
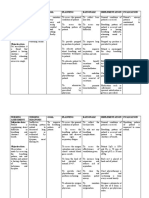
Assessment On Respiratory Problems
Assessment On Respiratory Problems
You might also like
- NCP Acl TearDocument2 pagesNCP Acl TearEd Pascasio100% (2)
- A Cog Practice Bulletin 175 Ultrasound in PregnancyDocument16 pagesA Cog Practice Bulletin 175 Ultrasound in Pregnancyansel7No ratings yet
- Resp Assessment 2 PDFDocument5 pagesResp Assessment 2 PDFsista mulyaniNo ratings yet
- 019 - Ulil Chiqmatussa'diah - EPN 2 - Assessment On Respiratory Problems..Document7 pages019 - Ulil Chiqmatussa'diah - EPN 2 - Assessment On Respiratory Problems..Setiaty PandiaNo ratings yet
- Defining CharacteristicsDocument2 pagesDefining CharacteristicsAngel MayNo ratings yet
- Fundamentals of Lung Auscultation: New England Journal of Medicine February 2014Document9 pagesFundamentals of Lung Auscultation: New England Journal of Medicine February 2014ANTJE ORNELLA REYESNo ratings yet
- NURSING CARE PLAN - JayDocument8 pagesNURSING CARE PLAN - JayJaylord VerazonNo ratings yet
- Advanced Life Support: Siska Christianingsih, S.Kep.,Ns.M.KepDocument31 pagesAdvanced Life Support: Siska Christianingsih, S.Kep.,Ns.M.KepFlorenciaNo ratings yet
- Nursing Care Plan: Cues Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Objectives Interventions Rationale EvaluationBianca Mikaela DosdosNo ratings yet
- Fundamentals of Lung Auscultation: Review ArticleDocument8 pagesFundamentals of Lung Auscultation: Review ArticleGabriela LosadaNo ratings yet
- A.) Signs and Symptoms/Assessment: B.) Diagnostic ProceduresDocument13 pagesA.) Signs and Symptoms/Assessment: B.) Diagnostic ProceduresJake Yvan DizonNo ratings yet
- Chest PhysiotherapyDocument17 pagesChest PhysiotherapySupriya chhetryNo ratings yet
- ?1 - Chest X-Ray Interpretation - A Structured Approach - Radiology - OSCEDocument14 pages?1 - Chest X-Ray Interpretation - A Structured Approach - Radiology - OSCEVerónicaNo ratings yet
- Endotracheal Tubes: Early Detection of Oesophageal IntubationDocument5 pagesEndotracheal Tubes: Early Detection of Oesophageal IntubationIkea BalhonNo ratings yet
- Fundamentals of Lung AuscultationDocument9 pagesFundamentals of Lung AuscultationSorin CalinNo ratings yet
- Airway Management For Nurses PDFDocument6 pagesAirway Management For Nurses PDFarizza ramosNo ratings yet
- Thoracic and Lung Assessment: College of Nursing and Allied Health Sciences Maasin City, Southern LeyteDocument4 pagesThoracic and Lung Assessment: College of Nursing and Allied Health Sciences Maasin City, Southern LeytePrincess Diana Jean ModesteNo ratings yet
- How To Auscultate For Heart Sounds in Adults: Evidence & PracticeDocument3 pagesHow To Auscultate For Heart Sounds in Adults: Evidence & Practiceangela mamauagNo ratings yet
- 1 s2.0 S0964339799800743 Main PDFDocument10 pages1 s2.0 S0964339799800743 Main PDFROSANNA BUCAGNo ratings yet
- Equipment Used in Physical ExaminationDocument5 pagesEquipment Used in Physical ExaminationMary Kaye Silvestre0% (1)
- 06 Paediatric and Child Health June2009 PulmonologyDocument51 pages06 Paediatric and Child Health June2009 PulmonologyVivek Edamuriyil RamesanNo ratings yet
- Mechanics of Circular Breathing in Wind MusiciansDocument8 pagesMechanics of Circular Breathing in Wind MusiciansjwmmdNo ratings yet
- Cardio Pulmonary Resuscitation (CPR) : Tracey Gibson, Elaine Cole & Anne McleodDocument6 pagesCardio Pulmonary Resuscitation (CPR) : Tracey Gibson, Elaine Cole & Anne McleodRETINA CREATIONSNo ratings yet
- Ch17 Lungsrespi Physical AssessmentDocument2 pagesCh17 Lungsrespi Physical AssessmentJherico Matthew AsisNo ratings yet
- Anatomy RespirationDocument29 pagesAnatomy RespirationPatricia Rosabelle RoñoNo ratings yet
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument5 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal Choudhary100% (1)
- Lungs and ThoracicDocument66 pagesLungs and ThoracicJoyce Jacobe0% (1)
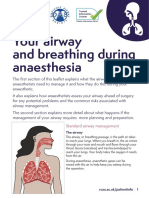
- Your Airway and Breathing During AnaesthesiaDocument7 pagesYour Airway and Breathing During AnaesthesiagshjfkNo ratings yet
- HA Finals ReviewerDocument15 pagesHA Finals ReviewerMichelle Rose RodaviaNo ratings yet
- Preop EvaluationDocument3 pagesPreop EvaluationRhea JavierNo ratings yet
- Pulmonary Auscultation PDFDocument5 pagesPulmonary Auscultation PDFThatikala AbhilashNo ratings yet
- RLE RequirementsDocument24 pagesRLE RequirementsNurhussien GalibNo ratings yet
- 175 Ultrasound in Pregnancy PDFDocument16 pages175 Ultrasound in Pregnancy PDFNestor FerrerNo ratings yet
- Steps of CPR ProcedureDocument8 pagesSteps of CPR ProcedureKrupa Jyothi PerumallaNo ratings yet
- Difficulty of BreathingDocument4 pagesDifficulty of BreathingNur SetsuNo ratings yet
- Assessment Nursing Diagnossis Scientific Basis Goal Nursing Intervention Rationale Evaluation IndependentDocument10 pagesAssessment Nursing Diagnossis Scientific Basis Goal Nursing Intervention Rationale Evaluation IndependentPamela laquindanumNo ratings yet
- Ultrasound of The Pediatric Chest2019Document13 pagesUltrasound of The Pediatric Chest2019JHONATAN MATA ARANDANo ratings yet
- Specific Competencies/ Objectives Content Time Allotment Methodology Resources EvaluationDocument21 pagesSpecific Competencies/ Objectives Content Time Allotment Methodology Resources EvaluationBert HolandaNo ratings yet
- CPG Chronic CoughDocument14 pagesCPG Chronic Coughmichael ryan canilangNo ratings yet
- ABADINGO-Pedia Nursing Care PlanDocument3 pagesABADINGO-Pedia Nursing Care PlanAndrea Abadingo100% (1)
- Small Animal Cardiology Auscultation - Vet VisionsDocument1 pageSmall Animal Cardiology Auscultation - Vet Visionsyuaifafa25No ratings yet
- 2022 PROCEDURE For Respiratory System Assessment With Findings FINALDocument4 pages2022 PROCEDURE For Respiratory System Assessment With Findings FINALJozelle HenryNo ratings yet
- DANDY PUTRA SURYA (2014901056) - NCP Ineffective Breathing PatternDocument10 pagesDANDY PUTRA SURYA (2014901056) - NCP Ineffective Breathing PatternAlri LestariNo ratings yet
- Session 4 - Performing Respiratory System ExaminationDocument26 pagesSession 4 - Performing Respiratory System ExaminationOtsward OwdenNo ratings yet
- Anatomy and Physiology of The Larynx and Hypopharynx: January 2010Document13 pagesAnatomy and Physiology of The Larynx and Hypopharynx: January 2010Listya ParamitaNo ratings yet
- The Role of Thoracic Expansion Exercises During The Active Cycle of Breathing TechniquesDocument9 pagesThe Role of Thoracic Expansion Exercises During The Active Cycle of Breathing TechniquesElan R.S.No ratings yet
- NCP On Ineffective Airway Clearance Nursing Diagnosi S Planning Nursing Interventions Implementatio N Evaluation Subjective: IndependentDocument10 pagesNCP On Ineffective Airway Clearance Nursing Diagnosi S Planning Nursing Interventions Implementatio N Evaluation Subjective: IndependentSheryhan Tahir BayleNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveDocument4 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjectivecammel ramos100% (1)
- Basic Life Support - Adult: First Issued By/date Issue Planned Review DateDocument15 pagesBasic Life Support - Adult: First Issued By/date Issue Planned Review DateyvesramosNo ratings yet
- NCP For Scenario BreathingDocument4 pagesNCP For Scenario Breathingmy moznNo ratings yet
- 44 CPR PDFDocument14 pages44 CPR PDFBramantyo NugrosNo ratings yet
- Aagaard Et Al. - 2018 - Timing of Focused Cardiac Ultrasound During Advanced Life Support - A Prospective Clinical StudyDocument6 pagesAagaard Et Al. - 2018 - Timing of Focused Cardiac Ultrasound During Advanced Life Support - A Prospective Clinical StudyVille SalmensuuNo ratings yet
- 3-Column Notes 1. What? 2. So What? 3. Now What?: Respiratory SystemDocument1 page3-Column Notes 1. What? 2. So What? 3. Now What?: Respiratory SystemalyssaNo ratings yet
- Physical Examination of The Respiratory SystemDocument11 pagesPhysical Examination of The Respiratory SystemMark CatabijanNo ratings yet
- Plan of Care Patient Independent-2 PDFDocument1 pagePlan of Care Patient Independent-2 PDFHilary AlvaradoNo ratings yet
- Lab Guide: Respiratory AssessmentDocument10 pagesLab Guide: Respiratory AssessmentDaisy MellaNo ratings yet
- Health AssessmentDocument35 pagesHealth AssessmentKm GaputanNo ratings yet
- Group 6 Group Case Study DONEDocument5 pagesGroup 6 Group Case Study DONEE.R.ONo ratings yet
- Steps of CPR ProcedureDocument8 pagesSteps of CPR ProcedureKrupa JyothirmaiNo ratings yet
- Seminars in Fetal & Neonatal Medicine: Steven M. Donn, Sunil K. SinhaDocument6 pagesSeminars in Fetal & Neonatal Medicine: Steven M. Donn, Sunil K. SinhadeniNo ratings yet
- High Resolution and High Definition Anorectal ManometryFrom EverandHigh Resolution and High Definition Anorectal ManometryMassimo BelliniNo ratings yet
- 019 - Ulil Chiqmatuss'diah - KMB 1Document4 pages019 - Ulil Chiqmatuss'diah - KMB 1Setiaty PandiaNo ratings yet
- 019 - Ulil Chiqmatussa'diah - EPN 2 - Assessment On Respiratory Problems..Document7 pages019 - Ulil Chiqmatussa'diah - EPN 2 - Assessment On Respiratory Problems..Setiaty PandiaNo ratings yet
- Simple East Asian Landscape Campaign - by SlidesgoDocument54 pagesSimple East Asian Landscape Campaign - by SlidesgoSetiaty PandiaNo ratings yet
- Jurnal KMB Diva - 015Document10 pagesJurnal KMB Diva - 015Setiaty PandiaNo ratings yet
- 4927 20042 1 PBDocument7 pages4927 20042 1 PBSetiaty PandiaNo ratings yet
- Qi Muslimah Talk 1 Ivana FixDocument16 pagesQi Muslimah Talk 1 Ivana FixSetiaty PandiaNo ratings yet
- Patient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentDocument5 pagesPatient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentSetiaty PandiaNo ratings yet
- 1385 FullDocument10 pages1385 FullSetiaty PandiaNo ratings yet
- Patient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentDocument5 pagesPatient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentSetiaty PandiaNo ratings yet
- Hubungan Tingkat Kecemasan Dengan Tingkat Kemandirian Activities of Daily Living Pada LansiaDocument8 pagesHubungan Tingkat Kecemasan Dengan Tingkat Kemandirian Activities of Daily Living Pada LansiaSetiaty PandiaNo ratings yet
- JCM 10 00522 v2Document12 pagesJCM 10 00522 v2Setiaty PandiaNo ratings yet
- Impact of Osteoarthritis On Activities of Daily LiDocument9 pagesImpact of Osteoarthritis On Activities of Daily LiSetiaty PandiaNo ratings yet
- Alat Ukur Untuk Menilai Kemampuan Fungsional Pasien Dengan Osteoartritis Lutut: Tinjauan PustakaDocument6 pagesAlat Ukur Untuk Menilai Kemampuan Fungsional Pasien Dengan Osteoartritis Lutut: Tinjauan PustakaSetiaty PandiaNo ratings yet
- Reike DIyah Setiawati - 042 - PSIK ADocument28 pagesReike DIyah Setiawati - 042 - PSIK ASetiaty PandiaNo ratings yet
- Health and Quality of Life OutcomesDocument8 pagesHealth and Quality of Life OutcomesSetiaty PandiaNo ratings yet
- Progress in Disaster Science: Jeremy Spoon, Drew Gerkey, Ram B. Chhetri, Alisa Rai, Umesh Basnet, Chelsea E. HunterDocument15 pagesProgress in Disaster Science: Jeremy Spoon, Drew Gerkey, Ram B. Chhetri, Alisa Rai, Umesh Basnet, Chelsea E. HunterSetiaty PandiaNo ratings yet
- Vital Signs and Monitoring - Podcast - IntermediateDocument4 pagesVital Signs and Monitoring - Podcast - IntermediateSetiaty PandiaNo ratings yet
- Material - Using Equipment For Patients' Examination - 019 - Ulil ChiqmatussadiahDocument2 pagesMaterial - Using Equipment For Patients' Examination - 019 - Ulil ChiqmatussadiahSetiaty PandiaNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Terjadinya PreeklampsiaDocument13 pagesFaktor-Faktor Yang Berhubungan Dengan Terjadinya PreeklampsiaSetiaty PandiaNo ratings yet
- Consulatation Liaison Psychiatry English Lecture 2012 10Document58 pagesConsulatation Liaison Psychiatry English Lecture 2012 10Setiaty PandiaNo ratings yet
- 116-Article Text-415-1-10-20190507Document8 pages116-Article Text-415-1-10-20190507Setiaty PandiaNo ratings yet
- Alasan Dilakukannya 4 Kali Amandemen Uud 1945 Tujuan Dan Sejarah PerkembanganDocument11 pagesAlasan Dilakukannya 4 Kali Amandemen Uud 1945 Tujuan Dan Sejarah PerkembanganSetiaty PandiaNo ratings yet
- Deteksi Mycobacterium Tuberculosis Pada Sampel Sputum Menggunakan Teknik Loop-Mediated Isothermal Amplification (LAMP-TB)Document7 pagesDeteksi Mycobacterium Tuberculosis Pada Sampel Sputum Menggunakan Teknik Loop-Mediated Isothermal Amplification (LAMP-TB)Setiaty PandiaNo ratings yet
- Management of Lymphatic Malformations in ChildrenDocument8 pagesManagement of Lymphatic Malformations in ChildrenAyuRosemeiliaDewiNo ratings yet
- Adrenaline (Anaethesia Tutorial of The Week)Document8 pagesAdrenaline (Anaethesia Tutorial of The Week)Raisa AriesthaNo ratings yet
- VenoferDocument13 pagesVenoferLuciano H.Vivas M.No ratings yet
- Rizal FinalsDocument9 pagesRizal FinalsAnonymous 5DiMa95W100% (1)
- Hankin - 1998 - Development of Depression From Preadolescence To AdulthoodDocument13 pagesHankin - 1998 - Development of Depression From Preadolescence To AdulthoodHanni JuhaszNo ratings yet
- Post Cardiac Arrest CareDocument28 pagesPost Cardiac Arrest CareAkib ArmanNo ratings yet
- Migraine Diagnosis and TreatmentDocument19 pagesMigraine Diagnosis and TreatmentMagdalila Pua RosalesNo ratings yet
- Kindergarten RhymesDocument15 pagesKindergarten RhymesAkshit R Shah100% (1)
- Public Health Laws: Romeo R. Andaya, MD, MSCPD, PHD, Fpafp Chair, DPMCH Uph-DjgtmuDocument8 pagesPublic Health Laws: Romeo R. Andaya, MD, MSCPD, PHD, Fpafp Chair, DPMCH Uph-DjgtmuKatNo ratings yet
- PhilHealth - ClaimForm2 1Document2 pagesPhilHealth - ClaimForm2 1Harold Kirby TanNo ratings yet
- Warfarin Mechanism of Action, Indications AtfDocument4 pagesWarfarin Mechanism of Action, Indications AtfAmir mohammad moori MohammadiNo ratings yet
- Craig Sims, Dana Weber, Chris Johnson - A Guide To Pediatric Anesthesia (2020, Springer International Publishing)Document535 pagesCraig Sims, Dana Weber, Chris Johnson - A Guide To Pediatric Anesthesia (2020, Springer International Publishing)cheechengNo ratings yet
- Medical Surgical Skills Checklist PDFDocument5 pagesMedical Surgical Skills Checklist PDFHussain R Al-MidaniNo ratings yet
- MHS MRI Consent FormDocument1 pageMHS MRI Consent Formjulia sabadellNo ratings yet
- Chapter 1: Introduction To Operative DentistryDocument11 pagesChapter 1: Introduction To Operative DentistryMariam AdnanNo ratings yet
- Anti-Drug Essay Writing Competition 2011 Full DocumentDocument13 pagesAnti-Drug Essay Writing Competition 2011 Full DocumentqueenklNo ratings yet
- A Field Manual of Camel Diseases Traditional and Modern Health Care For The DromedaryDocument273 pagesA Field Manual of Camel Diseases Traditional and Modern Health Care For The DromedaryHenrique100% (3)
- 6BI01 01R Que 20130521Document24 pages6BI01 01R Que 20130521karan79No ratings yet
- Case Study: Cushing and AddisonDocument4 pagesCase Study: Cushing and AddisonJeff ValdezNo ratings yet
- A Case of Pica On A 6-Year-Old Child From MedanDocument3 pagesA Case of Pica On A 6-Year-Old Child From MedanatikahnurhNo ratings yet
- LVS Chronic Pain WsDocument49 pagesLVS Chronic Pain WsdtncorreoNo ratings yet
- Daftar Pustaka ReferatDocument2 pagesDaftar Pustaka ReferatBetharlitha PurLikaNo ratings yet
- Captain of The Ship DoctrineDocument3 pagesCaptain of The Ship DoctrineAllison CuevasNo ratings yet
- BPPV - Benign Paroxysmal Positional VertigoDocument7 pagesBPPV - Benign Paroxysmal Positional VertigoYaser BarrawazNo ratings yet
- Eye HXDocument2 pagesEye HXAnishilNo ratings yet
- Dursch SmithDocument2 pagesDursch Smithapi-708256548No ratings yet
- Approved: Tertiary HospitalsDocument26 pagesApproved: Tertiary Hospitalsmurtada gubaNo ratings yet
- Nursing Care For Child With Autoimmune Diseases & GI DisordersDocument4 pagesNursing Care For Child With Autoimmune Diseases & GI Disordersbunso padillaNo ratings yet
- Nursingcrib Com NURSING CARE PLAN Spontaneous AbortionDocument2 pagesNursingcrib Com NURSING CARE PLAN Spontaneous AbortionMina RacadioNo ratings yet












































































































Download as pdf or txt
You might also like
- NCP Acl TearDocument2 pagesNCP Acl TearEd Pascasio100% (2)
- A Cog Practice Bulletin 175 Ultrasound in PregnancyDocument16 pagesA Cog Practice Bulletin 175 Ultrasound in Pregnancyansel7No ratings yet
- Resp Assessment 2 PDFDocument5 pagesResp Assessment 2 PDFsista mulyaniNo ratings yet
- 019 - Ulil Chiqmatussa'diah - EPN 2 - Assessment On Respiratory Problems..Document7 pages019 - Ulil Chiqmatussa'diah - EPN 2 - Assessment On Respiratory Problems..Setiaty PandiaNo ratings yet
- Defining CharacteristicsDocument2 pagesDefining CharacteristicsAngel MayNo ratings yet
- Fundamentals of Lung Auscultation: New England Journal of Medicine February 2014Document9 pagesFundamentals of Lung Auscultation: New England Journal of Medicine February 2014ANTJE ORNELLA REYESNo ratings yet
- NURSING CARE PLAN - JayDocument8 pagesNURSING CARE PLAN - JayJaylord VerazonNo ratings yet
- Advanced Life Support: Siska Christianingsih, S.Kep.,Ns.M.KepDocument31 pagesAdvanced Life Support: Siska Christianingsih, S.Kep.,Ns.M.KepFlorenciaNo ratings yet
- Nursing Care Plan: Cues Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Objectives Interventions Rationale EvaluationBianca Mikaela DosdosNo ratings yet
- Fundamentals of Lung Auscultation: Review ArticleDocument8 pagesFundamentals of Lung Auscultation: Review ArticleGabriela LosadaNo ratings yet
- A.) Signs and Symptoms/Assessment: B.) Diagnostic ProceduresDocument13 pagesA.) Signs and Symptoms/Assessment: B.) Diagnostic ProceduresJake Yvan DizonNo ratings yet
- Chest PhysiotherapyDocument17 pagesChest PhysiotherapySupriya chhetryNo ratings yet
- ?1 - Chest X-Ray Interpretation - A Structured Approach - Radiology - OSCEDocument14 pages?1 - Chest X-Ray Interpretation - A Structured Approach - Radiology - OSCEVerónicaNo ratings yet
- Endotracheal Tubes: Early Detection of Oesophageal IntubationDocument5 pagesEndotracheal Tubes: Early Detection of Oesophageal IntubationIkea BalhonNo ratings yet
- Fundamentals of Lung AuscultationDocument9 pagesFundamentals of Lung AuscultationSorin CalinNo ratings yet
- Airway Management For Nurses PDFDocument6 pagesAirway Management For Nurses PDFarizza ramosNo ratings yet
- Thoracic and Lung Assessment: College of Nursing and Allied Health Sciences Maasin City, Southern LeyteDocument4 pagesThoracic and Lung Assessment: College of Nursing and Allied Health Sciences Maasin City, Southern LeytePrincess Diana Jean ModesteNo ratings yet
- How To Auscultate For Heart Sounds in Adults: Evidence & PracticeDocument3 pagesHow To Auscultate For Heart Sounds in Adults: Evidence & Practiceangela mamauagNo ratings yet
- 1 s2.0 S0964339799800743 Main PDFDocument10 pages1 s2.0 S0964339799800743 Main PDFROSANNA BUCAGNo ratings yet
- Equipment Used in Physical ExaminationDocument5 pagesEquipment Used in Physical ExaminationMary Kaye Silvestre0% (1)
- 06 Paediatric and Child Health June2009 PulmonologyDocument51 pages06 Paediatric and Child Health June2009 PulmonologyVivek Edamuriyil RamesanNo ratings yet
- Mechanics of Circular Breathing in Wind MusiciansDocument8 pagesMechanics of Circular Breathing in Wind MusiciansjwmmdNo ratings yet
- Cardio Pulmonary Resuscitation (CPR) : Tracey Gibson, Elaine Cole & Anne McleodDocument6 pagesCardio Pulmonary Resuscitation (CPR) : Tracey Gibson, Elaine Cole & Anne McleodRETINA CREATIONSNo ratings yet
- Ch17 Lungsrespi Physical AssessmentDocument2 pagesCh17 Lungsrespi Physical AssessmentJherico Matthew AsisNo ratings yet
- Anatomy RespirationDocument29 pagesAnatomy RespirationPatricia Rosabelle RoñoNo ratings yet
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument5 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal Choudhary100% (1)
- Lungs and ThoracicDocument66 pagesLungs and ThoracicJoyce Jacobe0% (1)
- Your Airway and Breathing During AnaesthesiaDocument7 pagesYour Airway and Breathing During AnaesthesiagshjfkNo ratings yet
- HA Finals ReviewerDocument15 pagesHA Finals ReviewerMichelle Rose RodaviaNo ratings yet
- Preop EvaluationDocument3 pagesPreop EvaluationRhea JavierNo ratings yet
- Pulmonary Auscultation PDFDocument5 pagesPulmonary Auscultation PDFThatikala AbhilashNo ratings yet
- RLE RequirementsDocument24 pagesRLE RequirementsNurhussien GalibNo ratings yet
- 175 Ultrasound in Pregnancy PDFDocument16 pages175 Ultrasound in Pregnancy PDFNestor FerrerNo ratings yet
- Steps of CPR ProcedureDocument8 pagesSteps of CPR ProcedureKrupa Jyothi PerumallaNo ratings yet
- Difficulty of BreathingDocument4 pagesDifficulty of BreathingNur SetsuNo ratings yet
- Assessment Nursing Diagnossis Scientific Basis Goal Nursing Intervention Rationale Evaluation IndependentDocument10 pagesAssessment Nursing Diagnossis Scientific Basis Goal Nursing Intervention Rationale Evaluation IndependentPamela laquindanumNo ratings yet
- Ultrasound of The Pediatric Chest2019Document13 pagesUltrasound of The Pediatric Chest2019JHONATAN MATA ARANDANo ratings yet
- Specific Competencies/ Objectives Content Time Allotment Methodology Resources EvaluationDocument21 pagesSpecific Competencies/ Objectives Content Time Allotment Methodology Resources EvaluationBert HolandaNo ratings yet
- CPG Chronic CoughDocument14 pagesCPG Chronic Coughmichael ryan canilangNo ratings yet
- ABADINGO-Pedia Nursing Care PlanDocument3 pagesABADINGO-Pedia Nursing Care PlanAndrea Abadingo100% (1)
- Small Animal Cardiology Auscultation - Vet VisionsDocument1 pageSmall Animal Cardiology Auscultation - Vet Visionsyuaifafa25No ratings yet
- 2022 PROCEDURE For Respiratory System Assessment With Findings FINALDocument4 pages2022 PROCEDURE For Respiratory System Assessment With Findings FINALJozelle HenryNo ratings yet
- DANDY PUTRA SURYA (2014901056) - NCP Ineffective Breathing PatternDocument10 pagesDANDY PUTRA SURYA (2014901056) - NCP Ineffective Breathing PatternAlri LestariNo ratings yet
- Session 4 - Performing Respiratory System ExaminationDocument26 pagesSession 4 - Performing Respiratory System ExaminationOtsward OwdenNo ratings yet
- Anatomy and Physiology of The Larynx and Hypopharynx: January 2010Document13 pagesAnatomy and Physiology of The Larynx and Hypopharynx: January 2010Listya ParamitaNo ratings yet
- The Role of Thoracic Expansion Exercises During The Active Cycle of Breathing TechniquesDocument9 pagesThe Role of Thoracic Expansion Exercises During The Active Cycle of Breathing TechniquesElan R.S.No ratings yet
- NCP On Ineffective Airway Clearance Nursing Diagnosi S Planning Nursing Interventions Implementatio N Evaluation Subjective: IndependentDocument10 pagesNCP On Ineffective Airway Clearance Nursing Diagnosi S Planning Nursing Interventions Implementatio N Evaluation Subjective: IndependentSheryhan Tahir BayleNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveDocument4 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjectivecammel ramos100% (1)
- Basic Life Support - Adult: First Issued By/date Issue Planned Review DateDocument15 pagesBasic Life Support - Adult: First Issued By/date Issue Planned Review DateyvesramosNo ratings yet
- NCP For Scenario BreathingDocument4 pagesNCP For Scenario Breathingmy moznNo ratings yet
- 44 CPR PDFDocument14 pages44 CPR PDFBramantyo NugrosNo ratings yet
- Aagaard Et Al. - 2018 - Timing of Focused Cardiac Ultrasound During Advanced Life Support - A Prospective Clinical StudyDocument6 pagesAagaard Et Al. - 2018 - Timing of Focused Cardiac Ultrasound During Advanced Life Support - A Prospective Clinical StudyVille SalmensuuNo ratings yet
- 3-Column Notes 1. What? 2. So What? 3. Now What?: Respiratory SystemDocument1 page3-Column Notes 1. What? 2. So What? 3. Now What?: Respiratory SystemalyssaNo ratings yet
- Physical Examination of The Respiratory SystemDocument11 pagesPhysical Examination of The Respiratory SystemMark CatabijanNo ratings yet
- Plan of Care Patient Independent-2 PDFDocument1 pagePlan of Care Patient Independent-2 PDFHilary AlvaradoNo ratings yet
- Lab Guide: Respiratory AssessmentDocument10 pagesLab Guide: Respiratory AssessmentDaisy MellaNo ratings yet
- Health AssessmentDocument35 pagesHealth AssessmentKm GaputanNo ratings yet
- Group 6 Group Case Study DONEDocument5 pagesGroup 6 Group Case Study DONEE.R.ONo ratings yet
- Steps of CPR ProcedureDocument8 pagesSteps of CPR ProcedureKrupa JyothirmaiNo ratings yet
- Seminars in Fetal & Neonatal Medicine: Steven M. Donn, Sunil K. SinhaDocument6 pagesSeminars in Fetal & Neonatal Medicine: Steven M. Donn, Sunil K. SinhadeniNo ratings yet
- High Resolution and High Definition Anorectal ManometryFrom EverandHigh Resolution and High Definition Anorectal ManometryMassimo BelliniNo ratings yet
- 019 - Ulil Chiqmatuss'diah - KMB 1Document4 pages019 - Ulil Chiqmatuss'diah - KMB 1Setiaty PandiaNo ratings yet
- 019 - Ulil Chiqmatussa'diah - EPN 2 - Assessment On Respiratory Problems..Document7 pages019 - Ulil Chiqmatussa'diah - EPN 2 - Assessment On Respiratory Problems..Setiaty PandiaNo ratings yet
- Simple East Asian Landscape Campaign - by SlidesgoDocument54 pagesSimple East Asian Landscape Campaign - by SlidesgoSetiaty PandiaNo ratings yet
- Jurnal KMB Diva - 015Document10 pagesJurnal KMB Diva - 015Setiaty PandiaNo ratings yet
- 4927 20042 1 PBDocument7 pages4927 20042 1 PBSetiaty PandiaNo ratings yet
- Qi Muslimah Talk 1 Ivana FixDocument16 pagesQi Muslimah Talk 1 Ivana FixSetiaty PandiaNo ratings yet
- Patient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentDocument5 pagesPatient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentSetiaty PandiaNo ratings yet
- 1385 FullDocument10 pages1385 FullSetiaty PandiaNo ratings yet
- Patient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentDocument5 pagesPatient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentSetiaty PandiaNo ratings yet
- Hubungan Tingkat Kecemasan Dengan Tingkat Kemandirian Activities of Daily Living Pada LansiaDocument8 pagesHubungan Tingkat Kecemasan Dengan Tingkat Kemandirian Activities of Daily Living Pada LansiaSetiaty PandiaNo ratings yet
- JCM 10 00522 v2Document12 pagesJCM 10 00522 v2Setiaty PandiaNo ratings yet
- Impact of Osteoarthritis On Activities of Daily LiDocument9 pagesImpact of Osteoarthritis On Activities of Daily LiSetiaty PandiaNo ratings yet
- Alat Ukur Untuk Menilai Kemampuan Fungsional Pasien Dengan Osteoartritis Lutut: Tinjauan PustakaDocument6 pagesAlat Ukur Untuk Menilai Kemampuan Fungsional Pasien Dengan Osteoartritis Lutut: Tinjauan PustakaSetiaty PandiaNo ratings yet
- Reike DIyah Setiawati - 042 - PSIK ADocument28 pagesReike DIyah Setiawati - 042 - PSIK ASetiaty PandiaNo ratings yet
- Health and Quality of Life OutcomesDocument8 pagesHealth and Quality of Life OutcomesSetiaty PandiaNo ratings yet
- Progress in Disaster Science: Jeremy Spoon, Drew Gerkey, Ram B. Chhetri, Alisa Rai, Umesh Basnet, Chelsea E. HunterDocument15 pagesProgress in Disaster Science: Jeremy Spoon, Drew Gerkey, Ram B. Chhetri, Alisa Rai, Umesh Basnet, Chelsea E. HunterSetiaty PandiaNo ratings yet
- Vital Signs and Monitoring - Podcast - IntermediateDocument4 pagesVital Signs and Monitoring - Podcast - IntermediateSetiaty PandiaNo ratings yet
- Material - Using Equipment For Patients' Examination - 019 - Ulil ChiqmatussadiahDocument2 pagesMaterial - Using Equipment For Patients' Examination - 019 - Ulil ChiqmatussadiahSetiaty PandiaNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Terjadinya PreeklampsiaDocument13 pagesFaktor-Faktor Yang Berhubungan Dengan Terjadinya PreeklampsiaSetiaty PandiaNo ratings yet
- Consulatation Liaison Psychiatry English Lecture 2012 10Document58 pagesConsulatation Liaison Psychiatry English Lecture 2012 10Setiaty PandiaNo ratings yet
- 116-Article Text-415-1-10-20190507Document8 pages116-Article Text-415-1-10-20190507Setiaty PandiaNo ratings yet
- Alasan Dilakukannya 4 Kali Amandemen Uud 1945 Tujuan Dan Sejarah PerkembanganDocument11 pagesAlasan Dilakukannya 4 Kali Amandemen Uud 1945 Tujuan Dan Sejarah PerkembanganSetiaty PandiaNo ratings yet
- Deteksi Mycobacterium Tuberculosis Pada Sampel Sputum Menggunakan Teknik Loop-Mediated Isothermal Amplification (LAMP-TB)Document7 pagesDeteksi Mycobacterium Tuberculosis Pada Sampel Sputum Menggunakan Teknik Loop-Mediated Isothermal Amplification (LAMP-TB)Setiaty PandiaNo ratings yet
- Management of Lymphatic Malformations in ChildrenDocument8 pagesManagement of Lymphatic Malformations in ChildrenAyuRosemeiliaDewiNo ratings yet
- Adrenaline (Anaethesia Tutorial of The Week)Document8 pagesAdrenaline (Anaethesia Tutorial of The Week)Raisa AriesthaNo ratings yet
- VenoferDocument13 pagesVenoferLuciano H.Vivas M.No ratings yet
- Rizal FinalsDocument9 pagesRizal FinalsAnonymous 5DiMa95W100% (1)
- Hankin - 1998 - Development of Depression From Preadolescence To AdulthoodDocument13 pagesHankin - 1998 - Development of Depression From Preadolescence To AdulthoodHanni JuhaszNo ratings yet
- Post Cardiac Arrest CareDocument28 pagesPost Cardiac Arrest CareAkib ArmanNo ratings yet
- Migraine Diagnosis and TreatmentDocument19 pagesMigraine Diagnosis and TreatmentMagdalila Pua RosalesNo ratings yet
- Kindergarten RhymesDocument15 pagesKindergarten RhymesAkshit R Shah100% (1)
- Public Health Laws: Romeo R. Andaya, MD, MSCPD, PHD, Fpafp Chair, DPMCH Uph-DjgtmuDocument8 pagesPublic Health Laws: Romeo R. Andaya, MD, MSCPD, PHD, Fpafp Chair, DPMCH Uph-DjgtmuKatNo ratings yet
- PhilHealth - ClaimForm2 1Document2 pagesPhilHealth - ClaimForm2 1Harold Kirby TanNo ratings yet
- Warfarin Mechanism of Action, Indications AtfDocument4 pagesWarfarin Mechanism of Action, Indications AtfAmir mohammad moori MohammadiNo ratings yet
- Craig Sims, Dana Weber, Chris Johnson - A Guide To Pediatric Anesthesia (2020, Springer International Publishing)Document535 pagesCraig Sims, Dana Weber, Chris Johnson - A Guide To Pediatric Anesthesia (2020, Springer International Publishing)cheechengNo ratings yet
- Medical Surgical Skills Checklist PDFDocument5 pagesMedical Surgical Skills Checklist PDFHussain R Al-MidaniNo ratings yet
- MHS MRI Consent FormDocument1 pageMHS MRI Consent Formjulia sabadellNo ratings yet
- Chapter 1: Introduction To Operative DentistryDocument11 pagesChapter 1: Introduction To Operative DentistryMariam AdnanNo ratings yet
- Anti-Drug Essay Writing Competition 2011 Full DocumentDocument13 pagesAnti-Drug Essay Writing Competition 2011 Full DocumentqueenklNo ratings yet
- A Field Manual of Camel Diseases Traditional and Modern Health Care For The DromedaryDocument273 pagesA Field Manual of Camel Diseases Traditional and Modern Health Care For The DromedaryHenrique100% (3)
- 6BI01 01R Que 20130521Document24 pages6BI01 01R Que 20130521karan79No ratings yet
- Case Study: Cushing and AddisonDocument4 pagesCase Study: Cushing and AddisonJeff ValdezNo ratings yet
- A Case of Pica On A 6-Year-Old Child From MedanDocument3 pagesA Case of Pica On A 6-Year-Old Child From MedanatikahnurhNo ratings yet
- LVS Chronic Pain WsDocument49 pagesLVS Chronic Pain WsdtncorreoNo ratings yet
- Daftar Pustaka ReferatDocument2 pagesDaftar Pustaka ReferatBetharlitha PurLikaNo ratings yet
- Captain of The Ship DoctrineDocument3 pagesCaptain of The Ship DoctrineAllison CuevasNo ratings yet
- BPPV - Benign Paroxysmal Positional VertigoDocument7 pagesBPPV - Benign Paroxysmal Positional VertigoYaser BarrawazNo ratings yet
- Eye HXDocument2 pagesEye HXAnishilNo ratings yet
- Dursch SmithDocument2 pagesDursch Smithapi-708256548No ratings yet
- Approved: Tertiary HospitalsDocument26 pagesApproved: Tertiary Hospitalsmurtada gubaNo ratings yet
- Nursing Care For Child With Autoimmune Diseases & GI DisordersDocument4 pagesNursing Care For Child With Autoimmune Diseases & GI Disordersbunso padillaNo ratings yet
- Nursingcrib Com NURSING CARE PLAN Spontaneous AbortionDocument2 pagesNursingcrib Com NURSING CARE PLAN Spontaneous AbortionMina RacadioNo ratings yet