Download as pdf or txt
You might also like
- 2018 Article 288Document10 pages2018 Article 288dhimas permanaNo ratings yet
- Iuchi 2014Document6 pagesIuchi 2014Dian GbligNo ratings yet
- Effectiveness and Adverse Drug Reactions of Levetiracetam and Midazolam in Refractory Neonatal Seizure: A Cross Sectional Comparative StudyDocument6 pagesEffectiveness and Adverse Drug Reactions of Levetiracetam and Midazolam in Refractory Neonatal Seizure: A Cross Sectional Comparative StudySultan Rahmat SeptianNo ratings yet
- Comparative Efficacy of Intravenous Levetiracetam and Phenytoin in Status Epilepticus - A Systematic Review and Meta-Analysis of Randomized Controlled TrialsDocument7 pagesComparative Efficacy of Intravenous Levetiracetam and Phenytoin in Status Epilepticus - A Systematic Review and Meta-Analysis of Randomized Controlled TrialsBenazier Marcella BesmayaNo ratings yet
- FocusDocument8 pagesFocussri noviyanty yusufNo ratings yet
- 1 s2.0 S2214751921003066 Main 1Document8 pages1 s2.0 S2214751921003066 Main 1Gustavo PiñeroNo ratings yet
- Medicine: Risk Factors For Drug-Resistant EpilepsyDocument12 pagesMedicine: Risk Factors For Drug-Resistant EpilepsyyutomoNo ratings yet
- Strokeaha 118 024380Document5 pagesStrokeaha 118 024380Yi-Sung TsaiNo ratings yet
- Hongliang Mao Short and Long Term Response of VagusDocument16 pagesHongliang Mao Short and Long Term Response of VagusArbey Aponte PuertoNo ratings yet
- Atik Jurnal Nicu 1950695Document17 pagesAtik Jurnal Nicu 1950695atikNo ratings yet
- Comparative Cognitive Effects of Levetiracetam and Topiramate in Intractable EpilepsyDocument6 pagesComparative Cognitive Effects of Levetiracetam and Topiramate in Intractable EpilepsyDHIVYANo ratings yet
- Etomidate and General Anesthesia: The Butterfly Effect?: Matthieu Legrand, MD, PHD and Benoît Plaud, MD, PHDDocument3 pagesEtomidate and General Anesthesia: The Butterfly Effect?: Matthieu Legrand, MD, PHD and Benoît Plaud, MD, PHDOussamaBàidjiNo ratings yet
- 157 - Clinical Trials Adverse Events ChaDocument6 pages157 - Clinical Trials Adverse Events ChaWoo Rin ParkNo ratings yet
- 1071 (23337) PDFDocument4 pages1071 (23337) PDFNimesha WarnakulasooriyaNo ratings yet
- Head Trauma: V. B ( ), P. H ( ) and J. Fr. B ( )Document9 pagesHead Trauma: V. B ( ), P. H ( ) and J. Fr. B ( )Yudi PrasetyoNo ratings yet
- Etanercept in Alzheimer Disease: A Randomized, Placebo-Controlled, Double-Blind, Phase 2 TrialDocument8 pagesEtanercept in Alzheimer Disease: A Randomized, Placebo-Controlled, Double-Blind, Phase 2 TrialGiuseppe AcanforaNo ratings yet
- Ana 86 203Document12 pagesAna 86 203bozasnachoNo ratings yet
- Jurnal 3Document8 pagesJurnal 3Nendi feby valentinaNo ratings yet
- Gajjar B M Et. Al., 2016Document6 pagesGajjar B M Et. Al., 2016kaniNo ratings yet
- tsr1501 42Document10 pagestsr1501 42cah bagusNo ratings yet
- Urrent Eview: Prophylactic Anticonvulsants After NeurosurgeryDocument3 pagesUrrent Eview: Prophylactic Anticonvulsants After NeurosurgeryPulseWangminNo ratings yet
- Atonic Seizures in Children Meta AnalysisDocument9 pagesAtonic Seizures in Children Meta AnalysisRavi ChandraNo ratings yet
- Low-Dose Fentanyl Propofol Midazolam Ketamine andDocument5 pagesLow-Dose Fentanyl Propofol Midazolam Ketamine andDendy AgusNo ratings yet
- Journal Pone 0276012Document15 pagesJournal Pone 0276012hardi adiyatmaNo ratings yet
- Neuro in The ICUDocument4 pagesNeuro in The ICUEduardo GarciaNo ratings yet
- Jamaneurology Goeldlin 2024 Oi 240029 1716459699.82356Document10 pagesJamaneurology Goeldlin 2024 Oi 240029 1716459699.82356QueniNo ratings yet
- Grosse-Sundrup2012 Score PredictifDocument2 pagesGrosse-Sundrup2012 Score PredictifZinar PehlivanNo ratings yet
- PICpediatricDocument14 pagesPICpediatricAtzi FNo ratings yet
- Pi Is 0196064407016721Document3 pagesPi Is 0196064407016721abdulNo ratings yet
- Risk Factors For Seizures and Epilepsy in Children With Congenital Heart DiseaseDocument6 pagesRisk Factors For Seizures and Epilepsy in Children With Congenital Heart DiseaseclaudyNo ratings yet
- Clinical Management of Seizures in Newborns: Diagnosis and TreatmentDocument10 pagesClinical Management of Seizures in Newborns: Diagnosis and TreatmentfitriNo ratings yet
- Translet cts1Document5 pagesTranslet cts1HasvianNo ratings yet
- Ann EmergDocument8 pagesAnn EmergDyan TonyNo ratings yet
- Levetiracetam in Refractory Pediatric EpilepsyDocument11 pagesLevetiracetam in Refractory Pediatric EpilepsyAdlinaNo ratings yet
- Neurocognitive Radiation LalDocument7 pagesNeurocognitive Radiation Lalkmarmol77No ratings yet
- Drugs For Behavior Disorders After Traumatic Brain Injury - SystematicDocument16 pagesDrugs For Behavior Disorders After Traumatic Brain Injury - SystematicAlejandro GueudetNo ratings yet
- Advocating For Demonstration of Disease Modification - Have We Been Approaching Clinical Trials in Early Alzheimer Disease Incorrectly?Document2 pagesAdvocating For Demonstration of Disease Modification - Have We Been Approaching Clinical Trials in Early Alzheimer Disease Incorrectly?Lorrane NevesNo ratings yet
- Meyfroidt-Smith2019 Article FocusOnDeliriumSedationAndNeurDocument3 pagesMeyfroidt-Smith2019 Article FocusOnDeliriumSedationAndNeurmedicnanaNo ratings yet
- AsianJNeurosurg1341096-3791748 103157Document5 pagesAsianJNeurosurg1341096-3791748 103157Wahyu DarmaNo ratings yet
- Levetiracetam For Status Epilepticus - A Systematic ReviewDocument8 pagesLevetiracetam For Status Epilepticus - A Systematic ReviewBenazier Marcella BesmayaNo ratings yet
- Side-Effects Associated With Ketamine Use in DepressionDocument14 pagesSide-Effects Associated With Ketamine Use in Depression賀立安No ratings yet
- Long Term Outcomes of Status Epilepticus: A Critical AssessmentDocument15 pagesLong Term Outcomes of Status Epilepticus: A Critical AssessmentnafamaulidinaNo ratings yet
- Clinical Characteristics and Prognostic Factors of Children With Anti-N-Methyl-D-Aspartate Receptor EncephalitisDocument9 pagesClinical Characteristics and Prognostic Factors of Children With Anti-N-Methyl-D-Aspartate Receptor EncephalitisSara IsabelNo ratings yet
- Jurnal Anes 3Document10 pagesJurnal Anes 3Ari SamadNo ratings yet
- Interventions For Treatment of Poststroke Depression (AAFP 2023)Document2 pagesInterventions For Treatment of Poststroke Depression (AAFP 2023)Breno Resende Rodrigues CunhaNo ratings yet
- NIH Public Access: Management of Pediatric Status EpilepticusDocument16 pagesNIH Public Access: Management of Pediatric Status EpilepticusDiego CedamanosNo ratings yet
- Medi 97 E10919Document4 pagesMedi 97 E10919oktaviaNo ratings yet
- Jurnal Clinical L OutcomeDocument14 pagesJurnal Clinical L OutcomeaesunnitheticNo ratings yet
- Adherence To Antiepileptic Drugs and Seizure Control Among Patients With EpilepsyDocument6 pagesAdherence To Antiepileptic Drugs and Seizure Control Among Patients With EpilepsydewicahyadiNo ratings yet
- Bell 'S Palsy: Clinical and Neurophysiologic Predictors of RecoveryDocument5 pagesBell 'S Palsy: Clinical and Neurophysiologic Predictors of RecoveryMarsya Yulinesia LoppiesNo ratings yet
- Sedative Effects of Antihistamines: Safety, Performance, Learning, and Quality of LifeDocument17 pagesSedative Effects of Antihistamines: Safety, Performance, Learning, and Quality of Lifesaurabhvij82No ratings yet
- Validation of Chinese Version of The Morisky Medication Adherence Scale in Patients With EpilepsyDocument5 pagesValidation of Chinese Version of The Morisky Medication Adherence Scale in Patients With EpilepsyAndres RamirezNo ratings yet
- HIPOTERMIA EN TCE. Estudio POLAR 2018Document15 pagesHIPOTERMIA EN TCE. Estudio POLAR 2018Miguel Angel Velaz DomínguezNo ratings yet
- Epo EhiDocument12 pagesEpo EhiUriel MartzNo ratings yet
- Jurnal Tumor OtakDocument6 pagesJurnal Tumor OtakJaehyun JungNo ratings yet
- PIIS1059131122002151Document9 pagesPIIS1059131122002151Francisco XicohtencatlNo ratings yet
- Antipsychotics For Preventing Delirium in Hospitalized AdultsDocument12 pagesAntipsychotics For Preventing Delirium in Hospitalized AdultsLuis CsrNo ratings yet
- Autoimmune Encephalitis Proposed Recommendations For Symptomatic and Long-Term ManagementDocument11 pagesAutoimmune Encephalitis Proposed Recommendations For Symptomatic and Long-Term ManagementhazalsariyildizNo ratings yet
- Early Postoperative Seizures EPS in Patients UnderDocument11 pagesEarly Postoperative Seizures EPS in Patients UnderSri Eka HandayaniNo ratings yet
- Integrative Headache Medicine: An Evidence-Based Guide for CliniciansFrom EverandIntegrative Headache Medicine: An Evidence-Based Guide for CliniciansLauren R. NatbonyNo ratings yet
- Bipolar Disorders and Carbamazepine PharmacokinetiDocument5 pagesBipolar Disorders and Carbamazepine PharmacokinetiAgr YuroNo ratings yet
- Wk17 Cancers of The BloodDocument46 pagesWk17 Cancers of The BloodPotato PceeNo ratings yet
- Endocrine System Prepared By: Prof. Mike Chavez RN, USRNDocument7 pagesEndocrine System Prepared By: Prof. Mike Chavez RN, USRNMeiJoyFlamianoIINo ratings yet
- Illegal and Legal Substance Abuse Amongst Harm Reduction Program Users - A Case Study From CroatiaDocument18 pagesIllegal and Legal Substance Abuse Amongst Harm Reduction Program Users - A Case Study From CroatiamarijaNo ratings yet
- Drug Delivery and Targeting Parenteral RouteDocument8 pagesDrug Delivery and Targeting Parenteral Routehafiz patahNo ratings yet
- Jurnal PolyneuropatiDocument11 pagesJurnal PolyneuropatiMeutia Siti ZaharaNo ratings yet
- VI Sem. Nov. - 2022Document26 pagesVI Sem. Nov. - 2022Dhananjay KhadeNo ratings yet
- Drug Study (Pedia)Document7 pagesDrug Study (Pedia)Caurrine Monsalud100% (1)
- Successfull Treatment of Dermatophytosis With Combination of Itraconazole and IsotretinoinDocument5 pagesSuccessfull Treatment of Dermatophytosis With Combination of Itraconazole and IsotretinoinAlfaNo ratings yet
- Herbal Drugs For The Treatment of Polycystic Ovary Syndrome (Pcos) and Its ComplicationsDocument9 pagesHerbal Drugs For The Treatment of Polycystic Ovary Syndrome (Pcos) and Its ComplicationsDoc MailNo ratings yet
- List of Look-Alike MedicationsDocument5 pagesList of Look-Alike MedicationsAhmad TaramsyNo ratings yet
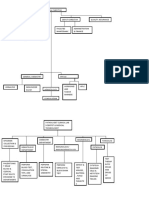
- Organizational ChartDocument5 pagesOrganizational ChartAlondra AranNo ratings yet
- Sodium and PotassiumDocument7 pagesSodium and PotassiumLUALHATI VILLASNo ratings yet
- Chemical and Therapeutic IncompatibilitiesDocument34 pagesChemical and Therapeutic IncompatibilitiesAlyssa Marie Petonio BialaNo ratings yet
- 4.fisiologi KardiovaskularDocument41 pages4.fisiologi Kardiovaskularrahmat feryadiNo ratings yet
- Drug Study - LithiumDocument3 pagesDrug Study - LithiumPRINCESS KOBAYASHINo ratings yet
- DOH AO No. 2020-0010 - Regulations On The Conduct of Clinical Trials For Investigational ProductsDocument55 pagesDOH AO No. 2020-0010 - Regulations On The Conduct of Clinical Trials For Investigational ProductsJonash MallariNo ratings yet
- Practical Research-Chapters 1-4 - Group 1-STEM DIAMONDDocument37 pagesPractical Research-Chapters 1-4 - Group 1-STEM DIAMONDArnoldTridanioOsioNo ratings yet
- Perencanaan Obat Non Ekat CTMDocument6 pagesPerencanaan Obat Non Ekat CTMArtyani Putri BintaNo ratings yet
- UP - Organic ChemistryDocument14 pagesUP - Organic ChemistryKate EvangelistaNo ratings yet
- Antimicrobial StewardshipDocument7 pagesAntimicrobial StewardshipMehwish MughalNo ratings yet
- Session 3 MEDICATION ADMINISTRATION (Summarized)Document10 pagesSession 3 MEDICATION ADMINISTRATION (Summarized)AlexandreaNo ratings yet
- Generic Name of MedicinesDocument87 pagesGeneric Name of Medicinesasgbalaji0% (1)
- Template Diglap LplpoDocument12 pagesTemplate Diglap LplpoNurul Elisa 'cHa'No ratings yet
- BMJ 22-09Document15 pagesBMJ 22-09Kiran ShahNo ratings yet
- (13384139 - Acta Medica Martiniana) Bronchial Asthma - Current Trends in TreatmentDocument9 pages(13384139 - Acta Medica Martiniana) Bronchial Asthma - Current Trends in TreatmentteuuuuNo ratings yet
- The Botanical and Chemical Distribution of Hallucinogens PDFDocument17 pagesThe Botanical and Chemical Distribution of Hallucinogens PDFJhasua Rebollar100% (2)
- Disorders of Na BalanceDocument24 pagesDisorders of Na BalanceElvis obajeNo ratings yet
- Group Iv Anions: - Distinguish by The Insolubility of Their Silver Salts in Acid SolutionDocument24 pagesGroup Iv Anions: - Distinguish by The Insolubility of Their Silver Salts in Acid SolutionSherwin OrdinariaNo ratings yet
- قائمة الادوية 2024مDocument686 pagesقائمة الادوية 2024مArabic CalligrapherNo ratings yet