
Brain Immune Interactions
Brain Immune Interactions
You might also like
- 【机制】IL-12 and IL-23 Pathway Inhibition in Inflammatory Bowel DiseaseDocument14 pages【机制】IL-12 and IL-23 Pathway Inhibition in Inflammatory Bowel Diseasejona renNo ratings yet
- The Nuctemeron of Apollonius of TyanaDocument9 pagesThe Nuctemeron of Apollonius of Tyanacc vereNo ratings yet
- A Critical Appraisal of Amyloid-β-targeting Therapies for Alzheimer Disease 2019 ReviewDocument16 pagesA Critical Appraisal of Amyloid-β-targeting Therapies for Alzheimer Disease 2019 Review畏No ratings yet
- Immunity To MicrobesDocument25 pagesImmunity To MicrobestimcarasNo ratings yet
- Microbes and the Mind: The Impact of the Microbiome on Mental HealthFrom EverandMicrobes and the Mind: The Impact of the Microbiome on Mental HealthNo ratings yet
- Case 1 EndocrineDocument5 pagesCase 1 EndocrineRegine Mae EncinadaNo ratings yet
- Hypersensitivity 1 4Document62 pagesHypersensitivity 1 4Wahyudi YusmanNo ratings yet
- Innate ImmunityDocument14 pagesInnate Immunitydexter603No ratings yet
- Biomedicines 11 00115 v2Document22 pagesBiomedicines 11 00115 v2Wesley M.SantosNo ratings yet
- Jurnal AutismDocument10 pagesJurnal AutismAby SuryaNo ratings yet
- HypersensitivityDocument52 pagesHypersensitivityFuzti Fauzia100% (1)
- Artigo1 Galecki 2018Document23 pagesArtigo1 Galecki 2018Anuska ErikaNo ratings yet
- Modulo1 - FArtigo - Atores de Risco No Autismo - Pensando Fora Do CérebroDocument14 pagesModulo1 - FArtigo - Atores de Risco No Autismo - Pensando Fora Do CérebroViviane MartinsNo ratings yet
- Jurnal AutismeDocument11 pagesJurnal AutismeKabhithra ThiayagarajanNo ratings yet
- Andropause: Current Concepts: Keywords: Androgen Deficiency in Ageing Male, Late Onset Hypogonadism, TestosteroneDocument14 pagesAndropause: Current Concepts: Keywords: Androgen Deficiency in Ageing Male, Late Onset Hypogonadism, TestosteroneYariCárdenasNo ratings yet
- Autismo y AutoinmunidadDocument50 pagesAutismo y AutoinmunidadPsicoterapia InfantilNo ratings yet
- Membrane and Protein TraffickingDocument135 pagesMembrane and Protein TraffickingsujanupamNo ratings yet
- The Genetics of Autism 2004Document2 pagesThe Genetics of Autism 2004emma199No ratings yet
- Cytokines & Their ActionsDocument59 pagesCytokines & Their ActionsSharanabasappa DurgNo ratings yet
- Ciprofloxacin Induced Chondrotoxicity and Tendinopathy PDFDocument7 pagesCiprofloxacin Induced Chondrotoxicity and Tendinopathy PDFAvelox FloxNo ratings yet
- Genetics ArchitectureDocument9 pagesGenetics ArchitectureFatimah Dina AlkaffNo ratings yet
- Specific Immunity. FINALDocument29 pagesSpecific Immunity. FINALLUZVIMINDA GORDONo ratings yet
- Human Zinc DefDocument6 pagesHuman Zinc DefMiodrag MilicNo ratings yet
- The Female Protective Effect in Autism SDocument10 pagesThe Female Protective Effect in Autism SNps Caren RodriguezNo ratings yet
- Multiple Sclerosis Bench To Bed - Alexzander A.A. Asea, Fabiana G PDFDocument189 pagesMultiple Sclerosis Bench To Bed - Alexzander A.A. Asea, Fabiana G PDFHîrjoabă IoanNo ratings yet
- Immunobiology of Gestational Zinc Deficiency: Nele WellinghausenDocument6 pagesImmunobiology of Gestational Zinc Deficiency: Nele WellinghausenAnonymous dXdCD7D9UNo ratings yet
- Epigenetic SDocument19 pagesEpigenetic SNoor SabahNo ratings yet
- Articles On Wheat ToxicityDocument96 pagesArticles On Wheat ToxicityDr. Heath MotleyNo ratings yet
- Spikevax Previously Covid 19 Vaccine Moderna Epar Public Assessment Report - enDocument169 pagesSpikevax Previously Covid 19 Vaccine Moderna Epar Public Assessment Report - enBlessworkNo ratings yet
- The Implications of Vitamin D Status During Pregnancy On Mother and Her Developing ChildDocument11 pagesThe Implications of Vitamin D Status During Pregnancy On Mother and Her Developing ChildindahNo ratings yet
- The Role of Copper As A Modifier of Lipid Metabolism: January 2013Document23 pagesThe Role of Copper As A Modifier of Lipid Metabolism: January 2013Leni LismayantiNo ratings yet
- Processed Foods and Their Nutrition: Salim-ur-Rehman, Kanza Aziz Awan and Tahir ZahoorDocument29 pagesProcessed Foods and Their Nutrition: Salim-ur-Rehman, Kanza Aziz Awan and Tahir ZahoorM SNo ratings yet
- Brain-Heart InteractionsDocument22 pagesBrain-Heart Interactionscc vereNo ratings yet
- Principle of VaccineDocument10 pagesPrinciple of VaccineRasyid WicaksonoNo ratings yet
- The Immune Response in Autism - A New Frontier For Autism ResearchDocument15 pagesThe Immune Response in Autism - A New Frontier For Autism ResearchJorge AlvesNo ratings yet
- Immunology PDFDocument1 pageImmunology PDFTanushree PalNo ratings yet
- Tau Opa ThiesDocument22 pagesTau Opa ThiesIrina OdajiuNo ratings yet
- Difference Between Mast Cell and BasophilDocument3 pagesDifference Between Mast Cell and Basophilponbohacop100% (1)
- Matabolic PathwaysDocument11 pagesMatabolic PathwaysLevi100% (2)
- Research Paper Vaccines AutismDocument5 pagesResearch Paper Vaccines Autismc9rvz6mm100% (1)
- Biomol Tranduksi Sinyal Presentasi Kelompok Komunikasi Sel-1Document42 pagesBiomol Tranduksi Sinyal Presentasi Kelompok Komunikasi Sel-1ratnaekawatiNo ratings yet
- Ospolot 200 MG, Film-Coated Tablets: Summary of Product Characteristics (SPC)Document7 pagesOspolot 200 MG, Film-Coated Tablets: Summary of Product Characteristics (SPC)ddandan_2No ratings yet
- Liver Enzymes - ALT/ALT: DR - SarojaDocument15 pagesLiver Enzymes - ALT/ALT: DR - SarojaSaroja VeereshNo ratings yet
- Neuronal Signaling: July 2015Document12 pagesNeuronal Signaling: July 2015bening swarajiwaNo ratings yet
- A Systematic Review of Iodine Deficiency Among Women in The UKDocument10 pagesA Systematic Review of Iodine Deficiency Among Women in The UKanass.rami0676959544No ratings yet
- Approach To FatigueDocument27 pagesApproach To FatigueBasil Hussam100% (1)
- The Effects of Iodine Deficiency in Pregnancy and InfancyDocument10 pagesThe Effects of Iodine Deficiency in Pregnancy and InfancyerlyNo ratings yet
- Start Low and Go Slow 1-21-2014Document5 pagesStart Low and Go Slow 1-21-2014Ed JonesNo ratings yet
- Autism Spectrum Disorder Symptoms Improve With Combination Therapy Directed at Improving Gut Microbiota and Reducing InflammationDocument7 pagesAutism Spectrum Disorder Symptoms Improve With Combination Therapy Directed at Improving Gut Microbiota and Reducing InflammationSarah Naomi Jeanett ObenhoferNo ratings yet
- Xenobiotic MetabolismDocument64 pagesXenobiotic MetabolismBelajar dan berdoaNo ratings yet
- Thyroid Autoimmune DiseasesDocument21 pagesThyroid Autoimmune Diseasesmicheal1960No ratings yet
- 5-Alpha-Reductase Inhibitor PDFDocument8 pages5-Alpha-Reductase Inhibitor PDFP. GuadamuzNo ratings yet
- Biochemistry of Adaptive ImmunityDocument22 pagesBiochemistry of Adaptive Immunityshreyansh singhNo ratings yet
- 2021-Reviews in Basic and Clinical Gastroenterology and HepatologyDocument16 pages2021-Reviews in Basic and Clinical Gastroenterology and HepatologyÉden SiqueiraNo ratings yet
- @PIDs Curs 200903Document43 pages@PIDs Curs 200903Mohammad_Islam87No ratings yet
- Immunodeficiency: Faculty of Applied Science Department of Medical Lab. Ml3A, ML3C, ML3DDocument35 pagesImmunodeficiency: Faculty of Applied Science Department of Medical Lab. Ml3A, ML3C, ML3Dالدنيا ساعة فاجعلها طاعةNo ratings yet
- Matrix Metalloproteinases: The Most Important Pathway Involved With Periodontal DestructionDocument9 pagesMatrix Metalloproteinases: The Most Important Pathway Involved With Periodontal DestructionmochamadfadilNo ratings yet
- ClostridumDocument30 pagesClostridumFrancesca VargasNo ratings yet
- Metabolism of Vitamin DDocument36 pagesMetabolism of Vitamin DNisachon DenpraphaNo ratings yet
- Neuroendocrine Regulationof ImmunityDocument41 pagesNeuroendocrine Regulationof ImmunitynepretipNo ratings yet
- Immune Regulation by GlucocorticoidsDocument35 pagesImmune Regulation by GlucocorticoidsSyifa SariNo ratings yet
- Fimmu 10 01744Document20 pagesFimmu 10 01744Suryadi LimardiNo ratings yet
- VAShiva SystemsHealth Reading Vinod CurrentStatusofAdaptogensDocument11 pagesVAShiva SystemsHealth Reading Vinod CurrentStatusofAdaptogenscc vereNo ratings yet
- Autonomic Immune Vascular InteractionDocument9 pagesAutonomic Immune Vascular Interactioncc vereNo ratings yet
- Z. J. Lipowski (Auth.), P. Pichot, P. Berner, R. Wolf, K. Thau (Eds.) - Biological Psychiatry, Higher Nervous Activity-Springer US (1985)Document928 pagesZ. J. Lipowski (Auth.), P. Pichot, P. Berner, R. Wolf, K. Thau (Eds.) - Biological Psychiatry, Higher Nervous Activity-Springer US (1985)cc vereNo ratings yet
- Ox InflammationDocument15 pagesOx Inflammationcc vereNo ratings yet
- Oxytocin and VasopressinDocument19 pagesOxytocin and Vasopressincc vereNo ratings yet
- Wake Sleep CycleDocument11 pagesWake Sleep Cyclecc vereNo ratings yet
- Principles of Allostasis Optimal DesignDocument36 pagesPrinciples of Allostasis Optimal Designcc vereNo ratings yet
- Heart-Brain AxisDocument15 pagesHeart-Brain Axiscc vereNo ratings yet
- Brain-Heart InteractionsDocument22 pagesBrain-Heart Interactionscc vereNo ratings yet
- Stress Final Text 2016Document11 pagesStress Final Text 2016cc vereNo ratings yet
- Sensory Hepatic NervesDocument9 pagesSensory Hepatic Nervescc vereNo ratings yet
- Wa0041Document161 pagesWa0041SULDAANUL CAASHIQIINNo ratings yet
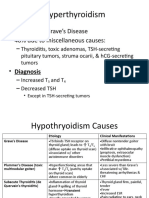
- Hyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesDocument6 pagesHyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesLeitavia D.No ratings yet
- Biology: Topic - Endocrine System Class-VIII Board - ICSEDocument3 pagesBiology: Topic - Endocrine System Class-VIII Board - ICSEItu DeyNo ratings yet
- Thyroid Gland Clinical Chemistry 2 (Laboratory) : LessonDocument4 pagesThyroid Gland Clinical Chemistry 2 (Laboratory) : LessonCherry Ann ColechaNo ratings yet
- Human Physiology Chapter 4 - EndDocument172 pagesHuman Physiology Chapter 4 - EndEmebet DebissaNo ratings yet
- Andrea Nakayama Hashimotos Institute 9-15-2014Document35 pagesAndrea Nakayama Hashimotos Institute 9-15-2014Vivek GuptaNo ratings yet
- DetailedapproaDocument65 pagesDetailedapproaMuhammed BarznjiNo ratings yet
- NCM 105 Nutrition and Diet LecDocument8 pagesNCM 105 Nutrition and Diet LecBi B BelleNo ratings yet
- 4 Lab ManualDocument160 pages4 Lab ManualAziz EzoNo ratings yet
- TIRMODDocument66 pagesTIRMODYaniNo ratings yet
- Final: LPL - Suvprabhat Pathology Lab Near Hospitsl Chowk (In Front of Zonal Hospital), Janakpur NepalDocument2 pagesFinal: LPL - Suvprabhat Pathology Lab Near Hospitsl Chowk (In Front of Zonal Hospital), Janakpur NepalAjay SharmaNo ratings yet
- Anatomy & Physiology of Thyroid GlandDocument5 pagesAnatomy & Physiology of Thyroid GlandJohnpaul DelapenaNo ratings yet
- Complications of MarasmusDocument3 pagesComplications of MarasmusNathania LongkutoyNo ratings yet
- Chapter 9 - Endocrine SystemDocument9 pagesChapter 9 - Endocrine SystemrishellemaepilonesNo ratings yet
- Thyroid DisordersDocument67 pagesThyroid DisordersMA 09No ratings yet
- Endocrine GlandsDocument14 pagesEndocrine GlandsVarsha Rai100% (1)
- Levothyroxine Interactions With Food and Dietary Supplements-A Systematic ReviewDocument20 pagesLevothyroxine Interactions With Food and Dietary Supplements-A Systematic Reviewalan_pedraza864No ratings yet
- Bio E1 Chapter 2 PDFDocument26 pagesBio E1 Chapter 2 PDFToto lstNo ratings yet
- Protocols For High-Risk Pregnancies - 2010 - Queenan - Appendix B Laboratory Values in Normal PregnancyDocument9 pagesProtocols For High-Risk Pregnancies - 2010 - Queenan - Appendix B Laboratory Values in Normal PregnancyHenry VillarosaNo ratings yet
- Tura KuDocument104 pagesTura KuFitzgerald BillyNo ratings yet
- Free Face Yoga Method Ebook Fumiko TakatsuDocument70 pagesFree Face Yoga Method Ebook Fumiko Takatsumagdalena0% (3)
- Total T3: For Use On The IMMULITE and Immulite 1000 SystemsDocument31 pagesTotal T3: For Use On The IMMULITE and Immulite 1000 SystemsEdgar Galván0% (1)
- Review of Hyperthyroidism As Per Ayurveda: Sirjana ShresthaDocument6 pagesReview of Hyperthyroidism As Per Ayurveda: Sirjana ShresthaSatyam SinghNo ratings yet
- Intro To EthologyDocument3 pagesIntro To EthologyRowzFerlTanutanNo ratings yet
- 5-Vitamin and MineralsDocument61 pages5-Vitamin and MineralsAnonymous 8hcK7j2UNo ratings yet
- Thyroid Gland An Diseases of Thyroid D Gland: Omc LectureDocument59 pagesThyroid Gland An Diseases of Thyroid D Gland: Omc LectureEdward MakemboNo ratings yet
- ОВБ-2 Ответы фулDocument70 pagesОВБ-2 Ответы фулMoldir AkynbayNo ratings yet
- Week 15 16 Module Biochem Lec EndocrinologyDocument19 pagesWeek 15 16 Module Biochem Lec EndocrinologyLy xyNo ratings yet
- Drugs Affecting The Endocrine System - PharmacologyDocument58 pagesDrugs Affecting The Endocrine System - PharmacologyMuhammad Riandy Lukman TanjungNo ratings yet



































































































Download as pdf or txt
You might also like
- 【机制】IL-12 and IL-23 Pathway Inhibition in Inflammatory Bowel DiseaseDocument14 pages【机制】IL-12 and IL-23 Pathway Inhibition in Inflammatory Bowel Diseasejona renNo ratings yet
- The Nuctemeron of Apollonius of TyanaDocument9 pagesThe Nuctemeron of Apollonius of Tyanacc vereNo ratings yet
- A Critical Appraisal of Amyloid-β-targeting Therapies for Alzheimer Disease 2019 ReviewDocument16 pagesA Critical Appraisal of Amyloid-β-targeting Therapies for Alzheimer Disease 2019 Review畏No ratings yet
- Immunity To MicrobesDocument25 pagesImmunity To MicrobestimcarasNo ratings yet
- Microbes and the Mind: The Impact of the Microbiome on Mental HealthFrom EverandMicrobes and the Mind: The Impact of the Microbiome on Mental HealthNo ratings yet
- Case 1 EndocrineDocument5 pagesCase 1 EndocrineRegine Mae EncinadaNo ratings yet
- Hypersensitivity 1 4Document62 pagesHypersensitivity 1 4Wahyudi YusmanNo ratings yet
- Innate ImmunityDocument14 pagesInnate Immunitydexter603No ratings yet
- Biomedicines 11 00115 v2Document22 pagesBiomedicines 11 00115 v2Wesley M.SantosNo ratings yet
- Jurnal AutismDocument10 pagesJurnal AutismAby SuryaNo ratings yet
- HypersensitivityDocument52 pagesHypersensitivityFuzti Fauzia100% (1)
- Artigo1 Galecki 2018Document23 pagesArtigo1 Galecki 2018Anuska ErikaNo ratings yet
- Modulo1 - FArtigo - Atores de Risco No Autismo - Pensando Fora Do CérebroDocument14 pagesModulo1 - FArtigo - Atores de Risco No Autismo - Pensando Fora Do CérebroViviane MartinsNo ratings yet
- Jurnal AutismeDocument11 pagesJurnal AutismeKabhithra ThiayagarajanNo ratings yet
- Andropause: Current Concepts: Keywords: Androgen Deficiency in Ageing Male, Late Onset Hypogonadism, TestosteroneDocument14 pagesAndropause: Current Concepts: Keywords: Androgen Deficiency in Ageing Male, Late Onset Hypogonadism, TestosteroneYariCárdenasNo ratings yet
- Autismo y AutoinmunidadDocument50 pagesAutismo y AutoinmunidadPsicoterapia InfantilNo ratings yet
- Membrane and Protein TraffickingDocument135 pagesMembrane and Protein TraffickingsujanupamNo ratings yet
- The Genetics of Autism 2004Document2 pagesThe Genetics of Autism 2004emma199No ratings yet
- Cytokines & Their ActionsDocument59 pagesCytokines & Their ActionsSharanabasappa DurgNo ratings yet
- Ciprofloxacin Induced Chondrotoxicity and Tendinopathy PDFDocument7 pagesCiprofloxacin Induced Chondrotoxicity and Tendinopathy PDFAvelox FloxNo ratings yet
- Genetics ArchitectureDocument9 pagesGenetics ArchitectureFatimah Dina AlkaffNo ratings yet
- Specific Immunity. FINALDocument29 pagesSpecific Immunity. FINALLUZVIMINDA GORDONo ratings yet
- Human Zinc DefDocument6 pagesHuman Zinc DefMiodrag MilicNo ratings yet
- The Female Protective Effect in Autism SDocument10 pagesThe Female Protective Effect in Autism SNps Caren RodriguezNo ratings yet
- Multiple Sclerosis Bench To Bed - Alexzander A.A. Asea, Fabiana G PDFDocument189 pagesMultiple Sclerosis Bench To Bed - Alexzander A.A. Asea, Fabiana G PDFHîrjoabă IoanNo ratings yet
- Immunobiology of Gestational Zinc Deficiency: Nele WellinghausenDocument6 pagesImmunobiology of Gestational Zinc Deficiency: Nele WellinghausenAnonymous dXdCD7D9UNo ratings yet
- Epigenetic SDocument19 pagesEpigenetic SNoor SabahNo ratings yet
- Articles On Wheat ToxicityDocument96 pagesArticles On Wheat ToxicityDr. Heath MotleyNo ratings yet
- Spikevax Previously Covid 19 Vaccine Moderna Epar Public Assessment Report - enDocument169 pagesSpikevax Previously Covid 19 Vaccine Moderna Epar Public Assessment Report - enBlessworkNo ratings yet
- The Implications of Vitamin D Status During Pregnancy On Mother and Her Developing ChildDocument11 pagesThe Implications of Vitamin D Status During Pregnancy On Mother and Her Developing ChildindahNo ratings yet
- The Role of Copper As A Modifier of Lipid Metabolism: January 2013Document23 pagesThe Role of Copper As A Modifier of Lipid Metabolism: January 2013Leni LismayantiNo ratings yet
- Processed Foods and Their Nutrition: Salim-ur-Rehman, Kanza Aziz Awan and Tahir ZahoorDocument29 pagesProcessed Foods and Their Nutrition: Salim-ur-Rehman, Kanza Aziz Awan and Tahir ZahoorM SNo ratings yet
- Brain-Heart InteractionsDocument22 pagesBrain-Heart Interactionscc vereNo ratings yet
- Principle of VaccineDocument10 pagesPrinciple of VaccineRasyid WicaksonoNo ratings yet
- The Immune Response in Autism - A New Frontier For Autism ResearchDocument15 pagesThe Immune Response in Autism - A New Frontier For Autism ResearchJorge AlvesNo ratings yet
- Immunology PDFDocument1 pageImmunology PDFTanushree PalNo ratings yet
- Tau Opa ThiesDocument22 pagesTau Opa ThiesIrina OdajiuNo ratings yet
- Difference Between Mast Cell and BasophilDocument3 pagesDifference Between Mast Cell and Basophilponbohacop100% (1)
- Matabolic PathwaysDocument11 pagesMatabolic PathwaysLevi100% (2)
- Research Paper Vaccines AutismDocument5 pagesResearch Paper Vaccines Autismc9rvz6mm100% (1)
- Biomol Tranduksi Sinyal Presentasi Kelompok Komunikasi Sel-1Document42 pagesBiomol Tranduksi Sinyal Presentasi Kelompok Komunikasi Sel-1ratnaekawatiNo ratings yet
- Ospolot 200 MG, Film-Coated Tablets: Summary of Product Characteristics (SPC)Document7 pagesOspolot 200 MG, Film-Coated Tablets: Summary of Product Characteristics (SPC)ddandan_2No ratings yet
- Liver Enzymes - ALT/ALT: DR - SarojaDocument15 pagesLiver Enzymes - ALT/ALT: DR - SarojaSaroja VeereshNo ratings yet
- Neuronal Signaling: July 2015Document12 pagesNeuronal Signaling: July 2015bening swarajiwaNo ratings yet
- A Systematic Review of Iodine Deficiency Among Women in The UKDocument10 pagesA Systematic Review of Iodine Deficiency Among Women in The UKanass.rami0676959544No ratings yet
- Approach To FatigueDocument27 pagesApproach To FatigueBasil Hussam100% (1)
- The Effects of Iodine Deficiency in Pregnancy and InfancyDocument10 pagesThe Effects of Iodine Deficiency in Pregnancy and InfancyerlyNo ratings yet
- Start Low and Go Slow 1-21-2014Document5 pagesStart Low and Go Slow 1-21-2014Ed JonesNo ratings yet
- Autism Spectrum Disorder Symptoms Improve With Combination Therapy Directed at Improving Gut Microbiota and Reducing InflammationDocument7 pagesAutism Spectrum Disorder Symptoms Improve With Combination Therapy Directed at Improving Gut Microbiota and Reducing InflammationSarah Naomi Jeanett ObenhoferNo ratings yet
- Xenobiotic MetabolismDocument64 pagesXenobiotic MetabolismBelajar dan berdoaNo ratings yet
- Thyroid Autoimmune DiseasesDocument21 pagesThyroid Autoimmune Diseasesmicheal1960No ratings yet
- 5-Alpha-Reductase Inhibitor PDFDocument8 pages5-Alpha-Reductase Inhibitor PDFP. GuadamuzNo ratings yet
- Biochemistry of Adaptive ImmunityDocument22 pagesBiochemistry of Adaptive Immunityshreyansh singhNo ratings yet
- 2021-Reviews in Basic and Clinical Gastroenterology and HepatologyDocument16 pages2021-Reviews in Basic and Clinical Gastroenterology and HepatologyÉden SiqueiraNo ratings yet
- @PIDs Curs 200903Document43 pages@PIDs Curs 200903Mohammad_Islam87No ratings yet
- Immunodeficiency: Faculty of Applied Science Department of Medical Lab. Ml3A, ML3C, ML3DDocument35 pagesImmunodeficiency: Faculty of Applied Science Department of Medical Lab. Ml3A, ML3C, ML3Dالدنيا ساعة فاجعلها طاعةNo ratings yet
- Matrix Metalloproteinases: The Most Important Pathway Involved With Periodontal DestructionDocument9 pagesMatrix Metalloproteinases: The Most Important Pathway Involved With Periodontal DestructionmochamadfadilNo ratings yet
- ClostridumDocument30 pagesClostridumFrancesca VargasNo ratings yet
- Metabolism of Vitamin DDocument36 pagesMetabolism of Vitamin DNisachon DenpraphaNo ratings yet
- Neuroendocrine Regulationof ImmunityDocument41 pagesNeuroendocrine Regulationof ImmunitynepretipNo ratings yet
- Immune Regulation by GlucocorticoidsDocument35 pagesImmune Regulation by GlucocorticoidsSyifa SariNo ratings yet
- Fimmu 10 01744Document20 pagesFimmu 10 01744Suryadi LimardiNo ratings yet
- VAShiva SystemsHealth Reading Vinod CurrentStatusofAdaptogensDocument11 pagesVAShiva SystemsHealth Reading Vinod CurrentStatusofAdaptogenscc vereNo ratings yet
- Autonomic Immune Vascular InteractionDocument9 pagesAutonomic Immune Vascular Interactioncc vereNo ratings yet
- Z. J. Lipowski (Auth.), P. Pichot, P. Berner, R. Wolf, K. Thau (Eds.) - Biological Psychiatry, Higher Nervous Activity-Springer US (1985)Document928 pagesZ. J. Lipowski (Auth.), P. Pichot, P. Berner, R. Wolf, K. Thau (Eds.) - Biological Psychiatry, Higher Nervous Activity-Springer US (1985)cc vereNo ratings yet
- Ox InflammationDocument15 pagesOx Inflammationcc vereNo ratings yet
- Oxytocin and VasopressinDocument19 pagesOxytocin and Vasopressincc vereNo ratings yet
- Wake Sleep CycleDocument11 pagesWake Sleep Cyclecc vereNo ratings yet
- Principles of Allostasis Optimal DesignDocument36 pagesPrinciples of Allostasis Optimal Designcc vereNo ratings yet
- Heart-Brain AxisDocument15 pagesHeart-Brain Axiscc vereNo ratings yet
- Brain-Heart InteractionsDocument22 pagesBrain-Heart Interactionscc vereNo ratings yet
- Stress Final Text 2016Document11 pagesStress Final Text 2016cc vereNo ratings yet
- Sensory Hepatic NervesDocument9 pagesSensory Hepatic Nervescc vereNo ratings yet
- Wa0041Document161 pagesWa0041SULDAANUL CAASHIQIINNo ratings yet
- Hyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesDocument6 pagesHyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesLeitavia D.No ratings yet
- Biology: Topic - Endocrine System Class-VIII Board - ICSEDocument3 pagesBiology: Topic - Endocrine System Class-VIII Board - ICSEItu DeyNo ratings yet
- Thyroid Gland Clinical Chemistry 2 (Laboratory) : LessonDocument4 pagesThyroid Gland Clinical Chemistry 2 (Laboratory) : LessonCherry Ann ColechaNo ratings yet
- Human Physiology Chapter 4 - EndDocument172 pagesHuman Physiology Chapter 4 - EndEmebet DebissaNo ratings yet
- Andrea Nakayama Hashimotos Institute 9-15-2014Document35 pagesAndrea Nakayama Hashimotos Institute 9-15-2014Vivek GuptaNo ratings yet
- DetailedapproaDocument65 pagesDetailedapproaMuhammed BarznjiNo ratings yet
- NCM 105 Nutrition and Diet LecDocument8 pagesNCM 105 Nutrition and Diet LecBi B BelleNo ratings yet
- 4 Lab ManualDocument160 pages4 Lab ManualAziz EzoNo ratings yet
- TIRMODDocument66 pagesTIRMODYaniNo ratings yet
- Final: LPL - Suvprabhat Pathology Lab Near Hospitsl Chowk (In Front of Zonal Hospital), Janakpur NepalDocument2 pagesFinal: LPL - Suvprabhat Pathology Lab Near Hospitsl Chowk (In Front of Zonal Hospital), Janakpur NepalAjay SharmaNo ratings yet
- Anatomy & Physiology of Thyroid GlandDocument5 pagesAnatomy & Physiology of Thyroid GlandJohnpaul DelapenaNo ratings yet
- Complications of MarasmusDocument3 pagesComplications of MarasmusNathania LongkutoyNo ratings yet
- Chapter 9 - Endocrine SystemDocument9 pagesChapter 9 - Endocrine SystemrishellemaepilonesNo ratings yet
- Thyroid DisordersDocument67 pagesThyroid DisordersMA 09No ratings yet
- Endocrine GlandsDocument14 pagesEndocrine GlandsVarsha Rai100% (1)
- Levothyroxine Interactions With Food and Dietary Supplements-A Systematic ReviewDocument20 pagesLevothyroxine Interactions With Food and Dietary Supplements-A Systematic Reviewalan_pedraza864No ratings yet
- Bio E1 Chapter 2 PDFDocument26 pagesBio E1 Chapter 2 PDFToto lstNo ratings yet
- Protocols For High-Risk Pregnancies - 2010 - Queenan - Appendix B Laboratory Values in Normal PregnancyDocument9 pagesProtocols For High-Risk Pregnancies - 2010 - Queenan - Appendix B Laboratory Values in Normal PregnancyHenry VillarosaNo ratings yet
- Tura KuDocument104 pagesTura KuFitzgerald BillyNo ratings yet
- Free Face Yoga Method Ebook Fumiko TakatsuDocument70 pagesFree Face Yoga Method Ebook Fumiko Takatsumagdalena0% (3)
- Total T3: For Use On The IMMULITE and Immulite 1000 SystemsDocument31 pagesTotal T3: For Use On The IMMULITE and Immulite 1000 SystemsEdgar Galván0% (1)
- Review of Hyperthyroidism As Per Ayurveda: Sirjana ShresthaDocument6 pagesReview of Hyperthyroidism As Per Ayurveda: Sirjana ShresthaSatyam SinghNo ratings yet
- Intro To EthologyDocument3 pagesIntro To EthologyRowzFerlTanutanNo ratings yet
- 5-Vitamin and MineralsDocument61 pages5-Vitamin and MineralsAnonymous 8hcK7j2UNo ratings yet
- Thyroid Gland An Diseases of Thyroid D Gland: Omc LectureDocument59 pagesThyroid Gland An Diseases of Thyroid D Gland: Omc LectureEdward MakemboNo ratings yet
- ОВБ-2 Ответы фулDocument70 pagesОВБ-2 Ответы фулMoldir AkynbayNo ratings yet
- Week 15 16 Module Biochem Lec EndocrinologyDocument19 pagesWeek 15 16 Module Biochem Lec EndocrinologyLy xyNo ratings yet
- Drugs Affecting The Endocrine System - PharmacologyDocument58 pagesDrugs Affecting The Endocrine System - PharmacologyMuhammad Riandy Lukman TanjungNo ratings yet