestNo ratings yet
- A Comparative Study On Fundamental and Technical AnalysisDocument34 pagesA Comparative Study On Fundamental and Technical AnalysisTarun Chawla0% (1)
- York County Court Schedule For May 4, 2015Document10 pagesYork County Court Schedule For May 4, 2015York Daily Record/Sunday NewsNo ratings yet
- 01 Reading PTEDocument5 pages01 Reading PTEUsha ShresthaNo ratings yet
- Romeo and Juliet 2023 WorkbookDocument62 pagesRomeo and Juliet 2023 WorkbooklstewardNo ratings yet
- P12y en T C74Document572 pagesP12y en T C74spakumaranNo ratings yet
- FRC Essays - Comply or ExplainDocument64 pagesFRC Essays - Comply or ExplainRahat TabassumNo ratings yet
- Manual For Audi A3Document2 pagesManual For Audi A3Anonymous mXONwr1c4No ratings yet
- Stresses in Soil 161208Document67 pagesStresses in Soil 161208Tuan Jalai100% (1)
- Aging Management Program Effectiveness: NEI 14-12 (Revision 0)Document16 pagesAging Management Program Effectiveness: NEI 14-12 (Revision 0)naveedNo ratings yet