Download as pdf or txt
You might also like
- Realtime RadiographyDocument13 pagesRealtime RadiographySivirahulNo ratings yet
- Infant Breastfeeding Assessment Tool (IBFAT)Document1 pageInfant Breastfeeding Assessment Tool (IBFAT)Sena Kawawura100% (1)
- Va Inspector Report 3Document100 pagesVa Inspector Report 3Jeff MorrisNo ratings yet
- Active Learning: KVP (Kilo-Voltage Peak) : It'S The Highest Voltage That Will ProducedDocument5 pagesActive Learning: KVP (Kilo-Voltage Peak) : It'S The Highest Voltage That Will ProducedAquanamNo ratings yet
- Screen-Film Systems: X-Ray Photons X-Ray PhotonsDocument12 pagesScreen-Film Systems: X-Ray Photons X-Ray PhotonsSabinaNo ratings yet
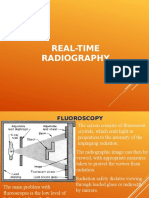
- Fluoroscopy: HistoryDocument5 pagesFluoroscopy: HistoryDidimo Antonio Paez ClavijoNo ratings yet
- 2015 - Evaluating Red Reflex and Surgeon Preference Between Nearly-Collimated and Focused Beam Microscope Illumination SystemsDocument10 pages2015 - Evaluating Red Reflex and Surgeon Preference Between Nearly-Collimated and Focused Beam Microscope Illumination Systemstung NguyenNo ratings yet
- ProposalDocument22 pagesProposalKD CarlosNo ratings yet
- Notes 20240508001650Document4 pagesNotes 20240508001650Waqas MahmoodNo ratings yet
- General Radio Graphic Image QualityDocument9 pagesGeneral Radio Graphic Image QualityRouben ParmanumNo ratings yet
- Ophthalmology Femtosecond LaserDocument5 pagesOphthalmology Femtosecond LaserChandrika MaluftiNo ratings yet
- Scoliosis ManagementDocument5 pagesScoliosis ManagementYandriyaneStephanieNo ratings yet
- Digital Radiography Artifacts PDFDocument9 pagesDigital Radiography Artifacts PDFYouness Ben TibariNo ratings yet
- Medical X-Ray Image Enhancement Method Based On DarkDocument4 pagesMedical X-Ray Image Enhancement Method Based On DarkNguyễn Nhật-NguyênNo ratings yet
- Realtime RadiographyDocument13 pagesRealtime RadiographySivirahulNo ratings yet
- Realtime RadiographyDocument13 pagesRealtime RadiographySivirahulNo ratings yet
- Experimental Eye Research: Xiaoxia Li, Miaoqin Wu, Luyi Zhang, Hui Liu, Lan Zhang, Jinjing HeDocument6 pagesExperimental Eye Research: Xiaoxia Li, Miaoqin Wu, Luyi Zhang, Hui Liu, Lan Zhang, Jinjing Hedella valeriaNo ratings yet
- Projection RadiographyDocument37 pagesProjection RadiographyAde WijayaNo ratings yet
- As OctDocument7 pagesAs OctRasha Mounir Abdel-Kader El-TanamlyNo ratings yet
- Ultrasound Guidance - PollardDocument72 pagesUltrasound Guidance - Pollardmasquebolso100% (3)
- Critical Issues in Breast Imaging by Vibro-AcoustographyDocument4 pagesCritical Issues in Breast Imaging by Vibro-AcoustographyDemian PereiraNo ratings yet
- InTech-Analog and Digital Systems of Imaging in RoentgenodiagnosticsDocument23 pagesInTech-Analog and Digital Systems of Imaging in RoentgenodiagnosticsAshleyNo ratings yet
- Medical Imaging Using Ionizing Radiation Optimization of Dose and Image Quality in FluoroscopyaDocument27 pagesMedical Imaging Using Ionizing Radiation Optimization of Dose and Image Quality in FluoroscopyaMurilo AssunçãoNo ratings yet
- Fluroscopy & Iitv SystemDocument87 pagesFluroscopy & Iitv SystemMunish DograNo ratings yet
- Jbo 018 111412Document9 pagesJbo 018 111412Duy ChâuNo ratings yet
- Intra-Undulator Measurements at VISA FELDocument4 pagesIntra-Undulator Measurements at VISA FELParticle Beam Physics LabNo ratings yet
- Whitepaper Clarity IqDocument11 pagesWhitepaper Clarity Iqboobesh kumar dNo ratings yet
- Introduction To Radiography, Fluoroscopy, and Tomosynthesis: Drew A. Torigian, MD, MA, FSARDocument5 pagesIntroduction To Radiography, Fluoroscopy, and Tomosynthesis: Drew A. Torigian, MD, MA, FSARMiguel Marcio Ortuño MejiaNo ratings yet
- Dose Reduction Techniques1Document4 pagesDose Reduction Techniques1eltonNo ratings yet
- Detection of Polycystic Ovary Syndrome From Ultrasound Images Using SIFT DescriptorsDocument5 pagesDetection of Polycystic Ovary Syndrome From Ultrasound Images Using SIFT DescriptorsBONFRINGNo ratings yet
- Ijmpcero 2016110709332094Document22 pagesIjmpcero 2016110709332094RaffaeleNo ratings yet
- Photovoltaic Restoration of Sight With High Visual Acuity: ArticlesDocument10 pagesPhotovoltaic Restoration of Sight With High Visual Acuity: ArticleswatsonNo ratings yet
- Xray Kub My Prep FinalDocument109 pagesXray Kub My Prep FinalphoenixibexNo ratings yet
- FluroscophyDocument39 pagesFluroscophyfathahillahNo ratings yet
- Analisis Perbandingan Medical Image Processing Dengan Image EnhancementDocument10 pagesAnalisis Perbandingan Medical Image Processing Dengan Image Enhancementbella arviantiNo ratings yet
- IWCIM Paques 1Document7 pagesIWCIM Paques 1binukirubaNo ratings yet
- Training Module Radiographic Positioning and AnatomyDocument47 pagesTraining Module Radiographic Positioning and AnatomyMark Anthony Salvador Kalaw100% (2)
- Clinical Review: Science, Medicine, and The FutureDocument4 pagesClinical Review: Science, Medicine, and The FutureDeepak KumarNo ratings yet
- Flexible and Broadband Colloidal Quantum Dots Photodiode Array For Pixel-Level X-Ray To Near-Infrared Image FusionDocument9 pagesFlexible and Broadband Colloidal Quantum Dots Photodiode Array For Pixel-Level X-Ray To Near-Infrared Image Fusion18877544451No ratings yet
- ERCP Radiology Basics 2003Document6 pagesERCP Radiology Basics 2003Alistair KohNo ratings yet
- Projection Radiography, Also Called ConventionalDocument11 pagesProjection Radiography, Also Called ConventionalRaziv Maulana UsmanNo ratings yet
- P Mid 15687575Document13 pagesP Mid 15687575Rute FidalgoNo ratings yet
- VivoDocument9 pagesVivoOlziihishig MungunshagaiNo ratings yet
- Computed Radiography Image Artifacts RevisitedDocument11 pagesComputed Radiography Image Artifacts RevisitedsiminithinNo ratings yet
- Sharma 2021Document10 pagesSharma 2021bahadur.oo.shahNo ratings yet
- Sample 2020 @purchasablebooks Pam Cherry, Angela M Duxbury Practical PDFDocument65 pagesSample 2020 @purchasablebooks Pam Cherry, Angela M Duxbury Practical PDFgladioacutoNo ratings yet
- FUNPHYS.3 E-M RadiationDocument36 pagesFUNPHYS.3 E-M RadiationshabanaNo ratings yet
- Visualization of Skin Penetration Using Confocal LaserDocument16 pagesVisualization of Skin Penetration Using Confocal Lasersandra hernandezNo ratings yet
- Breast Cancer Detection Using Infrared Spectral Pathology - 2021 - Clinical SpeDocument6 pagesBreast Cancer Detection Using Infrared Spectral Pathology - 2021 - Clinical SpevkvNo ratings yet
- 2013 Article 281Document5 pages2013 Article 281Nlife GNo ratings yet
- Digital Radiography. A Comparison With Modern Conventional ImagingDocument4 pagesDigital Radiography. A Comparison With Modern Conventional ImagingEka JuliantaraNo ratings yet
- MIGRT, Radiobioluminescence, and Nanoradioguidance in Radiation Therapy - Dr. Rao PapineniDocument2 pagesMIGRT, Radiobioluminescence, and Nanoradioguidance in Radiation Therapy - Dr. Rao PapineniPapineni LabsNo ratings yet
- 1329 FullDocument9 pages1329 FullNabita AuliaNo ratings yet
- Radiographicexposure 230926161509 83e25e60Document33 pagesRadiographicexposure 230926161509 83e25e60Saroj PoudelNo ratings yet
- Laser Dentistry ResearchDocument12 pagesLaser Dentistry Researchbehdad.geranmehrNo ratings yet
- Week 3 FLUOROSCOPY-15sept22Document43 pagesWeek 3 FLUOROSCOPY-15sept22fara latifa100% (1)
- Capitulo Mártonyi Lampara de Hendidura Libro Corenea Mannis 2023Document28 pagesCapitulo Mártonyi Lampara de Hendidura Libro Corenea Mannis 2023Sarah Camacho PinedaNo ratings yet
- 2018 - Image-Based Reconstruction of Tissue Scatterers Using Beam Steering For Ultrasound SimulationDocument13 pages2018 - Image-Based Reconstruction of Tissue Scatterers Using Beam Steering For Ultrasound Simulationshiyuan wangNo ratings yet
- Optoelectronic Retinal ProsthesisDocument13 pagesOptoelectronic Retinal ProsthesisSpoorthy HUNo ratings yet
- I1552 5783 57 9 Oct51Document18 pagesI1552 5783 57 9 Oct51Vladimir KobelevNo ratings yet
- LED-Based Photoacoustic Imaging: From Bench to BedsideFrom EverandLED-Based Photoacoustic Imaging: From Bench to BedsideMithun Kuniyil Ajith SinghNo ratings yet
- Fundamentals of Oral and Maxillofacial RadiologyFrom EverandFundamentals of Oral and Maxillofacial RadiologyRating: 4 out of 5 stars4/5 (1)
- Aa 11Document5 pagesAa 11Eriekafebriayana RNo ratings yet
- 2015 Article 779Document8 pages2015 Article 779Eriekafebriayana RNo ratings yet
- Ajns 10 276Document6 pagesAjns 10 276Eriekafebriayana RNo ratings yet
- Metabolic Syndrome and Risk of Mortality in Middle-Aged Versus Elderly Individuals: The Nord-Trøndelag Health Study (HUNT)Document8 pagesMetabolic Syndrome and Risk of Mortality in Middle-Aged Versus Elderly Individuals: The Nord-Trøndelag Health Study (HUNT)Eriekafebriayana RNo ratings yet
- A Study To Compare Maternal and Perinatal Outcome in Early vs. Late Onset PreeclampsiaDocument8 pagesA Study To Compare Maternal and Perinatal Outcome in Early vs. Late Onset PreeclampsiaEriekafebriayana RNo ratings yet
- Early - and Late-Onset Preeclampsia A ComprehensiveDocument10 pagesEarly - and Late-Onset Preeclampsia A ComprehensiveEriekafebriayana RNo ratings yet
- Midgut Volvulus: September 2020Document6 pagesMidgut Volvulus: September 2020Eriekafebriayana RNo ratings yet
- Metabolic Syndrome, Its Components, and Mortality in The ElderlyDocument6 pagesMetabolic Syndrome, Its Components, and Mortality in The ElderlyEriekafebriayana RNo ratings yet
- Metabolic Syndrome and All-Cause and Cardiovascular Mortality in An Italian Elderly PopulationDocument7 pagesMetabolic Syndrome and All-Cause and Cardiovascular Mortality in An Italian Elderly PopulationEriekafebriayana RNo ratings yet
- Namasitean 124Document6 pagesNamasitean 124Eriekafebriayana RNo ratings yet
- Savetamal 2008Document10 pagesSavetamal 2008Eriekafebriayana RNo ratings yet
- Molecular Embryology of The ForegutDocument8 pagesMolecular Embryology of The ForegutEriekafebriayana RNo ratings yet
- Trilogy of Foregut Midgut and Hindgut Atresias PreDocument5 pagesTrilogy of Foregut Midgut and Hindgut Atresias PreEriekafebriayana RNo ratings yet
- 44 - Imaging in Neuroemergency DR - Rohadi SP - BsDocument51 pages44 - Imaging in Neuroemergency DR - Rohadi SP - BsEriekafebriayana RNo ratings yet
- Schizophrenia An OverviewDocument12 pagesSchizophrenia An OverviewEriekafebriayana RNo ratings yet
- Intussusception in AdultsDocument12 pagesIntussusception in AdultsEriekafebriayana RNo ratings yet
- Deflazacort Therapeutic Index Relative Potency andDocument8 pagesDeflazacort Therapeutic Index Relative Potency andAna-Mihaela BalanuțaNo ratings yet
- 5ykgogrgmtd3pwbpedotjsidDocument10 pages5ykgogrgmtd3pwbpedotjsidKartik SharmaNo ratings yet
- Summary of BASICS OF DIFFUSION MRI PDFDocument13 pagesSummary of BASICS OF DIFFUSION MRI PDFParamitha AdriyatiNo ratings yet
- Comparison of Systemic Corticosteroid Preparations - UpToDateDocument1 pageComparison of Systemic Corticosteroid Preparations - UpToDateMarco Salinas ContrerasNo ratings yet
- Checklist For Administering Oxygen by Nasal CannulaDocument3 pagesChecklist For Administering Oxygen by Nasal CannulaNasrah TalusobNo ratings yet
- ... Rapid Complete Recovery From An Autism Spectrum Disorder After Treatment... With... Antifungal Drugs ...Document8 pages... Rapid Complete Recovery From An Autism Spectrum Disorder After Treatment... With... Antifungal Drugs ...Daniel GilbertoNo ratings yet
- Bài tập Tiếng Anh 11 Global Success Unit 1Document5 pagesBài tập Tiếng Anh 11 Global Success Unit 1monlove262No ratings yet
- Blood Test and Normal RangeDocument40 pagesBlood Test and Normal Rangeethirukumaran50% (2)
- Patient Satisfaction Following Orthognathic Surgical Correction of Skeletal Class III MalocclusionDocument9 pagesPatient Satisfaction Following Orthognathic Surgical Correction of Skeletal Class III MalocclusionAbles227 BlessNo ratings yet
- Literature Review 1Document7 pagesLiterature Review 1api-549225118No ratings yet
- Mapping GH Raber Kamis 1-9-2022Document11 pagesMapping GH Raber Kamis 1-9-2022McShadiq ZikryNo ratings yet
- Nutrition During Infancy: Presented By: Group 3Document50 pagesNutrition During Infancy: Presented By: Group 3Lynette EspejoNo ratings yet
- Tapan Majhi 10.12.21Document6 pagesTapan Majhi 10.12.21Suman MajhiNo ratings yet
- BPL Newsletter January 2012Document2 pagesBPL Newsletter January 2012BestPersonnelLTDNo ratings yet
- Mesoridazine Drug StudyDocument5 pagesMesoridazine Drug Studyshadow gonzalezNo ratings yet
- Brochure-Real-time PCR Detection Kit For Monkeypox VirusDocument2 pagesBrochure-Real-time PCR Detection Kit For Monkeypox VirusMouhamadou Habibi Keys TraoreNo ratings yet
- Post-Operative Instructions: Laparoscopic CholecystectomyDocument2 pagesPost-Operative Instructions: Laparoscopic Cholecystectomyrizwan234No ratings yet
- Presentation of Neurogenic Shock Within The Emergency Department - TaylorDocument6 pagesPresentation of Neurogenic Shock Within The Emergency Department - TaylorAnprtma kaunangNo ratings yet
- TC14Document3 pagesTC14FrancisNo ratings yet
- Concurrent Acute Poststreptococcal Glomerulonephritis andDocument42 pagesConcurrent Acute Poststreptococcal Glomerulonephritis andKardio UndipNo ratings yet
- Psychological Aspect of AgingDocument4 pagesPsychological Aspect of AgingMuhammad Wachid100% (1)
- Comparison Between Male and Female GametesDocument2 pagesComparison Between Male and Female GametesUZAIR MAHBUB BHUYAINNo ratings yet
- Rofecoxib Inhibits Heterotopic Ossification AfterDocument146 pagesRofecoxib Inhibits Heterotopic Ossification AfterHaqqi IslamiNo ratings yet
- Renal Diseases " Review "Document22 pagesRenal Diseases " Review "api-3827876No ratings yet
- TriamcinoloneDocument7 pagesTriamcinoloneziddin_ahmadNo ratings yet
- Extra Oral Examination of The Dental Patient: Primary Dental Journal March 2020Document7 pagesExtra Oral Examination of The Dental Patient: Primary Dental Journal March 2020muhammad nauvalNo ratings yet
- Nursing ProcessDocument45 pagesNursing ProcessSukmaErfiana100% (1)
- (SOAL) Literasi Bahasa Inggris 012Document6 pages(SOAL) Literasi Bahasa Inggris 012ZaachaanNo ratings yet