Download as docx, pdf, or txt
You might also like
- Pre Trial Brief: Petition For Declaration of Nullity of MarriageDocument3 pagesPre Trial Brief: Petition For Declaration of Nullity of MarriageMaria Lourdes P. Garcia94% (17)
- Ramboll APAC Brochure - 0123 - 1-3Document21 pagesRamboll APAC Brochure - 0123 - 1-3Franky KenNo ratings yet
- Team Manager's One-Day Tournament HandbookDocument24 pagesTeam Manager's One-Day Tournament HandbookDeeyana DeenNo ratings yet
- Developing A High Performance Organization in A VUCA WorldDocument12 pagesDeveloping A High Performance Organization in A VUCA Worldfeyza syifaNo ratings yet
- Study Guide For The Dental Technician ExaminationDocument64 pagesStudy Guide For The Dental Technician ExaminationAurora100% (3)
- Indigenous Languages Infant PDFDocument48 pagesIndigenous Languages Infant PDFDel MashiryNo ratings yet
- Division Memorandum - s2022 - 330 - DIVISION MONITORING AND EVALUATION OF SCHOOL READINESPREPAREDNESS TO FULL 5 DAYS IN-PERSON CLASSESDocument5 pagesDivision Memorandum - s2022 - 330 - DIVISION MONITORING AND EVALUATION OF SCHOOL READINESPREPAREDNESS TO FULL 5 DAYS IN-PERSON CLASSESjaniah CastilloNo ratings yet
- ANOS ZELONIA KATE Midterm ProfEd 3A BTVTEDDocument3 pagesANOS ZELONIA KATE Midterm ProfEd 3A BTVTEDZelonia Kate AnosNo ratings yet
- Origin and History of Arnis EquipmentDocument33 pagesOrigin and History of Arnis EquipmentRaniel RabieNo ratings yet
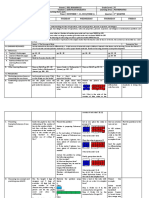
- DLL - Math 6 - Q2 - W1Document6 pagesDLL - Math 6 - Q2 - W1Janette Evangelista100% (1)
- Tle Notes 1.2Document4 pagesTle Notes 1.2Keesha Athena Villamil - CabrerosNo ratings yet
- Cyber Bullying: FormsDocument50 pagesCyber Bullying: FormsWalter Cañon CuentoNo ratings yet
- 9Document29 pages9yangNo ratings yet
- PCDA-Rev Advisory For Pensioners SPARSHDocument5 pagesPCDA-Rev Advisory For Pensioners SPARSHSandeep KumarNo ratings yet
- Gened CompileDocument163 pagesGened Compilerose PlopenioNo ratings yet
- Form No NTC 1-01 APPLICATION FOR RADIO OPERATOR EXAMINATIONDocument1 pageForm No NTC 1-01 APPLICATION FOR RADIO OPERATOR EXAMINATIONMa. Angela De GuzmanNo ratings yet
- Family Service Learning As A Tool To Strengthen Communities and FamiliesDocument3 pagesFamily Service Learning As A Tool To Strengthen Communities and FamiliesCulture & CommunityNo ratings yet
- DLL - Mapeh 5 - Q3 - W5Document7 pagesDLL - Mapeh 5 - Q3 - W5EDISON ALAWAGNo ratings yet
- Community Diagnosis Survey ToolDocument5 pagesCommunity Diagnosis Survey ToolLiza Mae MirandaNo ratings yet
- SocialScience MSDocument16 pagesSocialScience MSPelixiNo ratings yet
- B, Inggris 7Document15 pagesB, Inggris 7kesya dwiNo ratings yet
- CHILDRENS RIGHTS Grade 3Document10 pagesCHILDRENS RIGHTS Grade 3Eric MandaneNo ratings yet
- 1 - EPF - Form No. 11 (Sample)Document1 page1 - EPF - Form No. 11 (Sample)Rajdeep GaharwarNo ratings yet
- Arnel..... Customs and TraditionsDocument66 pagesArnel..... Customs and Traditionsoliver garcianoNo ratings yet
- Professional Ethics, Organizational Practices, and Culture of Trust by Entrepreneurial Managers of Selected Small and Medium Enterprises in BulacanDocument10 pagesProfessional Ethics, Organizational Practices, and Culture of Trust by Entrepreneurial Managers of Selected Small and Medium Enterprises in BulacanInternational Journal of Innovative Science and Research Technology100% (1)
- 21st CenturyDocument6 pages21st CenturyMonica BautistaNo ratings yet
- Pgi 2020Document50 pagesPgi 2020ShishirNo ratings yet
- Grade 7 Summer ActivityDocument7 pagesGrade 7 Summer ActivityAqsa KhanNo ratings yet
- ICT 7 Q1 Module1 Quarter IDocument23 pagesICT 7 Q1 Module1 Quarter Ialyana sophia limNo ratings yet
- Balita para Sa School PaperDocument4 pagesBalita para Sa School PaperMemie Jane Alvero Medallo100% (1)
- Learning Activity Sheet: Title: Kahulugan NG Matalinhagang Salita (Sawikain)Document7 pagesLearning Activity Sheet: Title: Kahulugan NG Matalinhagang Salita (Sawikain)kevinNo ratings yet
- Technical and Vocational Livelihood: Senior High SchoolDocument9 pagesTechnical and Vocational Livelihood: Senior High SchoolVanessa HadJeanxNo ratings yet
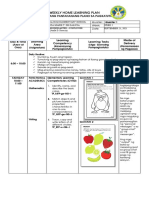
- Weekly Home Learning Plan: (Lingguhang Pantahanang Plano Sa Pagkatuto)Document5 pagesWeekly Home Learning Plan: (Lingguhang Pantahanang Plano Sa Pagkatuto)L Torrijos18No ratings yet
- NJSLA Testing 2022Document3 pagesNJSLA Testing 2022johnNo ratings yet
- VERON VAW ScriptDocument9 pagesVERON VAW ScriptAcinorev ArcenaNo ratings yet
- Department of Education: Individual Workweek Accomplishment ReportDocument5 pagesDepartment of Education: Individual Workweek Accomplishment ReportDhaiigandaNo ratings yet
- Edited - BEATON - DEMOLessonExemplar in ENGLISH 10 Differentiated Instruction 12 18 2020Document7 pagesEdited - BEATON - DEMOLessonExemplar in ENGLISH 10 Differentiated Instruction 12 18 2020Lanie HernandezNo ratings yet
- Philiri Booklet Grade 5 Pre-TestDocument20 pagesPhiliri Booklet Grade 5 Pre-TestMaria Carmela FornolesNo ratings yet
- Q4 HEALTH 8 Week 6Document4 pagesQ4 HEALTH 8 Week 6Catherine Joy De ChavezNo ratings yet
- Deposit Confirmation/Renewal AdviceDocument2 pagesDeposit Confirmation/Renewal AdviceVishwanath MuruganNo ratings yet
- Volleyball QuestionaireDocument5 pagesVolleyball QuestionaireGlaiza HigoNo ratings yet
- Eng10 Q3 W3 CapsletDocument9 pagesEng10 Q3 W3 CapsletErickson John EneroNo ratings yet
- Applying Data Mining Techniques To Predict Student Dropout: A Case StudyDocument6 pagesApplying Data Mining Techniques To Predict Student Dropout: A Case StudyBoris R. Pérez G.No ratings yet
- Verse Choir ScriptDocument4 pagesVerse Choir ScriptRenee Ross A. CondeNo ratings yet
- Location: Map of Naga CityDocument2 pagesLocation: Map of Naga Citycatherine boragayNo ratings yet
- CULTURAL EVENTS GUIDELINES Rev. 2019Document14 pagesCULTURAL EVENTS GUIDELINES Rev. 2019C-Jay ManingasNo ratings yet
- Stereotype and DiscriminationDocument7 pagesStereotype and DiscriminationChege DennisNo ratings yet
- Q2 Summative Test 2nd CYCLEDocument8 pagesQ2 Summative Test 2nd CYCLEJanessa EnteaNo ratings yet
- Number Theory Course Syllabus S.Y 2022-2023Document10 pagesNumber Theory Course Syllabus S.Y 2022-2023jncardanoNo ratings yet
- Aishwarya Viva - PPT ProjectDocument71 pagesAishwarya Viva - PPT Projectaishwarya damleNo ratings yet
- Medical SampleDocument1 pageMedical SampleI Komang Anom Gostap SidhartaNo ratings yet
- Grab Receipt ADR-165817592-8-006Document1 pageGrab Receipt ADR-165817592-8-006Kikz GusiNo ratings yet
- SMP 203 Systems Thinking 2nd Semester 2022 2023 F TadeoDocument18 pagesSMP 203 Systems Thinking 2nd Semester 2022 2023 F TadeoFernan Fangon TadeoNo ratings yet
- SLAC SESSION On How To LIVESTREAM Via Facebook Using OBS Studio ApplicationDocument5 pagesSLAC SESSION On How To LIVESTREAM Via Facebook Using OBS Studio ApplicationDexter MartinezNo ratings yet
- 2022 NEAP CV For Resource Speakers Gen OardeDocument3 pages2022 NEAP CV For Resource Speakers Gen OardeSVPSNo ratings yet
- BADM509 Mooc1 Combined Courseranotes PDFDocument237 pagesBADM509 Mooc1 Combined Courseranotes PDFLinaNo ratings yet
- 150LE Tube Bending Machine PDFDocument11 pages150LE Tube Bending Machine PDFAlex DreyerNo ratings yet
- Card Form 138Document23 pagesCard Form 138REBECCA TUBOGNo ratings yet
- Certificate of Participation - G7 G10Document66 pagesCertificate of Participation - G7 G10IrvinAironAmigableNo ratings yet
- Philippine FestivalsDocument20 pagesPhilippine FestivalsSet my Spirit Free CommunityNo ratings yet
- Candidate Information Sheet-V6Document4 pagesCandidate Information Sheet-V6ishNo ratings yet
- Candidate Application Form: Applicant DetailsDocument1 pageCandidate Application Form: Applicant DetailsVibha SikhwalNo ratings yet
- Introduction To Survey Methods: Prof. Dr. John T. ArokiasamyDocument41 pagesIntroduction To Survey Methods: Prof. Dr. John T. ArokiasamyThulasi tootsieNo ratings yet
- Form 5 Biology Notes Ms Kasthuri 2016Document11 pagesForm 5 Biology Notes Ms Kasthuri 2016KassyKasNo ratings yet
- List of Accredited Sars-Cov-2 Testing Laboratories As of May 31, 2021Document9 pagesList of Accredited Sars-Cov-2 Testing Laboratories As of May 31, 2021Shantal CapunponNo ratings yet
- O. A. U. Ile Ife O. A. U. Ile Ife: Obafemi Awolowo University, Ile-Ife Course Registration FormDocument1 pageO. A. U. Ile Ife O. A. U. Ile Ife: Obafemi Awolowo University, Ile-Ife Course Registration FormSteve MarkNo ratings yet
- Society For The Scientific Study of Religion, Wiley Journal For The Scientific Study of ReligionDocument22 pagesSociety For The Scientific Study of Religion, Wiley Journal For The Scientific Study of ReligionPetruPavălNo ratings yet
- (The Oily Press Lipid Library) Frank Gunstone - Lipids For Functional Foods and Nutraceuticals-Woodhead Publishing (2003) PDFDocument341 pages(The Oily Press Lipid Library) Frank Gunstone - Lipids For Functional Foods and Nutraceuticals-Woodhead Publishing (2003) PDFCamilo Andrés CastroNo ratings yet
- An Unusual Case of Corpse Dismemberment: Tomasz Konopka, MD, PHD, Filip Bolechała, MD, and Marcin Strona, MDDocument3 pagesAn Unusual Case of Corpse Dismemberment: Tomasz Konopka, MD, PHD, Filip Bolechała, MD, and Marcin Strona, MDGabriel GabrielNo ratings yet
- Wardlaws Perspectives in Nutrition A Functional Approach 1st Edition Byrd Bredbenner Solutions ManualDocument36 pagesWardlaws Perspectives in Nutrition A Functional Approach 1st Edition Byrd Bredbenner Solutions Manualbisterkeelvat.ydma3q100% (23)
- Boileau, DKK (2020) Organizational Ethnographic Case Studies Toward A New Generative In-Depth Qualitative Methodology For Health Care ResearchDocument17 pagesBoileau, DKK (2020) Organizational Ethnographic Case Studies Toward A New Generative In-Depth Qualitative Methodology For Health Care Researchbaehaqi17No ratings yet
- TRX Six Procedures PDFDocument8 pagesTRX Six Procedures PDFBabis XNo ratings yet
- Hatchet Essay QuestionsDocument7 pagesHatchet Essay QuestionspflhujbafNo ratings yet
- Week 009 Module A Concept of Activity ManagementDocument4 pagesWeek 009 Module A Concept of Activity ManagementMark John Paul CablingNo ratings yet
- Cancer Incidence in The Gaza Strip Facts & Figures 2015-2016Document13 pagesCancer Incidence in The Gaza Strip Facts & Figures 2015-2016PressureserveNo ratings yet
- The Dynamics of Public Policy by Adrian Kay PDFDocument158 pagesThe Dynamics of Public Policy by Adrian Kay PDFSadam Lashari100% (1)
- Physiology of TasteDocument45 pagesPhysiology of TasteDaffa YudhistiraNo ratings yet
- By Michael J. EllisonDocument12 pagesBy Michael J. EllisonA MNo ratings yet
- Clean and Hygienic Comfort Room Action PlanDocument2 pagesClean and Hygienic Comfort Room Action Plankariza pugalNo ratings yet
- Q4 Health 6 Long Quiz 1Document3 pagesQ4 Health 6 Long Quiz 1Shielanie EsclandaNo ratings yet
- InvestorPresentation Q4-FY21Document25 pagesInvestorPresentation Q4-FY21abijith reddyNo ratings yet
- Anatomy of CyclingDocument82 pagesAnatomy of Cyclingclaudia Torres100% (1)
- DNA Appliance FAQDocument3 pagesDNA Appliance FAQpopat78No ratings yet
- Shadow Work Journal Prompts Illustrated PDFDocument51 pagesShadow Work Journal Prompts Illustrated PDFkkccNo ratings yet
- Sigma MP 101 (US) EN SdsDocument9 pagesSigma MP 101 (US) EN SdsEduardo GarzaNo ratings yet
- Lecture No 01 Sports NutritionDocument36 pagesLecture No 01 Sports Nutritionmaryam khanNo ratings yet
- 600501Document78 pages600501ss105993100% (1)
- Literasi BHS InggrisDocument5 pagesLiterasi BHS InggrisFadil BaeNo ratings yet
- Neurology: CindyDocument32 pagesNeurology: CindyTaschiro YuliarthaNo ratings yet
- Osorio Ii Elementary School Referral System For Students in Crisis Physically, Verbally or Sexual AbuseDocument8 pagesOsorio Ii Elementary School Referral System For Students in Crisis Physically, Verbally or Sexual AbuseBenj AlejoNo ratings yet